Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
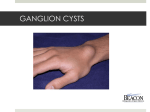
Arch Cardiovasc Imaging. 2016 August; 4(3):e45736. Published online 2016 August 28. doi: 10.5812/acvi.45736. Case Report Huge Pericardial Cyst with Compressing Effects on the Right-Heart Chambers Mehmet Onur Omaygenc,1,* Ibrahim Oguz Karaca,1 Beytullah Cakal,1 Haci Murat Gunes,1 Filiz Kizilirmak,1 and Bilal Boztosun1 1 Cardiology Department, Istanbul Medipol University Hospital, Istanbul, Turkey * Corresponding author: Mehmet Onur Omaygenc, Istanbul Medipol University Hospital, Cardiology Department, TEM Otoyolu Goztepe Cikisi No:1, 34214 Bagcilar, Istanbul, Turkey. Tel: +90-2124607774; +90-5054424718, Fax: +90-2124607059, E-mail: [email protected]@medipol.edu.tr Received 2016 July 02; Revised 2016 July 30; Accepted 2016 August 20. Abstract Introduction: Pericardial cysts are rare abnormalities of the mediastinum and generally have a benign course. Patients are mostly asymptomatic, and diagnosis is established incidentally in a majority of cases. The management of this asymptomatic population is also controversial. Case Report: We report a huge pericardial cyst, located at the right cardiophrenic angle impairing ventricular filling properties without causing evident symptoms. The cyst was almost 13 cm in the largest diameter. Echocardiography and computed tomography scan were utilized not only to confirm the diagnosis, but also to determine the treatment strategy. Conclusions: Surgical or percutaneous interventional treatment for pericardial cysts might be occasionally necessary, depending on the location of the cyst and its relationship with the adjacent structures. Unfortunately, our patient refused any kind of treatment option. Based on this report, the course of the disease, diagnostic modalities, and treatment strategies in general manner were additionally discussed. Keywords: Mediastinal Cyst, Pericardial Cyst, Pericardial Fluid 1. Introduction Pericardial cysts are rare abnormalities of the mediastinum and generally have a benign course. Patients are mostly asymptomatic unless major anatomic structures are compressed or rupture of the cyst occurs. Unfortunately, the management of this rare situation is controversial. The presence of large or gradually enlarging cysts and suspicion for a diagnosis other than a benign cyst might necessitate therapeutic intervention (1, 2). 2. Case Report A 42-year-old man was admitted to our outpatient clinic with mild exertional dyspnea. He was a heavy smoker and had a previous history of coronary stent implantation. He did not report a recent chest trauma. In his physical examination, the heart sounds were almost inaudible and the respiratory sounds were markedly reduced with rhonchi in all the lung fields. Chest X-ray, aside from pulmonary parenchymal abnormal findings, demonstrated a mass adjacent to the right ventricle (Figure 1A). ECG was normal, and the treadmill stress test result did not reveal significant myocardial ischemia. In echocardiographic examination, a large cystic structure compressing not only the right atrium but also the right ventricular base was observed in the apical and subcostal views (Video 1, Video 2, and Figure 1B). A significant respiratory variation was detected in the tricuspid in-flow Doppler recordings. The mitral in-flow was also affected, mainly due to impaired right ventricular filling. Accordingly, an undulation in preload and a slight ventricular interdependence were established (Figure 1C). The left ventricular volumes and functions were preserved. The inferior vena cava collapse during inspiration was within normal limits. Multislice computed tomography (CT) scan confirmed the diagnosis. A contrast-free cyst (127 × 68 × 100 mm), adjacent to the right-heart chambers, was detected. (Figure 1D). The cyst was located in the pericardial cavity, and the contents were postulated to be in fluid density (9 HU). Diffuse paraseptal and centrilobular emphysematous regions, pleuroparenchymal bands, and nodular lesions were also noticed in the pulmonary parenchymal sections. Apart from these, neither altered levels of serum inflammatory markers or serologic tests nor abnormal imaging data consistent with echinococcosis or tuberculosis were detected. The patient was consulted by the local heart team and Copyright © 2016, Iranian Society of Echocardiography. This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/) which permits copy and redistribute the material just in noncommercial usages, provided the original work is properly cited. Onur Omaygenc M et al. due to the huge size of the cyst and reduced filling properties, a consensus on the necessity of surgical or percutaneous intervention was achieved. Unfortunately, he refused these treatment options. At the 6th month’s visit, no symptom progression was observed and the echocardiographic findings were similar. 3. Discussion Pericardial cysts are considerably rare, with an overall incidence of 1 in 100,000 patients, and constitute 6% of all mediastinal masses (3). In line with this statement and to the best of our knowledge, approximately 25 striking cases and literature reviews have been published and cited in conventional citation indices since 2001 (1, 4, 5). These cysts are usually unilocular, well-delineated spaces encapsulated by a fibrous wall which is lined with mesothelium. The cavity is filled with a clear fluid. The most common locations of these benign cysts are both (mainly right) cardiophrenic angles (1, 2, 4). Most of these lesions range between 1 and 5 cm in diameter, but rarely cysts measuring over 20 cm have also been reported in the literature (4). Pericardial cysts are almost invariably located at the middle mediastinum. Aside from lymphoma, various benign cysts like bronchogenic, enteric, and rarely thymic cysts can be counted in the differential diagnosis. Cardiac or mediastinal hydatid cysts may also cause confusion. Calcification of the cyst wall and characteristic imaging properties such as floating membranes and daughter cysts may help distinguish them from other primary mediastinal masses (4, 6). In our patient, we did not observe any radiologic appearance consistent with echinococcosis inside the cavity. The inflammatory markers were within the normal limits, and the serum analysis for specific antibodies was also negative. Meanwhile, concomitant presence of tuberculosis was investigated and relevant biochemical and radiologic evidence was not observed. As for the exclusion of major differential diagnoses, the cyst was conclusively defined as a gradually expanding congenital cyst. Patients with pericardial cysts are generally asymptomatic, and the diagnosis is established incidentally in a majority of cases. Nevertheless, dyspnea, palpitations, and persistent cough may exist as initial symptoms. Hemoptysis, syncope, and fever are uncommon presentations and might indicate a local complication. Cyst rupture, cardiac tamponade, congestive heart failure, atrial fibrillation, right ventricular outflow tract obstruction, and obstruction of the right main bronchus can be considered possible complications at a glance (1, 2, 4). In our patient, mild symptoms and pulmonary auscultation findings necessitated a chest X-ray and diagnostic workup was started 2 Figure 1. A, Elliptical Mass is Seen Adjacent to the Right Ventricle (Arrows); B, Pericardial Cyst is Demonstrated by Transthoracic Echocardiography in the Subcostal View (Star); C, Significant Respiratory Variation is Seen in Mitral In-Flow Doppler Recordings; D, A Contrast-Free Pericardial Cyst is Located at the Right Cardiophrenic Angle. henceforward. Retrospectively speaking, almost absent heart sounds on the right of the sternum might be associated with the localization of the cyst. However, on the left side, it should probably be interpreted as the solidification of the pulmonary parenchyma and the masking of roaring expiratory auscultation findings. The key point of the further investigation process is echocardiographic examination. Pericardial cysts are observed as echolucent spaces adjacent to the parietal pericardium. As was the case in our patient, due to the mass effect of the cyst, filling properties might be impaired (1, 3, 5). The definition of the actual size of the cyst and its relationship with the neighboring structures requires CT or magnetic resonance imaging (MRI) as the method of choice after a comprehensive echocardiographic examination. The cysts appear as thin-walled, usually unilocular and well-delineated homogeneous cavities. In MRI imaging, they have distinctive signal-intensity alterations in T1 and T2 weighted sequences. Pericardial cysts fail to display contrast enhancement in both methods, and this condition helps distinguish these lesions from other pericardial disorders (1, 3). Our case absolutely met these features, and the localization of the cyst was typical. Since probable alternative pathologic conditions were unlikely, a congenital pericardial cyst was the definitive diagnosis. The management strategy vis-a-vis pericardial cysts is based on symptomatology. Asymptomatic patients can be followed up by serial echocardiographic e examinations. However, extensive cyst size, compression of the adjacent structures, and suspicion of a solid component may raise the need for intervention. Percutaneous aspiration is the 1st-line treatment for appropriate cases. In case of recurrence or possible malignant disease, surgical resection (thoracotomy or video-assisted thoracoscopic surgery) is required (1-3). It is mandatory to note that recommendations regarding the diagnostic process and treatment algorithms Arch Cardiovasc Imaging. 2016; 4(3):e45736. Onur Omaygenc M et al. mainly rely upon large case series and literature reviews. Thus, the management of asymptomatic or mildly symptomatic patients is still a matter for debate and more evidence is required particularly as regards follow-up data on those with bulky masses. Footnotes Authors’ Contribution: Mehmet Onur Omaygenc: corresponding author; Ibrahim Oguz Karaca: language editing, data collection; Beytullah Cakal: patient follow-up, formation of figures; Haci Murat Gunes: data collection; Filiz Kizilirmak: structural editing; Bilal Boztosun: senior author. Conflict of Interest: None. Financial Disclosure: None. Arch Cardiovasc Imaging. 2016; 4(3):e45736. References 1. Najib MQ, Chaliki HP, Raizada A, Ganji JL, Panse PM, Click RL. Symptomatic pericardial cyst: a case series. Eur J Echocardiogr. 2011;12(11):E43. doi: 10.1093/ejechocard/jer160. [PubMed: 21900299]. 2. Celik T, Firtina S, Bugan B, Sahin MA, Ors F, Iyisoy A. A giant pericardial cyst in an unusual localization. Cardiol J. 2012;19(3):317–9. [PubMed: 22641553]. 3. Adler Y, Charron P, Imazio M, Badano L, Baron-Esquivias G, Bogaert J, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2015;36(42):2921–64. doi: 10.1093/eurheartj/ehv318. [PubMed: 26320112]. 4. Hekmat M, Ghaderi H, Tatari H, Arjmand Shabestari A, Mirjafari SA. Giant Pericardial Cyst: A Case Report and Review of Literature. Iran J Radiol. 2016;13(1):ee21921. doi: 10.5812/iranjradiol.21921. [PubMed: 27110336]. 5. Islas F, de Agustin JA, Gomez de Diego JJ, Olmos C, Ferrera C, Luaces M, et al. Giant pericardial cyst compressing the heart. J Am Coll Cardiol. 2013;62(10):ee19. doi: 10.1016/j.jacc.2013.02.102. [PubMed: 23850918]. 6. Odev K, Aribas BK, Nayman A, Aribas OK, Altinok T, Kucukapan A. Imaging of Cystic and Cyst-like Lesions of the Mediastinum with Pathologic Correlation. J Clin Imaging Sci. 2012;2:33. doi: 10.4103/2156-7514.97750. [PubMed: 22919547]. 3