Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
LITHUANIAN UNIVERSITY OF HEALTH SCIENCES
MEDICAL ACADEMY
Ingrida Mockutė
THE EFFECT OF MATERNAL
THYROID FUNCTION AND EMOTIONAL
STATE DURING PREGNANCY
ON NEWBORN THYROID STIMULATING
HORMONE CONCENTRATION AND
ANTHROPOMETRIC MEASUREMENTS
Doctoral Dissertation
Biomedical Sciences, Medicine (07 B)
Kaunas, 2011
Dissertation prepared at the Department of Obstetrics and Gynecology and
the Institute of Psychophysiology and Rehabilitation, Lithuanian University
of Health Sciences, Medical Academy, during 2006–2011
Scientific Supervisor
Assoc. Prof. Dr. Eimantas Švedas
(Lithuanian University of Health Sciences, Medical Academy, Biomedical Sciences, Medicine – 07 B)
Consultant
Dr. Habil. Robertas Bunevičius
(Lithuanian University of Health Sciences, Medical Academy, Biomedical Sciences, Medicine – 07 B)
2
CONTENT
CONTENT .................................................................................................... 3
LIST OF ABBREVIATIONS ..................................................................... 5
LIST OF ORIGINAL PUBLICATIONS ................................................... 7
INTRODUCTION ........................................................................................ 8
AIM AND OBJECTIVES ......................................................................... 13
1. REVIEW OF LITERATURE ............................................................... 15
1.1. Maternal thyroid function tests ..................................................... 15
1.1.1. Physiology basics on the thyroid functions regulations ........ 15
1.1.2. Changes in TSH and FT4 values during pregnancy ............. 16
1.1.3. Thyroid function tests and changes in different
measurement techniques ................................................................... 18
1.1.5. Thyroperoxidase antibodies effect on thyroid axis
hormones and pregnancy outcomes ................................................. 24
1.1.6. Thyroid function screening controversies in pregnancy ...... 26
1.2. The importance of the newborn thyroid stimulating hormone .. 27
1.2.1. The fetal thyroid development and function ......................... 27
1.2.2. Iodine deficiency assessement by the newborn thyroid
stimulating hormone .......................................................................... 28
1.2.3. The newborn thyroid stimulating hormone concentrations
in relation to maternal age and gestation at birth........................... 31
1.2.4. Influence of delivery factors on newborn blood spot TSH
concentrations..................................................................................... 32
1.3. Maternal psychological factors and thyroid function tests
during pregnancy interference with newborn TSH and
anthropometric parameters .................................................................. 33
1.3.1. Maternal thyroid axis parameters repercussions with
newborn TSH...................................................................................... 33
1.3.2. Antenatal maternal mental state and thyroid axis function
interference with anthropometric characteristics of the newborn 34
2. MATERIAL AND METHODS............................................................. 38
2.1. Study population ............................................................................. 38
2.2. Methods ............................................................................................ 41
2.3. Statistical analyses........................................................................... 44
3. RESULTS ............................................................................................... 48
3.1. Maternal thyroid function tests during pregnancy (Study I) ..... 48
3.1.1. Reference intervals for thyroid testing at each trimester
of pregnancy ....................................................................................... 48
3
3.1.2. Trimester changes in concentration of TSH and FT4
during pregnancy ............................................................................... 49
3.1.3. Effect of thyroid peroxidase antibodies on thyroid
stimulating hormone reference limits ............................................... 57
3.2. The newborn thyroid stimulating hormone (Study II, III) ......... 57
3.2.1. Iodine deficiency assessed by the newborn TSH
concentrations (Study II) ................................................................... 61
3.2.2. The newborn TSH levels in relation to maternal age,
gestation, birthweight and gender (Study III) ................................. 61
3.2.3. The newborn TSH levels in relation to maternal thyroid
function................................................................................................ 63
3.3. Maternal thyroid function during pregnancy in the
interference with anthropometric parameters of newborn ................ 65
3.4. Antenatal maternal personality and mental state and
anthropometric characteristics of the newborns (Study IV, V) ......... 69
4. DISCUSSION ......................................................................................... 74
4.1. Longitudinaly assessed maternal thyroid axis changes during
pregnancy and comparisons of reference intervals............................. 74
4.2. Iodine deficiency assessed by the newborn thyroid stimulating
hormone concentrations ........................................................................ 80
4.3. The newborn thyroid stimulating hormone levels in relation
to maternal age, gestation, birth weight and gender ........................... 82
4.4. Delivery mode impact on newborn thyroid stimulating
hormone concentrations ........................................................................ 85
4.5. Antenatal maternal mental state and anthropometric
characteristics of newborns ................................................................... 86
CONCLUSIONS ........................................................................................ 93
SCIENTIFIC SIGNIFICANCE OF THE STUDY ................................. 94
PRACTICAL RECOMMENDATIONS .................................................. 95
ACKNOWLEDGEMENTS ....................................................................... 96
REFERENCE LIST ................................................................................... 98
PUBLICATIONS ON THE DISSERTATION THEME ...................... 128
ANNEXES ................................................................................................. 129
4
LIST OF ABBREVIATIONS
AACE
AITD
ANOVA
ATA
BFPI
BMI
β, Beta
CH
CI
DSM–III–R
–
–
–
–
–
–
–
–
–
–
EDS
ETA
FT3
FT4
F-test
hCG
HPA
ICCIDD
–
–
–
–
–
–
–
–
IDD
IDDM
K-S
LATS
NACB
NTDs
PPSS
–
–
–
–
–
–
–
PPT
p–value
r
R2
RIA
SD
Sig.
STAI
T3
T3RU
–
–
–
–
–
–
–
–
–
–
American Association of Clinical Endocrinologists
Autoimmune thyroid disease
Analysis of variance
American Thyroid Association
Big Five Personality Inventory
Body Mass Index
Standardised regression coefficient
Congenital hypothyroidism
Confidence Interval
The Diagnostic and Statistical Manual of Mental
Disorders, third edition, revised
Edinburgh Depression Scale
European Thyroid Association
Free triiodothyronine
Free thyroxine
To test if two population variances are equal
Human chorionic gondotropin
Hypothalamo-pituitary-adrenal axis
International Council for Control of Iodine Deficiency Disorders
Iodine Deficiency Disorder
Insulin–dependent diabetes mellitus
Kolmogorov–Smirnov test
Latin American Thyroid Society
The National Association of Clinical Biochemistry
Neural tube defects
Axis IV criteria of the Perceived Psychosocial Stress
Scale
Postpartum thyroiditis
Probability value
Coefficient of Correlation
Coefficient of Determination
Radioimmunoassay
Standard deviation
Significance level
State Trait Anxiety Inventor
Triiodothyronine
T3 resin uptake
5
TBG
TES
THBI
THBR
ТFT
TPO
TPO-Ab
TRH
TSH
t–test
TTR
UI
UNICEF
WHO
–
–
–
–
–
–
–
–
–
–
–
–
–
–
–
Serum thyroxine binding globulin
The Endocrine Society
Thyroid hormone-binding index
Thyroid hormone-binding ratio
Тhyroid function tests
Thyroid peroxidase
Thyroid peroxidase antibodies
Thyroid stimulating hormone releasing hormone
Thyroid stimulating hormone, thyrotrophin
Statistical hypothesis test
Serum transthyretin
Urinary iodine
United Nations Children‘s Fund
The World Health Organisation
The degree of association
6
LIST OF ORIGINAL PUBLICATIONS
This thesis is based on the following original publications that are
referred to in the text by the
Roman numerals I – IV.
I. Mockutė I, Švedas E, Raškauskienė N, Mickuvienė N, Pop VJ,
Bunevičius R. Thyroid function tests during pregnancy: a
longitudinal study in the area of compensated mild iodine
deficiency. Acta Obstetricia et Gynecologica Scandinavica. 2011.
Under review.
II. Mockutė, Ingrida; Raškauskienė, Nijolė; Kusminskas, Laima;
Švedas, Eimantas. Iodine deficiency assessed by the newborn
thyrotropin concentration = Jodo stygiaus įvertinimas pagal
naujagimių tireotropinio hormono kiekį // Lietuvos akušerija ir
ginekologija = Lithuanian obstetrics & gynecology 2010, t. 13,
Nr. 2, p. 131–136.
III. Mockutė, Ingrida; Švedas, Eimantas; Raškauskienė, Nijolė;
Mickuvienė, Narseta; Bunevičius, Robertas. The newborn thyroid
stimulating hormone levels in relation to maternal age and
gestation at birth = Naujagimio tirostimuliuojančio hormono
ryšys su motinos amžiumi bei nėštumo trukme // Lietuvos
akušerija ir ginekologija = Lithuanian obstetrics & gynecology
2010, t. 13, Nr. 3, p. 278–284.
IV. Bunevičius A, Čėsnaitė E, Mockutė I, Kusminskas L, Bunevičius
R. Antenatal maternal mental state and anthropometric
characteristics of the newborns: I. Impact of symptoms of
depression
and
anxiety.
Biologinė
psichiatrija
ir
psichofarmakologija 2007; 9(1):3–6.
V. Bunevičius A, Kusminskas L, Mockutė I, Bunevičius R Antenatal
maternal state and anthropometric characteristics of the
newborns: II. Impact of personality dimensions and stress.
Biologinė psichiatrija ir psichofarmakologija 2007; 9(2):35–38
The original papers in this thesis have been reproduced with the
permissions of the publishers.
7
INTRODUCTION
The issue of thyroid disease and dysfunction during pregnancy has been
an important research development in recent years (1-2). Pregnancy may
affect the course of thyroid disorders and, conversely, thyroid diseases may
affect the course of pregnancy. Moreover, thyroid disorders and their management may affect both the pregnant woman and the developing fetus (3).
Additionally, certain psychological factors, such as stress, anxiety, depressive symptoms and disorder may affect the pregnant women, the course of
pregnancy and subsequently the newborn (4-6). Pregnancy could be called a
psychoendocrine challenge to the mother and developing fetus. Finally,
pregnant women may be under the care of multiple health care professionals, including obstetricians, endocrinologists, psychiatrists, nurse midwives,
family practitioners, internists solving pregnancy, thyroid and psychiatry
related issues in clinical practice, providing recommendations towards a
healthier and satisfied pregnancy with the primary aim of healthy mother
and child.
The prevalence of hypothyroidism during pregnancy is estimated to be
0.3–0.5% for overt hypothyroidism (OH) and 2–3% for subclinical hypothyroidism (SCH) (1-2, 7). Hyperthyroidism in pregnancy prevalence ranges
from 0.1% to 0.4% with Graves’ disease accounting for 85% of cases (8-9).
Isolated hypothyroxinemia has been described in approximately 2% of
pregnancies (10). Thyroid autoantibodies are found in 5–15% of women of
the childbearing age, and chronic autoimmune thyroiditis is the main cause
of hypothyroidism during pregnancy (11-14). Between 2.2% and 2.5% of
women have been found to have serum thyroid stimulating hormone (TSH)
levels of 6 mIU/L or greater at 15 to 18 weeks’ gestation (12, 14).
Impaired maternal thyroid hormone metabolism during pregnancy due to
dietary iodine deficiency or thyroid disease can affect the outcome of pregnancy, including miscarriage, preterm birth, preeclampsia, placental abruption, breech delivery, increased fetal mortality and impaired neurological
development of the child (10-12, 15-21). Thyroid hormone dysfunction also
interferes with ovulation and fertility (22-24). A sufficient thyroid function
is essential to ensure a healthy pregnancy and delivery. To facilitate our understanding of the pathologic processes that affect the thyroid gland during
pregnancy, it is important to understand normal physiologic processes that
take place in pregnant women, including changes in thyroid function tests
(25). There is no data on Lithuanian women thyroid axis hormone changes
throughout the pregnancy. Moreover, we need to clarify thyroid impairment
early in pregnancy for timely intervention (12, 14, 26). A proper assessment
8
of thyroid axis hormone concentrations plays an important role evaluating
thyroid function. Research studies have shown that early maternal thyroid
insufficiency, even subclinical hypothyroidism (elevated thyrotrophin
(TSH) with normal free thyroxine (FT4)) and isolated hypothyroxinemia
(normal TSH with lower FT4) have the potential to impair fetal neurodevelopment and delay childhood neurodevelopment (27-30). Increasing attention has therefore focused on the diagnosis and treatment of maternal thyroid dysfunction during pregnancy. Measurement of TSH and FT4 provides
the primary data for evaluating thyroid status, in particular cut-off values are
important for the upper TSH reference limit and for the lower FT4 reference
limit.
The issue of thyroid axis hormone changes during pregnancy has not
been addressed in Lithuanian women. Moreover, the thyroid hormone axis
reference intervals for thyroid function assessment have not been constructed for pregnant women in Lithuania. A precise thyroid function evaluation
is important not only in respect of maternal and fetal wellbeing, but more so
having in mind that Lithuania is still in a vulnerable state of insufficient iodine environment (31-33). Although in recent years the understanding of
thyroid physiology in pregnancy has improved, the interpretation of biochemical thyroid function tests can still be difficult. The wide variability in
the lower and upper euthyroid reference limits of thyroid axis related hormones is influenced by assays used to assess hormone concentrations, by
demographics of the population (ethnicity, age, sex), by iodine nutrition status, concomitant diseases, as well as by physiological conditions such as
starvation or pregnancy (1-2, 34). However, development of sensitive biochemical assays that measure TSH, FT4 and free tri-iodothyronine (FT3)
has improved our understanding of the gestation dependent changes of these
hormones. The trend of decrease in FT4 and FT3 levels and increase in TSH
values with advancing pregnancy is described in textbooks and review articles (35) and (36), yet gestation-specific reference ranges are rarely provided (2).
Some investigators have found FT4 concentrations (37) and TSH (38) to
fall below the limit of normal using newer assays. The 50% plasma volume
expansion in pregnancy, increase in thyroid binding globulin (TBG) production, the stimulatory effect of chorionic gonadotropin (hCG) and a relative
iodine deficiency mean that thyroid hormone reference interval for non–
pregnant women may not be appropriate in pregnancy (39). Therefore it was
proposed to consider that pregnancy should be viewed as an ‘environmental’ factor triggering thyroid machinery and inducing thyroid pathology, especially in areas with a marginally reduced dietary iodine intake. Thus, the
ranges of thyroid function tests should be not only trimester–specific but
9
presumably also geography–specific to account for the differences in ethnicity and iodine intake (2).
The majority of thyroid function assessing studies are based on cross–
sectional data, whereas longitudinal cohort studies addressing thyroid function during pregnancy are still lacking (40-41). Longitudinal in contrast to
cross–sectional studies give a better indication of what occurs in thyroid axis hormone secretion during pregnancy and how reference interval for these
hormones should be constructed. Therefore our study was constructed to
evaluate thyroid axis changes in pregnancy by longitudinal approach.
Only five countries in Europe, namely Austria, Finland, Norway, Sweden
and Switzerland had no iodine deficiency problem in 1993 but it continued
to persist in all other European countries, to some degree (42). In 2004, it
was estimated that 2 billion people worldwide were at risk of iodine deficiency and 20% were in the Eastern and Western Europe being both affected
(42-43). While cretinism, the most extreme expression of iodine deficiency,
has become very rare and even extinct in Europe, of considerably greater
concern are the more subtle degrees of mental impairment associated with
iodine deficiency that lead to poor school performance, reduced intellectual
ability, and impaired work capacity. Nevertheless, iodine deficiency is the
most preventable cause worldwide of preventable mental retardation (44).
On the basis of the national medians of urinary iodine (UI) for the 40 European countries included in the review by the World Health Organisation
(WHO) in 2007, it is estimated that the populations of 19 countries have adequate iodine nutrition, 12 have mild iodine deficiency, one country experiences moderate iodine deficiency, and eight countries have insufficient data
(42). Thyroid function comes into alteration when iodine intake falls below
75µg/d (45). This situation can occur in individuals in China, India, Indonesia, but also in some countries of Europe and the United States (45). It
makes the 50% decrease in iodine intake found in HANES III survey in the
United States worrisome (46). The same study observed a marked urinary
iodine decrease in pregnant women, compared with the earlier data (47).
Lithuanian National survey data presented in 1995, revealed 62% of population with UI less than 100 μg/L (42, 48). In addition, there is growing evidence that iodine deficiency has reappeared in some European countries
where it was thought to have been eliminated (31). Salt iodization remains
the recommended strategy for eliminating iodine deficiency as being the
most cost-effective (49). In May 2002 a Special session on Children of the
United Nations General Assembly (New York) endorsed the goal of iodine
deficiency disorder (IDD) elimination by the year 2005, signed by Lithuanian governors as well (42). Evaluation of pregnant women was carried out
only once in Lithuania between 1998 and 2000, before implementation of
10
mandatory salt iodisation program in the country (32, 50). As stated in
WHO report (42) monitoring of national programmes is currently insufficient, especially as it relates to measuring progress towards the goal of eliminating iodine deficiency. Therefore, it is important to evaluate the current
situation on iodine sufficiency in our country and the effect of the program
thereafter. Neonatal thyroid stimulating hormone (TSH) as an indicator appears to be a particularly sensitive tool in the evaluation of the iodine status
of a population and in the monitoring of iodine intervention programmes
(51). Thus within the same study on thyroid axis study in healthy pregnant
women, we analysed TSH levels of progeny, as an indicator of iodine sufficiency in the area.
There is a well-established relationship between alterations of various
hormonal systems and psychiatric disorders, both in endocrine and psychiatric patients (52). It is now widely accepted that thyroid hormone continues
to play a critical role in the adult brain, influencing mood and cognition,
although the details remain to be investigated (53). The relation between
depression and thyroid dysfunction or thyroid autoimmunity has been
documented not only in psychiatric (53-54) and general population (55-57),
but also in postpartum women (58-59). It was demonstarted that subclinical
hyperthyroidism increases the risk of depression in early pregnancy (60),
and low antenatal thyroid functioning in late preganancy is related to
postpartum depression (59). In our study, despite endocrinological thyroid
function measures, maternal personality traits and emotional state were continuosly monitored. Currently, the issue of mental heath assessment antenataly is broadly discussed (61). There are oppinions on benefits of screening
for depression in pregnancy and postpartum (62). Infants of depressed
mothers display delayed psychologic, cognitive, neurologic, and motor development (61, 63), as well as antenatal maternal stress and anxiety impacts
adverse pregnacy outcomes (64). Assessing women for psychosocial risk
factors and symptoms of distress during regular pregnancy follow-up gives
the opportunity to link women with appropriate interventions for
management.
Knowing, that intrauterine life is a challenging period for fetal development and an impared intrauterine environment affects the development of
future chronic diseases (65-67), birthweight could be called a marker of fetal
and newborn wellbeing or health. Therefore, our study evaluated maternal
psychoendocrine impact on the newborn anthropometry, since low birth
weight is associated with increased risk of mortality and morbidity of infants (68) and an overweigth - with increased complications in pregnacy and
prediction of metabolic outcomes in later life (69). Globally, 15.5% of all
births, or more than 20 million infants worldwide, are born with low birth11
weight. The level of low birthweight in developing countries (16.5%) is
more than double the level in developed regions (7%) (68). On the other
hand, there has been a rise in the prevalence of large newborns over a few
decades in many parts of the world. In 2010, around 43 million children under five were overweight. Once considered a high-income country problem,
overweight and obesity are now on the rise in low- and middle-income
countries. In 2008, 1.5 billion adults, 20 years and older, were overweight
(70). Birthweight is a strong indicator not only of maternal health and nutritional status, but also of the newborn's chances for survival, growth, longterm health and psychosocial development (71). Understanding the importance and the global scale of the birthweight issue, we analysed possible
factors accounting for the latter with the concern on maternal personality
traits and emotional state during pregnancy, as well as the impact of thyroid
function.
12
AIM AND OBJECTIVES
The aim of the research was to evaluate maternal thyroid axis hormone
and emotional state changes during pregnancy, to assess newborn thyroid
stimulating hormone concentration the third day after birth and determine
their interrelations and the effect on pregnancy outcomes.
The objectives of the study
1.
To determine trimester–specific reference intervals and evaluate the
effects of thyroid autoimmunity on thyroid stimulating hormone
and free thyroxine concentrations in different trimesters of pregnancy in the cohort of healthy pregnant women.
2.
To determine iodine deficiency using newborn thyroid stimulating
hormone screening data as an indirect method and maternal thyroid
function measures.
3.
To examine the relation between newborn thyroid stimulating hormone concentration and delivery outcomes and maternal thyroid
function during pregnancy.
4.
To evaluate the relation of maternal thyroid function, emotional
state and anthropometric characteristics of the newborns.
Scientific novelty of the study
The study was designed to assess longitudinally maternal thyroid axis
hormone changes during pregnancy and consecutively establish reference
intervals for TSH and FT4 in this study, which could be used for diagnosing
and monitoring thyroid disorders in pregnancy. Measurement of TSH and
FT4 provides the primary data for evaluating thyroid status. Since, published reference interval data are limited and absolute reference limits vary,
clinical laboratories frequently use only insufficiently approved reference
intervals given by the manufacturers of commercially available assays. The
current worldwide disscusions of reliable reference intervals for thyroid
function tests in pregnancy, stimulated to present our data on healthy pregnant women in Lithuania. Variables that affect the setting of TSH and FT4
reference intervals, in particular manufacturer’s methodology and iodine
status, are discussed in this paper.
This study addresses the iodine sufficiency issue on the basis of newborn
thyroid stimulating hormone. The effectiveness of the salt iodisation program and the achievement of the goal of IDD elimination by the year 2005,
13
signed by the Lithuanian governors at the United Nations General Assembly
(New York) is referred to in this manuscript.
Moreover, our present study demonstrates the strongest predictors alterating newborn thyroid stimulating hormone and anthropometric parameters in
relation to certain maternal pshychological factors together with maternal
thyroid axis hormones throughout different time points in pregnancy.
Finally, our longitudinally designed research study gives a better understanding of the complex maternal–fetal interaction related to the ongoing
complex physiological thyroid processes and psychoemotional aspects during pregnancy.
14
1. REVIEW OF LITERATURE
1.1. Maternal thyroid function tests
1.1.1. Physiology basics on the thyroid functions regulations
The TSH-releasing hormone (TRH), pyroglutamyl-histadyl-prolinamide,
is synthesized in anterior hypothalamic neurons and released in the region of
the median eminence. Circulating down the neurohypophyseal portal plexus, TRH binds to cell membrane receptors on anterior pituitary thyrotropes
and causes production and release of TSH. The number of TRH receptors is
in part regulated by T3 nuclear receptor occupancy. High T3 nuclear receptor occupancy is associated with reduced TRH receptor numbers.
TSH, a glycoprotein, is composed of alpha and beta chains linked by
sulfhydryl bonds. The alpha chain is common to TSH, luteinizing hormone,
follicle stimulating hormone, and human chorionic gonadotropin while the
beta chain is unique to each. Hormonal production of the thyroid gland is
constituted of thyroxine (T4) (80%) and triiodothyronine (T3) (20%). TSH
interacts with plasma membrane receptor, which leads to endocytosis of colloid followed by fusion of the endocytic vacuole with intracellular lysosomes, which leads to digestion of the contained thyroglobulin and release
of bound T4 and T3. In the circulation, whole T4 originates from thyroid
secretion but most of T3 (80%) is produced extrathyroidally from T4 deiodination. Conversion of T4 to T3 may be influenced by various conditions
and circulating T3 is a less reliable reflection of thyroid hormone production
than T4. T4 and T3 enter the circulation and reversibly bind to circulating
proteins, the most important of which is TBG, an inter-alpha-globulin, as
two thirds of the T4 is carried by TBG. In pregnancy, the proportion of circulating T4 carried by increased levels of TBG is even greater, in excess of
75% (23). Other thyroxine binding proteins are transthyretin (TTR) and albumin. The circulating levels of both serum albumin and TTR remain stable, with only a slight tendency to decrease near the end of gestation, mainly
as a result of hemodilution due to the increased vascular pool (72). TBG has
the highest affinity for the iodothyronines, thus both T4 and T3 are tightly
bound (73). The unbound T4 enters cells and is deiodinated by three enzymes at one of two potential sites. Removal of carbon 5' iodine from the
outer ring of T4 by type I deiodinase, forms T3 (74). There is a preferential
secretion of T3 by the thyroid gland during pregnancy, under direct influence of TSH (23). Type II deiodinase increases for maintaining T3 produc-
15
tion in placenta, when availability of T4 decreases. Placenta also contains
type III deiodinase, which converts T4 to reverse T3 and T3 to T2 (75).
Secretion of the thyroid hormones T4 and T3 is regulated by pituitary
TSH. TSH secretion, in turn, is controlled through negative feedback by
thyroid hormones. There is a negative log-linear relationship between serum
free T4 and TSH concentrations (76). This means that very small changes in
serum free T4 concentrations induce very large reciprocal changes in serum
TSH concentrations (76). As a result, thyroid function is best assessed by
measuring serum TSH, assuming steady state conditions in the absence of
pituitary or hypothalamic disease. It follows that high TSH and low FT4 is
characteristic of hypothyroidism and low TSH and high FT4 is characteristic of hyperthyroidism (77).
1.1.2. Changes in TSH and FT4 values during pregnancy
The normal thyroid function is essential for successful fetal development,
maternal morbidity and well–being of the child. Complex physiologic
changes take place during pregnancy, which tend together to modify the metabolism of the thyroid and have a variable impact at different time points
during gestation.
Pregnancy is accompanied by alterations in the thyroid function because
of the rise in human chorionic gondotropin (hCG) and the stimulatory effects of estrogen on thyroid binding globulin (TBG) synthesis. In early gestation hCG has two antagonistic effects on thyroid economy, tending to
lower FT4 after the rapid increase in serum TBG, and to increase FT4
through its specific thyroid-stimulating action (45). The structural homology
between hCG and TSH molecules has a direct stimulatory effect of hCG on
thyrocytes. Respectively, that induces a small and transient increase in free
thyroxine levels near the end of the 1st trimester (peak circulating hCG)
and, in turn, a partial TSH suppression during normal pregnancy (23, 78).
The rise in serum FT4 is proportional to peak hCG values, subsequently
TSH nadir mirrors the rise of hCG concentrations (78). The peak rise in
hCG and the nadir in serum TSH occur together at about 10-12 weeks of
gestation. During the first trimester in approximately 20 % of healthy pregnant women, serum TSH values may be transiently lowered to subnormal
values (23, 78-81). Serum TSH levels return progressively to the normal
range, starting in the second trimester (82). Thereas, free thyroid hormone
concetrations start decreasing during the second and third pregnancy trimesters (23, 83).
The increase in total serum T4 and T3 concentrations in the first trimester
of pregnancy rise to levels about 1.5 fold those of nonpregnant women that
16
occurs due to an increase in serum TBG concentrations (45). Due to stimulatory estrogen effects, TBG production in liver increases, and also due to
reduced plasma clearance of TBG (84), stabilization of TBG molecule, prolonged half-life due to salylation processes (23), consequently, TBG concentrations start to increase early in pregnancy and, by 16–20 weeks of gestation, have doubled (23, 78). In order to maintain unaltered FT4 levels, increase in TBG secretion is followed by increasing sintesis and diminished
degradation of total T4, until a new homeostasis is reached. This is achieved
during pregnancy by ~50% increase in thyroid hormone production (3, 85).
The requirement for increased total T4 secretion, increases iodine requirements during pregnancy (45). In addition to an increase in serum TBG, the
modest decreases in both TTR and albumin are commonly found in pregnancy, but the physiological impact of these changes is unknown (86).
In regions with the iodine supply borderline or low, the situation is clearly different, thus significant changes occur during pregnancy (23, 78, 87). In
iodine sufficient conditions, the physiologic FT4 decrement that is observed
during the second and third trimester remains minimal (~10%) (88), whereas it is, enhanced (~20–25%) in iodine deficient nutritional conditions (78).
Iodine insufficiency revealed by pregnancy explains the progressive increase in serum TSH observed after 16 weeks of gestation (23).
The physiological changes that take place in maternal thyroid economy
lead to an increase in thyroid hormone production of ~50% above preconception baseline hormone production. Moreover, renal iodide clearance
augments significantly due to an increased glomerular filtration rate in the
first weeks of gestation and persists thereafter (23, 45). Furthermore, iodine
deprivation for the mother continues later in gestation from the passage of a
part of the available iodine from maternal circulation to the fetal–placental
unit (89). Hence, when iodine deprivation exists during the first half of gestation, it tends to become more severe in the final stages (3). A limited
availability of iodine during pregnancy presents an additional challenge to
the thyroid gland when hormone requirements are increased. In order to
achieve the necessary increment in thyroid hormone production, the iodine
intake needs to be increased during early pregnancy. In addition, maternal
iodine intake must be increased to supply the requirements of the fetal thyroid during the second and third trimesters (45).
In the nonpregnant condition an adequate iodine intake is estimated to be
100–150 μg/d (23). When women with an iodine intake of <100 μg/d become pregnant, the pregnancies are frequently associated with thyroid function abnormalities, mainly maternal hypothyroxinemia, resulting in excessive thyroidal stimulation and goiter formation in both the mother and the
child (90-94). Thus, WHO Technical Consultation held in 2005 proposed
17
the daily recommended nutrient intake (RNI) for iodine during pregnancy
and breastfeeding should range between 200 and 300 μg/d, with an average
of 250 μg/d (95). Moreover, when salt restriction is prescribed, it is highly
recommended to monitor serum TSH changes and provide supplements of
iodine during pregnancy (94). Furthermore, a recent study showed that in
addition to consumption of iodisated salt, pregnant women should take iodine supplements throughout pregnancy (96). It was proposed to consider
that pregnancy should be viewed as an ‘environmental’ factor triggering the
thyroid machinery and, in turn, inducing thyroid pathology in areas with a
marginally reduced iodine intake (3). In clinical practice, iodine restriction
is presented by relative hypothyroxinemia (T4/TBG), an elevated total
T3/T4 molar ratio, and an increase in serum thyroglobulin and progressively
increasing TSH levels, after nadir in the first trimester (3).
1.1.3. Thyroid function tests and changes in different measurement
techniques
Nowadays, when the sensitivity and specificity of TSH assays have improved, it is recognised that the serum TSH measurement offers better sensitivity for detecting thyroid dysfunction compared to FT4 testing (97).
Variables such as age, gender, race, and season, phase of menstrual cycle, cigarette smoking, exercise, fasting or phlebotomy-induced stasis have
minor effects on the reference intervals for thyroid tests in adult outpatient
(2, 98-99). Thus recently, an approach to adopt age, gender, and ethnicity
specific thyrotropin reference limits in population was proposed by United
States researchers (100).
Serum TSH concentration is determined by immunoassay methodology.
Depending on the type of label attached to the TSH antibody, the assay is
variously called immunoradiometric, immunofluorimetric, immunochemiluminometric, or immunoenzymometric. Published sensitivities of the various assays range from 0.004 to 0.6 mIU/L (101).
First generation TSH radioimmunoassays had detection limits of about 1
mIU/L. Since the normal range for serum TSH is about 0.4 to 5.0 mIU/L,
these assays were useful for the diagnosis of primary hypothyroidism (as
serum TSH concentrations are appropriately elevated), but were not sufficiently sensitive to distinguish between normal serum TSH concentrations
and the low serum TSH concentrations present in most patients with hyperthyroidism.
Second generation TSH immunometric assays have detection limits of
about 0.1 mIU/L. These assays can be used as screening tests to distinguish
hyperthyroidism from euthyroidism and hypothyroidism (102). However,
18
since the range of subnormal TSH measurement is very limited, values near
or at the detection limit do not distinguish the degree of hyperthyroidism,
and poor quality control in many laboratories can lead to erroneous values
(103).
Third generation TSH chemiluminometric assays, currently in wide use,
have detection limits of about 0.01 mIU/L. They can therefore provide detectable TSH measurements even in mild hyperthyroidism (104). In order to
detect reliable values of serum TSH in the hyperthyroid range, one needs a
third generation assay with a functional sensitivity of at least ≤0.05 mIU/L
(105).
TSH assay characteristics depend on the reagents, protocols, and technical performance of the assay (106). High-quality laboratories should have
intraassay variation of less than 5% for TSH in the range of 1.0–4.5
mIU/Liter. Fewer data are available concerning interassay variation in TSH
concentration performed on the same sample; still it should be less than
10% (105, 107-109). Thus, in appropriately calibrated assays, a single TSH
determination should reasonably reflect the TSH concentration in that sample (77).
There is a linear inverse relationship between FT4 and log-linear of the
serum TSH, making the serum TSH consentration a very sensitive indicator
of the thyroid state in patients with an intact hypothalamic-pituitary axis
(45, 108). Mildly elevated serum TSH concentrations in euthyroid individuals are caused by circulating TSH variants of decreased biological potency
(110) and TSH resistance syndromes (111-113) or in a subclinical hypothyroidism. Spurious TSH elevations due to assay interference can also occur
with circulating heterophilic antibodies (114-116) or antimouse IgG (117118).
Serum total T4 is usually measured by radioimmunoassay (RIA), chemiluminometric assay, or similar immunometric technique. Most of serum T4
is bound to TBG, transthyretin (also called thyroxine-binding prealbumin),
or albumin. Serum total T4 assays measure both bound and unbound
("free") T4. Normal ranges vary among laboratories; a typical range is 4.6 to
11.2 μg/dL (60 to 145 nmol/L) (98). Serum T3 is also measured by RIA,
chemiluminometric assay or other immunometric assay. T3 is less tightly
bound to TBG and transthyretin, but more tightly bound to albumin than T4.
The normal range is even more variable among laboratories than for total
T4; a typical range is approximately 75 to 195 ng/dL (1.1 to 3 nmol/L) (98).
Four different tests have been used to estimate the free T4: equilibrium
dialysis, "direct" free hormone measurements, calculating the free hormone
index by using the thyroid hormone-binding ratio or index (THBR or THBI)
via measurement of the T3 resin uptake (T3RU), and calculating the ratio of
19
total thyroid hormone to TBG levels (119). Because none of these methods
measure FT4 directly, guidelines suggest that these methods should be
named "free T4 estimate tests" (120).
Current approaches to free T4 measurement are vulnerable to several
method-dependent artifacts: abnormal albumin binding of T4 or of the assay
tracer, the inhibition of T4 binding to TBG by medications, and the effects
of critical illness, especially in heparin-treated patients, pregnancy, and the
abnormalities in sick premature infants (98). Because of systematic variation
between methods (whether a technique is albumin dependent or prone to
incubation or dilution artifacts), it is essential to consider methodological
details when evaluating free T4 estimates in aforementioned situations
(121).
Equilibrium dialysis/RIA is considered as the reference methods for free
thyroid hormone measurements (122-123). Routine clinical laboratories use
automated direct two-step or one-step immunoassays with a high molecular
weight ligand or labelled antibody (124). Nevertheless, FT4 measurements
are still vulnerable to method-dependent artefacts in particular population
such as patients with renal failure and pregnant women (124). In general,
two-step labeled hormone back titration methods are less subjected to artifacts due to abnormal binding proteins, changes in albumin, TBG than onestep hormone analogue methods (125).
Free T4 assays frequently fail to meet performance standards in pregnant
patients (126), especially when they are performed using one-step procedure
(45). To compensate this, some kits have provided different normal ranges
for pregnant patients, usually lower than those of non-pregnant patients. It
has been suggested that total T4 measurements are more reliable during
pregnancy, but the normal pregnant range for T4 is higher than that of nonpregnant patients due to TBG excess. Total T4 levels during pregnancy are
1.5-fold higher than in non-pregnant women (83). Serum TSH concentrations are not subjected to these measurement difficulties.
The T3RU is used as an indirect measure of serum thyroid hormone
binding capacity, and the FT4 index (FT4I), derived from the T4 and T3RU,
for correct estimates of T4 for serum binding abnormalities (101). The FT4
index based on the T3RU test shows only small fluctuations in pregnancy,
while the index based on the T4/TBG ratio shows significantly lower values
than those found in nonpregnant women (23).
There are narrow individual variations in thyroid hormone test values,
with data suggesting that each individual has a genetically determined FT4
set-point (108). When thyroid status is stable and hypothalamic-pituitary
function is intact, serum TSH measurement is more sensitive than FT4 for
detecting mild (subclinical) thyroid hormone excess or deficiency in relation
20
to an individual’s genetic free T4 set-point (77). Serum FT4 measurement is
a more reliable indicator of thyroid status than TSH when thyroid status is
unstable (77).
1.1.4. Reference interval for thyroid function tests in pregnancy
Presently, there is a controversy over the type of thyroid hormone measurement that represents the most reliable interval to differentiate normal thyroid function from abnormalities associated with subtle thyroid dysfunction
during pregnancy (3).
A topic of active debate rose when improvements in serum TSH assays
led to better a definition of the lower limit of the reference range, for a
healthy population (127). Most laboratories have used upper limit of normal
for serum TSH of about 4.5 to 5.0 mIU/L. Guidelines proposed by the National Association of Clinical Biochemistry (NACB) have stated that in the
future the upper limit of the serum TSH euthyroid reference range is likely
to be reduced to 2.5 mIU/L for all adults, because more than 95% of
screened normal euthyroid volunteers had serum TSH values between 0.4
and 2.5 mIU/L (120). However, a population study in Germany, which excluded patients with a positive family history, goiter, nodules, or positive
TPO-Ab antibodies, found a normal reference range from 0.3 to 3.63 mIU/L
(128). Previous studies in America have estimated that lowering the threshold from 4.5 to 2.5 mIU/L would identify an additional 9.7% patients, representing 20.6 million, with subclinical hypothyroid if the upper TSH limit
decreased; the majority of them do not have thyroid disease (106).
Presently, a controversy exists as whether patients with serum TSH values between 5 to 10 mIU/L require treatment. For individuals with a serum
TSH of 5–10 mIU/L, there is an increased risk of progression to overt hypothyroidism. The risk (129) is estimated to be 2.6% per year in the absence of
TPO-Ab and 4.3% per year in TPO-Ab presence. After 20 years, overt hypothyroidism developed in 33% of patients with mildly raised TSH and in
55% of similar patients who also had TPO-Ab (129). Limited history data
are available for individuals with serum TSH between 2.5 and 5.0 mIU/L.
Surks et al. (106) obtained data for rates of progression to overt hypothyroidism for such patients from the Whickham study. When serum TSH was
between 3.0 and 5.0 mIU/Liter in adults 20–40 years of age, the probability
of developing hypothyroidism in 20 years was less than 10%, whereas when
TPO-Ab were present, the prevalence in 20 years, increased to 15–30%.
However, the American Association of Clinical Endocrinologists
(AACE), the American Thyroid Association (ATA) and Endocrine Society
(TES) (1) consensus panel has continued to recommend that 4.5 mIU/L be
21
maintained as the upper limit of normal, reasoning that although some individuals within the range of 2.6–4.5 mIU/L may have subclinical thyroid disease, there is a lack of evidence of adverse outcome in this group (130).
Pregnancy - related thyroid function changes lately rose debates on proper evaluation of thyroid axis hormones throughout pregnancy (2). NACB
recommends that ‘trimester-specific reference intervals should be used when
reporting thyroid test values in pregnant women (120). Though, it has been
suggested that until trimester-specific and method-specific reference ranges
are established, an upper limit for TSH in pregnant women of 2.5 mIU/L
(compared with 4.0–4.5 mIU/L in non-pregnant women) should be adopted
(131). For women with clinical hypothyroidism anticipating pregnancy, new
guidelines from TES recommend that optimal preconception levels of TSH
should be <2.5 IU/L (1).
NACB states that initiation of levothyroxine (L-T4) therapy should be
considered if the serum TSH level is >4.0mIU/L in the first trimester of
pregnancy (77). They further recommend that if overt hypothyroidism is
diagnosed during pregnancy, thyroxine doses should be rapidly titrated to
reach and thereafter maintain serum TSH concentrations of <2.5 mIU/Liter
in the first trimester (or 3 mIU/ liter in second and third trimesters) or to
trimester-specific normal TSH ranges (of <2.3, <3.1, and <3.5 for the first,
second, and third trimesters, respectively) (1). Although routine screening
was not recommended, the earlier AACE, ATA, TES consensus group (97)
had recommended L-T4 replacement to restore serum TSH to the reference
range in pregnant women found by case finding to have subclinical hypothyroidism (normal free T4 with TSH above the upper limit of normal) (97).
However, it is recognized that the supporting evidence is insufficient, and
such recommendations are largely based on expert consensus (132).
If one uses total T4 to estimate thyroid function, it is therefore reasonable
to adapt the non pregnant reference range by multiplying this range by 1.5
starting from second half of the pregnancy (133-134).
The reference ranges provided by the manufacturers of free thyroid hormone measurement kits have been established using pools of non pregnant
normal sera. Such reference ranges are no longer valid in the pregnant state
because the FT4 assays are influenced by the serum changes associated with
pregnancy. Therefore, it has been suggested to adapt serum FT4 reference
ranges to ‘laboratory–specific’ or ‘trimester–specific’ ranges for specific use
during pregnancy but, so far, no consensus has been reached worldwide on
such ‘pregnancy–adapted’ ranges, and it is recommended to remain cautious
in the interpretation of serum FT4 levels in pregnancy.
22
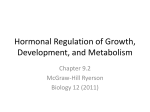
Figure 1.1. TSH changes during pregnancy. The graph shows median
values (in rectangle) versus the range of 2.5th and 97.5th percentiles (in
oval) for each trimester of pregnancy taken from eight studies of trimesterspecific TSH reference intervals, reported during 2004-2009, for women
without thyroid peroxidase autoantibodies, from iodine-sufficient populations. The dotted horizontal lines show the typical nonpregnant reference
range (0.4–4.1 mIU/L), (Adapted from: Glinoer, Spencer, 2010 (2)).
Similarly, reference ranges should be established for serum TSH levels
during pregnancy (81, 135-136). Gestation–specific reference intervals for
TSH could diminish the potential risk of misinterpretation of thyroid function tests in pregnancy (81, 120).
Figure 1.1 illustrates median TSH values and the 2.5th to 97.5th serum
TSH percentiles for each trimester of pregnancy, recalculated from eight
studies reported between 2004 and 2009 and carried out in women negative
for TPO-Ab, which were from iodine-sufficient population and confirms the
downward shift of serum TSH values during pregnancy (2).
Many factors, as has been mentioned, such as ethnicity, age, manufacturer’s methodology, iodine status and rigor for selection of the reference
population and calculation method may affect the establishment of reference
intervals for thyroid function tests (137-138). Reference intervals may need
to be gestational age specific and method specific, and other factors may
also need to be taken into account. Selection of normal subjects may account for variations in reference intervals by different authors, despite the
23
use of the same methodology for testing (137). Several studies have attempted to derive pregnancy-specific reference ranges for thyroid function
tests with inconsistent results (81, 135-136, 139-140), perhaps reflecting differences in iodine status between studies and, in some studies, the inclusion
of women with thyroid autoimmunity (81, 139).
The majority of thyroid function assessing studies are based on cross–
sectional data, however longitudinal studies addressing thyroid function during pregnancy are still lacking with respect to mild to moderate iodine–
deficient populations (40-41). Trimester–specific intervals are needed since
thyroid insufficiency may be associated with adverse obstetric outcome and
fetal neuro–developmental deficits (2, 25, 134).
Moreover, accurate assessment of thyroid function during pregnancy is
critical, for both the initiation of thyroid hormone therapy, and for the adjustment of thyroid hormone dose in those already receiving thyroid hormones. Knowledge about normal changes in thyroid hormone concentrations throughout pregnancy allows better individualized iodine supplementation and thus improved antenatal care. To interpret thyroid hormone tests
properly reliable and population–specific reference ranges during pregnancy
are needed, not least in land–locked populations where iodine intake may be
insufficient. Such situations can be found in most continents, including Europe. Longitudinal, as opposed to cross–sectional data will give a better indication of what occurs in this respect in pregnancy and how reference ranges should be constructed. No relevant up to date studies have been conducted with Lithuanian pregnant women.
1.1.5. Thyroperoxidase antibodies effect on thyroid axis hormones
and pregnancy outcomes
The maternal physiological changes that occur in normal pregnancy induce not only complex endocrine changes, but also an effect of the immune
responses (141). Antithyroid antibodies are classified as immunoglobulin G.
It is a heterogenous group of antibodies as there are antibodies against
TSH–receptor, against thyroid peroxidase and also against thyroglobulin
(142). Thyroid peroxidase (TPO), originally described as thyroid microsomal antigen, is present on the apical surface of thyroid follicular cells and is
the antigen involved in cell–mediated cytotoxicity (143). Pregnancy is a period in which the titres of antibodies decrease to protect fetus from abortion;
but just after delivery they increase again (142). The prevalence of autoimmune thyroid disease (AITD) in the pregnant population is comparable to
that found in the general female population with a similar age range, i.e. between 5–15% (144).
24
Women who are euthyroid but carry thyroid antibodies at the onset of
pregnancy have an increased risk of developing hypothyroidism during gestation (145). Forty to 60% of women with positive TPO–Ab in early pregnancy develop postpartum thyroid dysfunction, mainly postpartum thyroiditis (PPT) and Graves‘ disease after delivery (142, 146). Five percent of all
pregnant women and 25% of pregnant women with insulin-dependent diabetes mellitus develop PPT during the first year after delivery (147). PTT incidence is also affected by genetic influences (148), iodine intake (149), and
smoking (150).
In those studies where epidemiologic information is available on groups
of control women, the data show that thyroid autoimmunity is 5.2–fold more
frequent in women with a diagnosis of hypothyroidism, compared with euthyroid controls (mean of 48.5% versus 9.2%). Importantly, the prevalence
of thyroid antibodies in pregnant hypothyroid women depends on the severity of thyroid dysfunction (12).
Women with thyroid autoimmunity who are euthyroid in the early stages
of pregnancy are at risk of developing hypothyroidism and should be monitored for elevation of TSH above the normal range (1). The risk of progression to hypothyroidism could be predicted from serum TSH levels and
TPO–Ab titers measured in early pregnancy (23). When serum TSH is
above 2.5 mIU/L and/or TPO–Ab titers above 1250 U/mL before 20 weeks,
these markers are indicative to develop hypothyroidism by the end of pregnancy. In women with AITD, mean serum free T4 is not only significantly
lower than in controls, but in addition, is at the lower limit of normality
(89).
An increased risk of miscarriage, perinatal mortality, preterm delivery,
placental abruption, large for gestational age infants and maternal post partum thyroid disease have been reported in euthyroid women with positive
TPO-Ab concentrations (1-4)(143, 151-154). There is an association noticed
between clinical and subclinical hypothyroidism (SCH) and infertility. Female infertility was significantly associated with AITD without thyroid dysfunction (155). In a meta-analysis of four observational studies euthyroid
women with positive TPO-Ab undergoing assisted reproduction technologies had two-fold higher miscarriage rates that negative for TPO-Ab (156),
the same was observed by others (22, 156-157). Striking reductions in the
rates of miscarriage (by 75%) and premature delivery (by 69%) were reported among women with AITD who had received thyroxine supplementation
since early gestation and throughout pregnancy. Furthermore, thyroxine–
treated women with AITD maintained a euthyroid status, while FT4 decreased by 30% and TSH levels increased progressively during gestation in
the untreated group (4,7)(158-159). The authors concluded that the overall
25
risk of having a miscarriage was 3–fold to 5–fold greater in euthyroid women with AITD (154). Moreover, long-term morbidity of mothers with thyroid dysfunction or antibodies during early pregnancy seems to predict later
thyroid disease and pose a risk of diabetes (160-161).
The occurrence of stressful life events (marital disharmony, housing and
socioeconomic problems) and some biological factors (e.g. previous psychiatric illnesses) are strongly associated with postpartum depression. Some
authors also said that postpartum depression (60, 162) and postpartum psychosis (163) depend on the presence of antithyroid antibodies during pregnancy. It is believed that cytokines which are released during the autoimmune process can affect the central nervous system and can determine
changes in behaviour (142).
Moreover, recent data on the increased incidence of pregnancy loss in
pregnant women with TSH levels between 2.5 and 5.0 mIU/L provides
strong physiological evidence to support redefining the TSH upper limit of
normal in the first trimester to 2.5 mIU/L (164). Most pregnant women are
unlikely to know their antithyroid antibody status because universal screening is not routinely done. Although a positive association exists between the
presence of thyroid antibodies and pregnancy loss, universal screening for
antithyroid antibodies and possible treatment cannot be recommended at this
time (1). Whether thyroid hormones should be given prior to or during
pregnancy in euthyroid women with TPO-Ab remains controversial (165).
1.1.6. Thyroid function screening controversies in pregnancy
Establishment of thyroid axis hormone reference interval in pregnancy is
important having in mind another gately debatable issue – screening for thyroid dysfuncion in pregnancy. Given the prevalence and adverse outcomes
associated with maternal thyroid dysfunction, currently discussion has focused on the possibility that screening pregnant women for thyroid disease
could improve outcomes for both mother and child (12, 135). Currently,
universal screening in asymptomatic fertile patients is not endorsed by the
American College of Obstetrics and Gynecology (166), the US Preventative
Task Force (167), or TES (1). In contrast, the AACE recommends that TSH
be measured in women of childbearing age before pregnancy or in the first
trimester (168), and ATA recommends screening beginning at the age of 35
years and then every 5 years thereafter (97). In addition, a committee of six
members who had participated in a consensus statement group comprising
experts from AACE, ATA, and TES (97) independently proposed a position
stating that TSH testing ‘‘should be performed routinely during the prepregnancy evaluation or as soon as pregnancy is diagnosed’’ (169). Despite
26
these controversies, obtaining a serum TSH level for those with a history of
infertility and/or recurrent miscarriage is warranted (1). Opponents of
screening, however, suggest that aggressive case finding in pregnant women
is appropriate for identification of maternal thyroid dysfunction during
pregnancy (139, 170). Intrestingly, Vaidya et al. have reported that targeted
thyroid function testing of only pregnant women at high risk for thyroid disease (e.g. family history of thyroid disease) would miss about one third of
women with overt and subclinical thyroid disease (171).
Whatever approach is taken to identify thyroid dysfunction in pregnant
women, appropriate interpretation of thyroid function tests plays a critical
role in this process. As reference intervals for thyroid function tests in pregnant women can be significantly different from those in non-pregnant women, therefore construction of trimester-specific reference intervals are esssential.
1.2. The importance of the newborn thyroid stimulating hormone
1.2.1. The fetal thyroid development and function
Thyroid develops between the 2nd and 7th week of gestation. Between 8
and 11 weeks of gestation differenciation with follicle formation, concentration of iodine and formation of thyroxine occur, but full regulatory hypothalamic–pituitary–thyroid axis interactions are established between 12 and 18
weeks (172). At early gestational stages, the presence of thyroid hormones
in fetal structures can only be explained by transfer of maternal thyroid
hormones to the fetal compartment, because fetal production of thyroid
hormones does not become efficient until mid-gestation. Thyroid hormone
and specific nuclear receptors are found in fetal brain at 8 wk after conception (173). Thyroxine can be detected in amniotic fluid prior to the onset of
fetal thyroid function, indicating its maternal origin by transplacental transfer (173). Between 6 and 12 weeks of gestation, if maternal total T4 concentration is set to represent 100%, the total T4 concentration in the coelomic
fluid would represent 0.07% and T4 in the amniotic cavity as little as
0.0003–0.0013% of maternal total T4 concentrations (173). Fetus is solely
dependent on maternal thyroxine not only during early gestation (173-174),
but even after 12 weeks, thyroid hormone in fetus continues to be partly
supplied by mother (175). In utero, fetal T4 is converted to reverse triiodothyronine (rT3), not active form of T3. Just before birth a switch to T3 production occurs to faciliate extrauterine survival. In normal newborns, born
vaginally, there is a sharp increase in T3 and T4 levels 24–48 hours postpartum (45, 172). After delivery, the serum TSH levels in the newborn increas-
27
es sharply to peak at about 2 to 4 hours after birth, returning to its initial
value within 48 hours (45). This neonatal TSH surge is thought to occur in
delivery stress and response to rapid reduction in the environmental temperature after delivery (172). Moreover, the TSH surge is thought to contribute
to the enhancement of extrathyroid conversion of T4 to T3 by D1 or D2
(176) and adrenergic stimulation of the Dio2 gene (177). Thus, maternal
thyroid is extremely important source of thyroid hormones to ensure the adequate development of the fetal-maternal unit (30, 174, 178), both for trofoblast function and for normal fetal, with the concers of neurodevelopment
(174, 179). Therefore, understanding of maternal-fetal thyroid economies
are also covered in our research.
1.2.2. Iodine deficiency assessement by the newborn thyroid
stimulating hormone
Iodine is an essential micronutrient present in the human thyroid gland
and it is an essential component of the thyroid hormones, TT4 and TT3,
with iodine comprising 65% and 59% of their weights, respectively (42).
The normal function of the thyroid gland, also the tendency to develop abnormalities in thyroid gland function and structure, depend greatly on the
iodine intake of the subject (180-181). Iodine deficiency is one of the major
global public health problems leading to endemic cretinism, goiter and mental impairment (44, 182-183).
Thyroid hormones regulate metabolic processes in most cells, play a determining role in the process of early growth and development of most organs, especially that of the brain and central nervous system in humans from
the early gestation to the age of 3 years (28-29, 184-189). If iodine deficiency exists during this period and results in thyroid hormone deficiency, it
might impair the development of brain and central nervous system, continuously causing an irreversible mental retardation (44). It was estimated that
among the 1572 million people in the world exposed to iodine deficiency
(28.9 % of the world population) 11.2 million were affected by overt cretinism, the most extreme form of mental retardation due to the deficiency and
that another 43 million people were affected by some degree of mental impairment (174). Moreover, over 285 million school-age children worldwide
are iodine deficient (190).
An important epidemiological consideration is that the risk of iodine deprivation during pregnancy needs to be assessed locally and closely monitored over time, because mild to moderate iodine deficiency may occur in
areas that are not immediately recognized as iodine–deficient (3, 44). Another epidemiological concept should be considered that the iodine intake
28
may vary unexpectedly from one area to another within a given country.
This occurs often in regions with mild to moderate iodine deficiency, because of significant variations in the ‘natural’ iodine content of food and water (3, 191). Lithuania, although has a small territory, the iodine sufficiency
areas also vary from one region to other (32, 48, 192).
Recently it has been realized that even milder forms of iodine insufficiency could increase pregnancy loss, perinatal and infant mortality, neonatal hyperthyrotropinemia, neonatal hypothyroidism, growth retardation, and
intellectual disability (193). Elevated serum TSH in the newborn indicates
an insufficient supply of thyroid hormones to the developing brain (3). Congenital hypothyroidism (CH) ranges from 1 in 3000 to 1 in 4000 newborn
infants (15, 194) and is a common preventable cause of mental retardation.
An elevated TSH concentration in a newborn's blood is the earliest available
laboratory manifestation of CH. Owing to its superior specificity and sensitivity, TSH testing is preferred over thyroxine testing (195). Neonatal thyroid screening using TSH as the primary screening test detects not only
permanent sporadic CH, but also compensated or transient primary hypothyroidism, whose incidence can be as high as 1 in 10 newborns and whose
main cause is iodine deficiency (51). Detection of CH in Lithuania has started in 1993, later endorsed by the Lithuanian Ministry of Health in 2005 issued regulations Nr. V–865 on management the universal newborn screening for congenital metabolic diseases (196).
The World Health Organisation (WHO), International Council for Control of Iodine Deficiency Disorders (ICCIDD) and United Nations Children‘s Fund (UNICEF) suggested the use of neonatal TSH levels as one of
the indicators to assess iodine deficiency as the best indicator allowing prediction of possible impairment of mental development at the population level (197). Elevated neonatal TSH is a particularly sensitive tool in the evaluation of the iodine status of a population and in the monitoring of iodine supplementation programmes (51). Though, a recent study is concerned whether newborn TSH as a tool to assess the iodine status in populations is ideal
(96). Low iodine content of the thyroid of newborns follows by an accelerated turnover rate of their intrathyroidal iodine reserves. This turnover rate
is 1% in adults. It is 17% in the newborn in conditions of iodine repletion,
but is as high as 62% and 125% in conditions of moderate and severe iodine
deficiency, respectively (51). Such an accelerated turnover rate requires thyroid hyperstimulation, concequently followed by an increase in TSH of the
newborn (51).
According to the WHO recommendation, the frequency of an elevated
neonatal TSH of >5 mIU/L in whole blood (or 10 mIU/L serum) has to be
less than 3% in blood samples obtained from cord or after 3 days of age and
29
indicates iodine sufficiency in a population (31). The frequency of newborn
thyrotropin concentrations >5 mIU/L appears to be a sensitive indicator of
iodine nutrition during pregnancy as well (198). APIE REFERENC 32
Therefore, thyrotropin screening in newborns has been used to assess the
severity of iodine deficiency in populations (198-201). Table 1.2.2.1 gives
the indicators for assesing iodine status based on the guidelines of the WHO
and ICCIDD (190, 202).
Table 1.2.2.1. Epidemiologic criteria* for assessing severity of iodine deficiency based on whole–blood thyroid–stimulating hormone (TSH) levels
Severity of iodine deficiency
Indicator
TSH >5 mIU/L
(whole blood)
Target
Newborns
Severe
Moderate
Mild
Normal
≥ 40.0%
20.0–39.9%
3.0–19.9%
< 3.0%
*World Health Organization and the International Council for the Control of Iodine
Deficiency Disorders (WHO/ICCIDD) (190).
The agreed and commonly accepted strategy and the method applied for
the correction of iodine deficiency is universal salt iodization (USI) – the
addition of suitable amounts of potassium iodide (KI), potassium iodate
(KIO3) or sodium iodide to all salt for human and livestock consumption
(42). Potassium salts are the most frequently used. In 2003 the governmental
recommendations for use of iodized salt were introduced in Lithuania and
USI program was implemented in Lithuania under the regulatory rules Nr.
V–255 (50) by the order the Minister of Health of 22 April 2004. The Hygiene Norm on Hygiene for Foodstuffs was amended to includ that “all food
retail outlets, catering and bakery establishments shall use only iodized table
salt, containing 20–40 mg/kg iodine” effective from 1 January 2005.
The Institute of Medicine recommends a daily iodine intake of 220 μg
during pregnancy and 290 μg during lactation; the WHO recommends 250
μg of iodine daily for pregnant and lactating women (203). The ATA has
recommended that women receive prenatal vitamins containing 150 μg of
iodine daily during pregnancy and lactation (204). In practice, this requires
the administration of multivitamin pills designed specifically for pregnancy
purposes and containing iodine supplements (3). It should be remembered
that, because of the longstanding restriction in dietary iodine before the onset of pregnancy, a lag period of approximately one trimester is inevitable
before the benefits of iodine supplementation to improve thyroid function
can be observed (205-206).
30
In 2002 iodine consumption was assessed in Lithuanian population,
showing mean consumtion of 120.8 μg iodine per day (women - 104.4 μg).
Yet, women in cities consume just 96.7 μg iodine per day. Moreover, survey
by Lithuanian National Nutrition center in 2005 revealed that only 67% of
households are using iodised salt (207). Of the 40 countries reviewed by
WHO in the recent report, only nine have coverage of iodized salt at the
household level of at least 90% (42). According to WHO (203), Lithuania
belongs to the second category countries (between 20 and 90% of households using iodised salt; median urinary iodine between 20 μg/L and 100
μg/L). Therefore, the the WHO recommended the approach of giving iodine
supplement for pregnant and lactating women: as a daily oral dose of iodine
as potassium iodide, so that the total iodine intake is 250μg/d of iodine, either alone or combined with other minerals and vitamins or as a single annual oral dose of 400μg of iodine as iodised oil (203).
Thefore, the aim of this study was to determine TSH levels in newborns
and assess iodine deficiency issue of the implementation of USI program in
Lithuania by using neonatal TSH screening data as an indirect method.
1.2.3. The newborn thyroid stimulating hormone concentrations in
relation to maternal age and gestation at birth
There is known association between elevated TSH level in the newborn
and brain impairment, CH and other congenital malformations predominant
being cardiac, neural tube defects and dysmorphic features (208-210). From
the obstetrical point of view, the risk for congenital malformations and particularly chromosomal abnormalities increases with advanced maternal age.
The childbearing period in the reproductive life cycle is generally defined as
between the ages of 15 and 44 years in the studies (211). Maternal age as an
influencing factor on neonatal TSH levels is of particular interest, especially
recent decades, when the demography of parenting is changing due to delayed decisions to motherhood (212).
Neonatal screening TSH values may vary depending on the influence of
multiple methodological sample collection factors, including timing of specimen collection, the TSH assay and collection paper used (213). There are,
however, limited data available on perinatal factors potentially affecting neonatal blood spot TSH levels (214-216). Whether evaluation of TSH levels
in newborns is ordered as a screening test or in response to symptoms, the
understanding of confounding factors has to be further explored. Moreover,
it is important to identify newborn TSH levels effecting factors due to
emerging studies on new screening cut-off determination (217). Therefore,
our study examines the relationship between neonatal TSH levels and possi-
31
ble confounding factors such as maternal age, newborn birth weight, gestational age and gender. Since birth statistics over recent decades in Europe
shift in favour of delaying motherhood until thirties and beyond (212), it is
of interest to assess newborn TSH levels in relation to maternal age.
1.2.4. Influence of delivery factors on newborn blood spot TSH concentrations
Prior reports have indicated that concequencies of labor and delivery can
alter thyroid hormone function in mothers and infants at the time of delivery
(218-219). Several studies have demonstrated associations between mode of
delivery and measures of stress-related hormones measured in maternal
blood and umbilical cord blood (220-222). In response to stress, the production of hormones including epinephrine, norepinephrine, and cortisol is increased. These increases alter the hypothalamic–pituitary–adrenal (HPA)
axis, which is also involved in thyroid hormone production (223). Noradrenaline is believed to have a stimulatory influence on TSH secretion
(224). The level of cord blood thyroid stimulating hormone has been found
to be higher among newborns believed to have undergone greater perinatal
stress, including the onset of labour (216), longer duration of second stage
(225-226), nuchal encirclement of the cord (226), meconium stained amniotic fluid (225-226), caesarian section (200, 227), vacuum extraction (225),
forceps extraction (228), hypoxaemia (228-229), low Apgar score (230232), small for gestational age (229). Although, other researchers state that
elevated TSH values observed in newborns delivered vaginally (216, 225226). Vaginal deliveries requiring augmentation and cesarean sections after
attempted labor are stressful for the infant, this may initiate a cascade of thyroid axis hormonal responses (216). Infants born by vaginal breech delivery
also had a higher incidence of elevated levels of cord blood thyroid stimulating hormone compared with cephalic-presenting infants (233). Interestingly,
the fetal presentation has been reported to have no effect on levels of newborn cord blood thyroid stimulating hormone in those born by elective caesarean section (i.e. without labour). For newborns born by emergency caesarean section after onset of labour, the median level of thyroid stimulating
hormone is higher among newborns with breech presentation, compared
with those with cephalic presentation (219). The median level of cord blood
thyroid stimulating hormone is also higher if the cephalic presentation is a
result of a prior successful external cephalic version, compared with spontaneous cephalic presentation (219). Mean TSH values were observed to be
significantly lower in preterm than in full-term infants (234). The postulated
mechanisms of stress-induced elevation of cord blood thyroid stimulating
32
hormone include catecholamine release and pituitary hyperactivity in response to intrauterine asphyxia (224). Increased differential brain perfusion
and decreased thyroid perfusion during hypoxia also have been proposed
(229). The mode of delivery is associated with maternal and fetal endocrine
stress responses (222). Therefore, we investigated the impact of delivery
mode factors on newborn the blood spot TSH results in singleton pregnancies.
1.3. Maternal psychological factors and thyroid function tests during
pregnancy interference with newborn TSH and anthropometric
parameters
1.3.1. Maternal thyroid axis parameters repercussions with newborn
TSH
Transplacental passage of TSH from mother to fetus is negligible, but
maternal T4 could be found in fetal compartment (235). Throughout gestation, the serum TSH values are grater in fetus than are present in maternal
circulation and higher than would be expected in adults with normal thyroid
function (45). This indicates that there is an increasing hypothalamicpituitary resistence to T4 during fetal development which is speculated to be
a consequence of increased TRH secretion (235-236). From these results it
was concluded that maternal TSH does not pass through the placental barrier. In this respect, the fetal pituitary-thyroid axis functions as a unit that is
essentially independant of the mother (235, 237-238).
Nevertheless, maternal thyroid dysfunction, especially in early
pregnancy, may place the mother and fetus at an increased risk of adverse
obstetrical outcomes (239). Untreated hypothyroidism is associated with
increased risk for preeclampsia, low birth weight, placental abruption,
miscarriage, and perinatal mortality (1, 12, 15, 240-242). Recently, Idris et
al. found that in addition to an increased risk of low birth weight,
hypothyroidism early and late in pregnancy may increase the rate of
caesarean section (242). Elevated maternal serum TSH in the second
trimester is also associated with an increased rate of fetal death after 16
weeks’ gestation (12). Studies have found that although women treated for
hypothyroidism may have higher rates of preeclampsia (243) and cesarean
section (19) than euthyroid women. Tan et al. observed that women who are
treated with levothyroxine (L-T4) in pregnancy were not at increased risk of
maternal or neonatal morbidity (244).
In addition to adverse obstetrical outcomes, maternal thyroid dysfunction
is associated with impaired mental development of the infant (29, 239, 245).
33
Neuropsychological deficits in the child from as early as 3 weeks to 9 years
of age have been observed. Kooistra et al. studied newborns born to mothers
with serum free thyroxine (FT4) levels below the 10th percentile at 12
weeks’ gestation, and observed decreased neonatal behavioural assessment
scores at three weeks of age, compared with control subjects (28). Pop et al.
studied healthy infants and found that having maternal serum FT4 levels
below the 10th percentile at 12 weeks’ gestation was a significant risk for
impaired psychomotor development at 10 months of age (245). A similar
result was observed by Kasatkina et al. (246). The finding of a low maternal
serum FT4 level at five to nine weeks’ gestation correlated significantly
with a lower coefficient of mental development at 6, 9, and 12 months of
age (246). Mothers with low serum FT4 at 12 weeks’ gestation who
continued to have low levels at weeks 24 and 32 were at risk of having a
child with delays in mental and motor development at one and two years of
age. This neurodevelopmental delay was even more profound when the
mothers had a continuing decrease in serum FT4 as pregnancy progressed
(29). Children born to women who were not treated for thyroid deficiency
during pregnancy had average IQ scores at seven to nine years of age that
were 7 points lower than those of controls (15).
It is clear that maternal thyroid plays an essential role in the course of
pregnancy, therefore we decided to analize newborn TSH levels at three
days of age in relation to maternal thyroid hormone axis.
1.3.2. Antenatal maternal mental state and thyroid axis function
interference with anthropometric characteristics of the newborn
Thyroid hormones profile changes during pregnancy (247) and may
affect maternal (185, 248) as well as fetal well-being. Our understanding
that thyroid disease has negative impact on pregnancy course and outcomes
is increasing. Presence of thyroid antibodies in euthyroid women is
associated with misscariage (157) and during early pregnancy with maternal
depression (60). It has been shown that hypothyroidism during pregancy is
associated with higher rates of gestational hypertension, fetal death,
miscarriage, lower birthweight of newborns and disturbed mental
development of the child (1, 12, 15, 240). It was also demonstrated that
maternal hypothyroxinemia (29, 245) during pregnancy is associated with
impaired mental development of the infant. However, there are scanty data
on effects of changes in thyroid hormone profile during pregnancy on
anthropometrics of the newborns.
The neonatal anthropometric characteristics such as birthweight are
considered to be directly related to health and nutrition of mother during
34
pregnancy and represent development of fetus. Birthweight is an important
factor that determines infant and childhood morbidity and mortality (249).
Moreover, alterations in birth weight has been shown to be associated with a
number of adverse medical outcomes later in life, such as diabetes,
hypertension, metabolic and cardiovascular disorders (250-252).
Birthweight is affected to a great extent by mother’s own foetal growth
and her diet from birth to pregnancy, and thus, her body composition at
conception (68). Maternal anthropometric parameters, such as pregestational
body size indices and gestational weight gain have repeatedly been shown to
be independent determinants of the size of the child (253-254). Therefore,
maternal metabolic and endocrine factors may well be independent
determinants of fetal growth (255). Apart from maternal plasma glucose,
studies on the role of maternal metabolic parameters as independent
determinants of fetal growth are limited (255-256). Recently, in the animal
models it was investigated that a low protein diet, even in the preimplantation phase, causes vascular dysfunction in offspring resulting in
high blood pressure and anxiety related behavior (257-258). Similarly, in
women a high carbohydrate diet, especially when combined with low
protein, suppresses placental growth which impacts on offspring birth
weight (259). Furthermore, the long term diet of a woman, even from her
own developing years, also has effects on her pregnancy and placental
ability to support an embryo (260). It is possible that the effects of maternal
anxiety, depression and stress on the developing fetus and newborn are
moderated by these factors together with maternal diet (261). Studies
showed that inappropriate eating behaviors are commonly followed by other
psychiatric symptoms, such as anxiety and depression (262-263).
Psychiatric disorders, particularly mood and anxiety disorders, have the
highest prevalence in women during childbearing years (264).
Apart from well-known biomedical risk factors for fetal development,
including history of adverse pregnancy events, exposure to teratogenic
substances, multiple-gestations and others, various maternal psychological
problems widely prevalent during pregnancy including stress, anxiety and
depression were shown to have significant negative effect on fetal and
neonatal outcomes (265-266) including preterm birth, obstetric
complications, lower 5-minute Apgar scores, lower birthweight, congenital
anomalies and postpartum depression (266-270).
The results from recent population based study showed that the
prevalence of depression and/or anxiety disorders among pregnant woman is
up to 30% and it seems to be higher during pregnancy than postpartum
(271). In Lithuanian pregnant woman the prevalence of depressive disorders
was found to be about 7% and the prevalence of symptoms of depression
35
was reported to be about 17% (272). Depression and anxiety disorders
might have a negative impact on well-being of pregnant woman, on their
relationship with family members and might interfere with fetus growth and
development. If untreated, these antenatal mood disorders together with
socio-economic deprivation and with other adverse factors may increase the
likelihood of postnatal depression (263, 273). Furthermore, antenatal
maternal depression as well as antenatal anxiety disorder is a risk factors for
behavioral and emotional problems (274) and psychotic illness (275-276) in
later life of children (277).
A recent study in a large sample of newborns showed that trait anxiety in
the first two trimesters of pregnancy is associated with lower bithweight and
shorter birth length after controlling for confounders (278). Although an
association between pathophysiology of these psychiatric disorders and
pregnancy outcomes remains unclear, it is thought that depression, anxiety
and stress during pregnancy might have negative effect on mother’s health
related behaviors, such as increased alcohol and tobacco consumption or
poor nutrition that are associated with decreased birthweight (279).
Moreover, depression, anxiety and stress were showed to cause a
dysregulation of HPA axis (261, 280), decreased fetal growth hormones
(265) and increased uterine artery resistance (281-282). Both maternal trait
anxiety and maternal experience of anxiety during pregnancy determine
offspring development (283) so, importantly, the study shows that maternal
anxiety impacts on offspring in an adverse way. Additionally, stress in
pregnancy programs high anxiety in offspring (284). If stress is sustained
(chronic), the typical response is elevated basal glucocorticoid
concentrations, altered negative feedback to the HPA axis (285-286). Lately
it is discussed, that in control of maternal anxiety there is an emerging role
for progesterone secretion in the brain (287-288). Increasing anxiety can
lead to depression, which can be very severe perinatally. Interestingly,
anxiety decreases in early gestation and remains subdued until birth (289).
Pregnancy anxiety has been recognized as emerging in women that
generally lack social support (290) and may be living under environmentrelated stressful conditions, while lack of physical activity leads to higher
anxiety and mood disturbances (291). It seems that chronic stress can induce
maternal anxiety in rodents (292) and even predispose to postnatal
depression.
The interaction between maternal personality traits during pregnancy and
neonatal outcomes is not widely studied, but it is possible that some
personality traits might predispose maternal behavior that interferes with
well-being of fetus and that others may have protective effect. It is known
that adults with high conscientiousness have better health outcomes and
36
longevity whereas adults with high neuroticism have poorer health outcomes and more likely to engage in lifestyle risk activities, such as smoking
and alcohol intake (293). High level of neuroticism is associated with higher
levels of anxiety and stressfulness (294). In pregnant women such personality traits might influence neonatal outcomes, including anthropometric characteristics (261). Personality traits may modulate emotional and endocrine
responses to stress causing changes in hormonal profile that may lead to an
unfavorable environment to the development of fetus (268, 295-296).
Therefore, the aim of the present study was to assess whether psychological factors and thyroid axis hormone concentrations during pregnancy predict neonatal anthropometric characteristics.
37
2. MATERIAL AND METHODS
2.1. Study population
Pregnant women were eligible for enrolment into the study if they presented for the antenatal care in Kaunas, Lithuania, at the Department of Obstetrics and Gynecology at Kaunas University of Medicine as well as at
Šilainiai Primary Health Care Center between 2003 and 2005 years and
agreed to participate giving written informed consents these women were
continuously inrolled in the study:”Effect of psychoendocrine challenge
during gestation and delivery to well–being of mother and child: multi–
central study”. The study and its consent procedures were approved by the
Regional Committee of Ethics in Biomedical Research at the Kaunas University of Medicine, Kaunas, Lithuania (No. 84/2002 and P1-84/2002).
A total of 322 pregnant women were assigned for participation. Subjects
in the different studies are shown in Figure 2.1.1. Exclusion criteria were
known extragenital disease, including current or past thyroid disease, thyroid function modifying medication, family history of thyroid disease, multiple pregnancy, hyperemesis gravidarum, fetal congenital abnormalities.
Attendance to all assigned serum thyroid hormone samplings and emotional
state evaluation was required. Of these 322 women, 15 did not attend any
serum sampling and 18 women were excluded because of type I diabetes
(n=3), multiple sclerosis (n=1), pre-existing goiter (n=6), thyroid hormone
therapy (n=1), toxoplasmosis during pregnancy (n=1), twin pregnancy (n=4)
and fetal cerebral malformations diagnosed at ultrasound screening (n=2).
An initial sample group consisted of 289 apparently healthy pregnant women (mean age 28.3 ± 4.9 years; range 18–41 years), and they were evaluated
for thyroid function during the first (12th–16th week), the second (22nd–
26th week) and the third trimester (32nd–36th week) of pregnancy. Of them,
105 missed at least 1 meeting of hormonal measurement, therefore excluded
from the study data analysis (Figure 2.1.1). The final analysis of maternal
thyroid function and thyroid immune status was performed using data from
184 pregnant women. Our research was constructed by iniciation of five
study designs. Main characteristics of the cohort are provided in Table 2.1.1.
The study I assessed maternal thyroid function tests during pregnancy. Of
184 pregnant women, 23 (12.5%) women were found to have elevated TPOAb concentrations (mean age 27 ± 5 years, range 20–40). After excluding
TPO-Ab positive women, the remaining 161 (87.5%) data sets were used as
reference population establishing reference intervals for the thyroid hor-
38
mones concentrations in three trimesters of pregnancy. In this group, one
woman (0.6%) had a TSH>4.5 mIU/L, and 40 (24.8%) had TSH<0.4 mIU/L
in the 1st trimester.
Assigned for
participation
N=322
15 not
attended
18 excluded
Follow up
N=289
12th–16th week
22nd–26th week
32nd–36th week
Lost to followup women
N=105
Lost to followup newborn
N=74
Women
N=184
12th–16th week
22nd–26th week
32nd–36th week
Study I
Newborn
N=215
Study II
Lost to follow –up
6 newborn
5 women
Pair mother–newborn
N=173
Study III, IV, V
Figure 2.1.1. General design of the study
Study II evaluated iodine insufficiency by using newborn heel blood spot
TSH measurements taken on the third day after birth. There were 74 newborns excluded, due to early TSH measure. The third day dry blood spot
TSH was obtained from 215 newborns. Two newborns were exluded on the
basis of incorrect typing of laboratory results. In iodine study, 213 newborns
were used as target group for analysis.
39
Table 2.1.1. Characteristics of the study women and their children
Variables
Study I
Study III, IV, V
Maternal variables
N=184
N=173
28.2 ± 4.8 (19–41)
28.3 ± 4.8 (19–41)
Prepregnancy weight* (kg)
76.6 ± 10.6
76.6 ± 10.6
Height* (cm)
167.8 ± 5.6
167.8 ± 5.6
0.40 ± 0.1
0.39 ± 0.2
27.2 ± 3.5 (20.7–41.7)
27.2 ± 3.5 (20.7–41.7)
BMI>30 kg/m , n (%)
36 (19.6)
34 (19.7)
Nullipara, n (%)
114 (62.9)
105 (60.7)
Average parity*
1.9 ± 1.1
Study II
N=213
120 (56.3)
1.9 ± 1.1
96 (55.4)
39.6 ± 1.2 (35–41)
39.6 ± 1.0 (35–41)
7 (3.2)
1 (1.1)
3.558 ±448 (2176–4700)
3.550 ±448 (2176–4650)
Age* (years)
Mean (SD), range
Weight gain*, kg/week
Prepregnancy BMI*, kg/m
2
Mean (range)
2
Newborn variables
Gender (% males)
N=173
a
Gestational age (weeks)
Mean (range)
Premature, n (%) <37 weeks
Birthweight* (g)
Mean (range)
Birth height* (cm), (range)
51.8 ± 2.1 (46–63)
51.8 ± 2 (46–63)
* Characteristic described as mean±S.D.or n (%) were appropriate; BMI, body mass index
Studies III, IV, V required mother-newborn pairs data. Further data was
used to examine the relation between newborn thyroid stimulating hormone
concentration and delivery outcomes and maternal thyroid function during
pregnancy (study III). Additionally, data was used to evaluate the relation of
maternal thyroid function, emotional state and anthropometric characteristics of the newborns (study IV, V). For those studies, mother’s birth delivery
medical records were reviewed for maternal and newborn delivery data, anthropometric characteristics. Delivery case data of 6 newborns was not
available. Three women were excluded from the study because they had diagnosis of gestational diabetes, 2 women were excluded from the study because they delivered very low birthweight newborns (<1500 g). A total
sample of 173 mother–newborn pairs was finally included in the analysis.
The main characteristics of the cohort are provided in Table 2.1.1.
40
2.2. Methods
Assays. Blood sample analysis for thyroid function during pregnancy was
carried out and serum TSH and FT4 were measured in all trimesters of gestation. Venous blood samples for TSH and FT4 were drawn from 9 am to 14
pm in the first trimester at 12-16, second trimester at 22-26 and third trimester at 32-36 weeks of gestation. In the first trimester we also assessed
TPO-Ab concentrations. All samples were centrifuged from 14 till 16.30 pm
daily. Serum was collected in tubes without gel berriers or clot-promoting
additives and frozen at -70°C. Once thawed before analyses, each assay was
performed on all samples using the same kits to minimize inter–assay variation at the Labarotory in Tilburg University, The Netherlends.
TSH was measured using a solid–phase, two site chemiluminescent enzyme immunometric assay (IMMULITE Third generation TSH, Diagnostic
Products Corporation, Los Angeles, USA). The inter–assay coefficients of
variation were 5.0 % and 4.4 % at concentrations 0.22 and 2.9 mIU/L, respectively. FT4 concentration was measured with a solid–phase immunometric assay (IMMULITE Free T4). The interassay coefficients of variation
for this technique were 6.7 % and 4.4 % at concentrations 11.6 and 31.5
pmol/L, respectively.
The Immulite assay provided a TSH reference interval of 0.4–4.5 mIU/L
and a FT4 reference interval 10.3–25.7 pmol/L for nonpregnant adults. The
assay manufacturer’s population reference intervals calculated from serum
specimens from individuals with normal thyroid function (iodine status
wasn’t defined in the manufacturers specifications). The reference intervals
for nonpregnant adults provided by the manufacturer are also included for
comparison with gestational age–specific reference interval.
Finally, the IMMULITE TPO-Ab kit was used for the determination of
TPO-Ab. The inter–assay coefficients of variation for this analysis were 9.0
% and 9.5 % for concentrations 40 and 526 IU/mL, respectively. The TPOAb assay was standardized in terms of the International Reference
Preparation for TPO-Ab MRC 66/387. Reference intervals for TPO-Ab (<
35 IU/ml) were taken from the manufacturer’s kit insert. TPO-Ab titers
above 35 IU/ml were defined as elevated; TPO-Ab titers below 35 IU/ml
were defined as normal concentrations.
In study II, newborns were used as target groups for iodine monitoring.
Blood spot TSH measures were used from the National Neonatal Screening
Program for congenital hypothyroidism. Recommended timing of taking
blood from a heel prick is better after 48 hours, of age to minimize the false
positive high TSH due to the physiological neonatal TSH surge that elevates
TSH levels and causes dynamic T4 and T3 changes in the first 1 or 2 days
41
after birth (297). Therefore our blood spot TSH data was obtained on the
third day after birth, according to the institutional regulations by the nurse–
neonatologist. The neonatal enzyme immunoassay with fluorometric detection (Neonatal hTSH FEIA Plus, product No. 6199880) was used for determination of TSH from blood specimens dried on filter paper. The newborn
Screening Programme Centre recommends that cut–off for a blood spot
TSH 10 mIU/L is used to detect congenital hypothyroidismn (217). All
measures of TSH in blood specimens dried on filter paper were analyzed at
the Centre for Medical Genetics, Vilnius University Hospital.
Neonatal and maternal parameters (study II–V). Detailed information on
maternal and neonatal factors was obtained from medical records from three
delivery centers: Kaunas Medical University Clinics, P. Mažylis Maternity
Hospital, Kaunas Christian Maternity Hospital and Kaunas 2nd Clinical
Hospital. Gestational age was defined by the known date of last menstrual
period and/or ascertained by early ultrasound assessment. Infants delivered
before 37 weeks of gestation are considered premature. Length of gestation
at delivery was treated as a continuous variable measured as the number of
weeks of gestation at delivery. Infant birth weight in grams was examined as
a continuous variable. From birth delivery medical case histories we analyzed gender of the newborns, birth weight (in grams), height (in centimeters) and gestational age. Weight and height of the newborns were substantiated by neonatologist who supervised childbirth in the first 24 postnatal
hours. Maternal prepregnancy weight (in kilograms), height (in centimeters)
were measured at the first antenatal visit by observing nurse. Weightgain (in
kilograms per week) was calculated out of the measured weight at delivery.
We also calculated Body Mass Index (BMI) of the mother and the newborn,
using formula: BMI = weight (kilograms) / height2 (meters). Maternal age at
delivery, delivery mode was registered.
Apgar scores on the 1st and 5th minutes of extrauterine life of the newborns were evaluated by neonatologist who supervised childbirth in the 1st
and 5th postpartum minutes. Apgar score is used in clinical practice to assess a newborn’s respiratory effort, heart rate, color, tone and reflex irritability (Table 2.2.1). Scoring range is from 0 to 10. Apgar scores between 8 and
10 indicate that the newborn is making smooth transition to extrauterine life;
scores ≤7 are associated with increased morbidity and mortality of newborns.
Study IV, V. Pregnant women were evaluated three times by psychiatrist
(L.K.) for stress, depression symptoms and anxiety in the first trimester
(12th–16th weeks), in the second trimester (22nd–26th weeks) and in the
third trimester (32nd–36th weeks) of pregnancy and were evaluated for personality traits in the second trimester of pregnancy. Thesis “Depression and
42
its relationship to thyroid function during pregnancy” has been defended by
psychiatrist (L.K.).
Table2.2.1. Apgar scores
Score
Criteria
Color
Heart rate
Reflex response to nasal
catheter/tactile stimulation
0
Absent
1
Pink body, blue
extremities
<100 beats/min
>100 beats/min
None
Grimace
Sneeze, cough
All blue, pale
Muscle ton
Limp
Respiration
Absent
Some flexion of
extremities
Irregular, slow
2
All pink
Active
Good, crying
Psychosocial stressors were classified according to the life events using
the Diagnostic and Statistical Manual of Mental Disorders, third edition, revised (DSM–III–R) (298), Axis IV criteria of the Perceived Psychosocial
Stress Scale (PPSS). This instrument evaluates acute and chronic perceived
psychosocial stressors. Women were interviewed about negative life events
that are considered to cause psychosocial stress. Each negative life event is
rated according to how severe it would be to an average individual. The
score for chronic stress and the score for acute stress are set and the higher
score indicates the higher perceived chronic stress or the higher perceived
acute stress. Score of 1 indicates no psychosocial stress, 2 – mild psychosocial stress, 3 – medium psychosocial stress, 4 – severe psychosocial stress, 5
– very severe psychosocial stress and 6 – catastrophic psychosocial stress.
In this study we categorized women in two groups, those who did experience acute/chronic stress with PPSS score of two or more; and those who
did not experience PPSS.
Antenatal maternal personality traits were evaluated using Lithuanian
version of the Big Five Personality Inventory (BFPI) (294). An instrument
of 44 questions designed to assess the Big Five personality dimensions of
Extroversion, Agreeableness, Conscientiuosness, Neuroticism and Openness. BFPI consists of 5 subscales. Extroversion and neuroticism subscale
consist of 8 items, agreeableness and conscientiuosness of 9, openness of
10, respectively. Each item is a descriptor and is rated in a 5–point scale
from 1 (agree strongly) to 5 (disagree strongly). The BFPI showed good
psychometric properties (294).
The validated Lithuanian version (299) of the Edinburgh Depression
Scale (EDS) was used to measure severity of depressive symptoms (300).
43
Though originally, this instrument was designed for screening of postnatal
depression, today it is widely used for evaluation of depressive symptoms
throughout all periods of women’s life in clinical practice as well as in epidemiological studies (301). The EDS is beneficial against other instruments
used for screening of depressive symptoms during pregnancy because it
evaluates psychological, cognitive, but not physical symptoms of depression
that are prevalent during pregnancy. The EDS is easy to administer and
most important, it is an effective screening tool for identifying woman with
depressive symptoms during pregnancy. The EDS is a ten item selfrating
instrument and takes 2 to 5 minutes to complete. Each item is scored from 0
to 3, to which subject responds and is based on her experience over the past
seven days. Possible scoring range is from 0 to 30. Higher score on the EDS
indicates higher severity of depressive symptoms. Depression is clinically
significant, when EDS score is ≥12.
Symptoms of anxiety were evaluated using the Spielberger State-Trait
Anxiety Inventory (STAI) (302). The STAI – Trait scale is widely used for
clinical and research purposes in psychiatric population as well as in mentally healthy subjects, including pregnant women, to assess severity of anxiety
symptoms (303). The Trait-Anxiety scale of STAI consists of twenty statements that assess how respondents feel "generally”. We considered that
women are positive for symptoms of anxiety if they scored 45 or more on
the STAI-T.
Women were also interviewed about smoking and use of alcohol during
pregnancy. Because only 1.2% (2 women) of the sample were non–daily
(occasional) smokers, and 100% reported never drinking during pregnancy,
these variables were not examined in the analyses.
2.3. Statistical analyses
Results are expressed as mean and median values; variability is indicated
by SD and/or value range. All continuous data are represented as means
(SD, standard deviation), all categorical data as numbers and percent. Frequency rates were compared by 2 test. The correlation among variables was
performing by using the Pearson correlation coefficient or ordinal regression, when normality assumption was satisfied, and for non-normal variables the Spearman correlation coefficient was used. The hypothesis of the
dispersion equality was verified using Levene’s test.
Study I. Following descriptive variables, skewness was estimated by the
Kolmogorov-Smirnov test: p<0.05 was considered to indicate a nonGaussian distribution. TSH showed a left skewed non-Gaussian and values
44
of FT4 concentrations a near normal distribution. The most powerful transformation to reduce the positive skew was square root transformation. TSH
was normalized using square root transformation in order to use parametric
tests and summarized as means with 95% confidence intervals (CI). Transformed mean values were untransformed for presentation. Means were
compared with t-tests and analysis of variance.
General linear models (GLM) using both the repeated measures ANOVA
(three time points) and the mixed model for the repeated measures ANOVA
(three time points, two groups - TPO-Ab negative and positive), were used
to explore the longitudinal effect of pregnancy (followed by Bonferroni post
hoc pair-wise comparisons) and the effect of elevated TPO-Ab on the thyroid axis hormone concentrations (F test was reported). The comparisons in
TPO-Ab positive and negative mothers among trimesters were made by
GLM univariate ANOVA followed by pair-wise comparisons. For two
group comparisons, ANOVA will give results identical to a t-test. The F
tests the effect of TPO-Ab. Effect size for the repeated measures ANOVA
was measured by eta squared η2. A p-value of <0.05 was considered significant.
The reference intervals of the hormone concentrations are reported as
median and empirical (based on the order statistics) 2.5th–97.5th percentiles
by trimester. The International Federation of Clinical Chemistry (IFCC)
recommends at least 120 reference values to use for the calculation of a reference interval (denoted the 0.95 central inter-fractile interval and defined as
the interval between the 0.025 and the 0.975 fractiles of the distribution).
For most purposes, non-parametric intervals are recommended (304). The
trimester-specific TSH reference intervals were calculated with TPO-Ab
positive women excluded and included.
Study II. Mean, median and standard deviation (SD) of TSH values of the
newborns were considered to report the result of the screening. The Mann–
Whitney test was used to detect difference in median by groups defined by
newborn gender. Newborns TSH complied with assumptions of normality
of the dependent variable. The effects of maternal age, gestational age, gender and birth weight on newborn TSH levels were assessed by analysis of
variance (ANOVA), multiple correlation coefficient, the Spearman‘s correlation coefficients. Since birth weight is dependent on gestational age, we
conducted a multivariate analysis simultaneously to examine the relationship between neonatal TSH levels and maternal age (modeled continuously), newborn gender, gestational age and birth weight. Multiple linear regressions were performed to quantify the associations between the above
parameters and change in TSH.
45
Study III. The linear regression analysis was used to examine whether
maternal age and pre–pregnancy weight, gestational age, thyroid function in
all three trimesters of pregnancy predicted anthropometric characteristics
and Apgar scores of newborns. Five separate regression models were created for neonatal weight, height, BMI and Apgar scores in the 1st and 5th
minutes of extrauterine life. Linear and quadratic terms (a quadratic term for
maternal age was included in the final analysis to improve model fit) of maternal
age at the time of delivering the birth, gestational age, pre–pregnancy
weight, number of gestations, duration of pregnancy, gender of the newborn, TSH and FT4 values in all three trimesters of pregnancy were used as
independent variables. Parity, the number of times a woman had previously
given birth, was dichotomized into 0 – nulliparous or 1 – multiparous. This
set of variables was reduced by backward elimination until only those significant at p < 0.05 remained in the model. Using the determination coefficient R2 value and the model correspondence criterion, we created the optimal regression model allowing for prognosis of anthropometrics of newborns. Factors that were not statistically significant and worsened the R²
value were excluded from the final regression model.
Study IV, V. For comparison of score on the EDS, STAI, acute and
chronic stress among three trimesters, the non parametric tests (Friedman
test) were applied.
The linear regression analyses were used to examine whether maternal
age and pre-pregnancy weight, gestational age, thyroid function, symptoms
of depression, symptoms of anxiety, perceived acute and chronic psychosocial stress in all three trimesters of pregnancy and personality traits in the
second trimester of pregnancy predicted anthropometric characteristics and
Apgar scores of newborn. Five separate regression models were created for
neonatal weight, height, BMI and Apgar scores in the 1st and 5th minutes of
extra-uterine life. Linear and quadratic terms (a quadratic term for maternal
age was included in the final analysis to improve model fit) of maternal age
at the time of delivering the birth, gestational age, pre-pregnancy weight,
number of gestations, duration of pregnancy, gender of the newborns, TSH
and FT4 values, score on the EDS, scores on the STAI, perceived acute and
chronic psychosocial stress in all three trimesters of pregnancy and score on
the BFPI in the second trimester of pregnancy were used as independent
variables. The dichotomonuous variables were created with values of acute
and chronic stress; non-stress category included all participants who not
identified themselves as stressed.
This set of variables was reduced by backward elimination until only
those significant at p < 0.05 remained in the model. Using the determination
coefficient R2 value and the model correspondence criterion, we created the
46
optimal regression model allowing for prognosis of anthropometrics of
newborns. Factors that were not statistically significant and worsened the R²
value were excluded from the final regression model. A probability level of
p<0.05 was considered as statistically significant. All statistical analyses
were performed using software from Statistical Package for Social Sciences
15.0 for Windows (SPSS, Inc., Chicago, Ill., USA).
47
3. RESULTS
3.1. Maternal thyroid function tests during pregnancy (Study I)
3.1.1. Reference intervals for thyroid testing at each trimester of
pregnancy
The descriptive statistical measures of serum TSH and FT4 concentrations in terms of mean, median and standard deviation, 2.5th and 97.5th percentiles in healthy pregnant women negative for TPO–Ab in three trimesters
of pregnancy are presented in Table 3.1.1.1. The reference intervals for
nonpregnant adults provided by the manufacturer are also included for comparison.
The reference intervals for TSH concentrations were found to be 0.02–
2.72 mIU/L for the first trimester, 0.22–2.51 mIU/L for the second trimester
and 0.28–2.36 mIU/L for the third trimester of pregnancy.
The reference intervals for FT4 concentrations were determined to be
13.2–23.1 pmol/L for the first trimester, 11.8–18.5 pmol/L for the second
trimester and 10.5–18.3 pmol/L for the third trimester of pregnancy.
Table 3.1.1.1. Descriptive statistics of TSH and FT4 concentrations for each
trimester of pregnancy in healthy women negative for TPO-Ab (N=161)
TSH, mIU/L
Trimester of pregnancy
1st
2nd
3rd
Mean
0.83
1.04
1.00
Median
0.70
0.93
0.91
Standard deviation
0.67
0.57
0.51
Minimum
0.003
0.08
0.13
Maximum
4.82
3.78
3.03
Skewness
2.29
0.49
1.44
Kolmogorov–Smirnov test
Kolmogorov–Smirnov test after square
root transformation
Trimester specific reference intervals,
calculated as 2.5 – 97.5 percentiles
Manufacturer’s nonpregnant adult reference interval a
0.014
0.002
0.056
0.823
0.079
0.412
0.02–2.72
0.22–2.51
0.28–2.36
0.4–4.5
48
Table 3.1.1.1 (continued)
FT4, pmol/L
Trimester of pregnancy
1st
2nd
3rd
Mean
17.15
14.57
13.97
Median
17.00
14.50
13.90
Standard deviation
2.36
1.75
1.80
Minimum
12.20
11.20
8.64
Maximum
23.70
22.20
21.20
Skewness
0.80
1.13
0.37
Kolmogorov–Smirnov test
Trimester specific reference intervals,
calculated as 2.5 – 97.5 percentiles
Manufacturer’s nonpregnant adult reference interval a
0.565
0.432
0.831
13.2–23.1
11.8–18.5
10.5–18.3
10.3–25.7
a
The IMMULITE Third generation (Diagnostic Products Corporation, Los Angeles, USA)
analyzer was used for testing. TSH, thyrotrophin; FT4, free thyroxine.
3.1.2. Trimester changes in concentration of TSH and FT4 during
pregnancy
Serum TSH (based on square root–transformed value) and serum FT4
(arithmetic means) concentrations in 161 women without elevated TPO-Ab
concentrations and in 23 pregnant women with elevated TPO-Ab concentration are presented in Figures 3.1.2.1 and 3.1.2.2.
A 3 (trimester) x 2 (TPO-Ab) mixed-model for the repeated measures
ANOVA showed that there was a significant main effect on TSH for TPOAb, F(1,182)=15.19, p<0.001 (Figure 3.1.2.1). The interaction effect (trimester x TPO-Ab) is important and it is significant at p=0.002. Clearly, the
TPO-Ab is having a differential effect on the two groups. Two analyses
were run, one on each group. A repeated measures ANOVA determined that
mean TSH concentration in the TPO-Ab negative women differed statistically between trimesters F(2,160)=25.34, p<0.001, though this was a relatively small effect size (η2=0.14). Post hoc tests revealed that was a significant difference in TSH levels between trimesters 1 and 2, and 1 and 3
(p<0.001), but no significant difference between trimesters 2 and 3. The
changes in TSH by trimester in TPO-Ab positive women were not significant (F(2,22)=1.35, p<0.27).
49
**
2
TSH, mIU/L
**
*
1.5
TPOAbpositive
TPOAbnegative
1
0.5
0
I
II
III
Trimester of gestation
Figure 3.1.2.1. Thyroid stimulating hormone (TSH) concentrations by trimester of gestation in pregnant women with normal (n=161) and elevated
(>35 IU/ml, n=23) TPO-Ab concentrations
Dots represent the normalized average of TSH in each trimester. A square root transformation was used (mean, 95% CI).
** p<0.01; * p<0.05 age adjusted differences between subjects positive and negative for
TPO–Ab;
Comparison among trimesters:
TPO-Ab ≤ 35 IU/ ml: I vs. II and III p<0.001; II vs. III p>0.05
TPO-Ab >35 IU/ml: I vs. II and III; II vs. III p>0.05
The results of comparisons among trimesters in TPO-Ab positive and
negative mothers by GLM univariate ANOVA showed significant effect on
TSH for TPO-Ab in the first and second trimesters, but not in the third trimester (p=0.071). After controlling for age (with age as covariate) the TPOAb positive women had significantly higher TSH concentrations compared
to TPO-Ab negative in the first (F(1,183)=11.59, p=0.001); in the second
(F(1,183)=12.45, p=0.001) and third trimester (F(1,183)=4.58, p=0.035).
The means (95% CI) of the square root transformed TSH concentrations
for each trimester were 0.71 (0.62–0.81), 0.97 (0.88–1.06), and 0.94 (0.86–
1.02) mIU/L, respectively (Figure 3.1.2.1).
Mixed-model for repeated data revealed that the main effect of TPO-Ab
on FT4 was not significant F(1,182)=0.56, p=0.45 (Figure 3.1.2.2). Thus,
there was no overall difference in the FT4 of TPO-Ab positive compared to
TPO-Ab negative. The fact that the linear trend was not significant for the
interaction (trimester x TPO-Ab) means that both groups are showing about
the same linear trend. A significant main effect for trimester was obtained,
F(1,182)=89.8, p<0.001, η2=0.33. Bonferroni comparisons revealed a significant difference in FT4 levels between trimesters 1 and 2, and 1 and 3, and 2
and 3 (p<0.001) in TPO-Ab negative women. In TPO-Ab positive there was
50
a significant difference in FT4 levels between trimesters 1 and 2, and 1 and
3 (p<0.05), but no significant difference between trimesters 2 and 3.
The means (95% CI) of FT4 concentrations for each trimester were 17.15
(16.78–17.52), 14.57 (14.30–14.84), and 13.97 (13.69–14.25) pmol/L, respectively. The physiologic decrement in the mean concentrations of FT4
reaching 19% was observed during the second and the third trimester of
pregnancy compared to the first trimester of pregnancy in both groups of
women (Figure 3.1.2.2).
FT4, pmol/L
20
18
TPOAbnegative
TPOAbpositive
16
14
12
10
I
II
III
Trimester of gestation
Figure 3.1.2.2. Free T4 concentrations by trimesters of gestation in
pregnant women with normal (n=161) and elevated (>35 IU/ml, n=23)
TPO-Ab concentrations (mean, 95% CI)
The physiologic decrement of mean FT4 concentrations during pregnancy, 19%.
Comparison among trimesters:
TPO-Ab ≤ 35 IU/ ml: I trimester vs. II and III; II vs. III p<0.001;
TPO-Ab >35 IU/ml: I trimester vs. II and III p<0.05; II vs. III p>0.05.
Gestational age-specific reference intervals in antibody negative women
for each assay are shown in Table 3.1.1.1. These reference intervals were
used to classify TFT results (e.g. ‘high’=above 97.5th confidence limit,
‘normal’=within central 95% confidence interval, and ‘low’=below 2.5th
confidence limit), and then were compared with classifications determined
using the non-pregnant assay-specific reference intervals provided by the
assay manufacturer (Table 3.1.2.1).
51
Table 3.1.2.1. Serum TSH and FT4 concentrations in pregnancy outside the
reference intervals (RI)
TSH
Trimester of gestation
1st
2nd
1st
<Lower limit, n (%)
40 (24.8)
9(5.6)
13 (8.1)
>Upper limit, n (%)
1 (0.6)
0
0
<Lower limit, n (%)
3 (1.9)
5 (3.1)
3 (1.9)
>Upper limit, n (%)
4 (2.5)
3 (1.4)
3 (1.9)
Outside non-pregnant RI (0.4-4.5 mIU/L)
Outside of gestation-related RI
Misclassified
<Lower limit
37 (22.9)
4 (3.7|)
10 (6.2)
Not identified
>Upper limit
4 (2.5)
3 (1.4)
3 (1.4)
FT4
Trimester of gestation
2nd
1st
2nd
<Lower limit, n (%)
0
0
0
>Upper limit, n (%)
0
0
0
<Lower limit, n (%)
4 (2.5)
4 (2.5)
4 (2.5)
>Upper limit, n (%)
3 (1.4)
3 (1.4)
2 (1.4)
Outside non-pregnant RI (10.3-25.7 pmol/L)
Outside of gestation-related RI
Misclassified
<Lower limit
0
0
0
Not identified
>Upper limit
0
0
0
a
RI, non-pregnant reference interval: TSH, 0.4-4.5 mIU /L; FT4, 10.3-25.7 pmol/L
When the non–pregnant TSH reference interval (0.4–4.5 mIU/L) was applied to the study participants, 37 women (22.9%) whose serum TSH concentration was within the first–trimester–specific reference range would
have been misclassified as having subclinical hyperthyroidism, and four
women (2.5%) with a TSH concentration above the first–trimester–specific
upper reference limit would not have been identified. In the second trimester
four women (3.7%) would have been misclassified and three (1.4%) had
gone unidentified while during the third trimester 10 (6.2%) would have
been misclassified and three (1.4%) not been identified. One woman in the
first trimester had a concentration of TSH over 4.5 mIU/L suggesting subclinical hypothyroidism; however, her FT4 concentrations were high nor-
52
mal. Moreover, her TSH and FT4 concentrations in the second and in the
third trimesters were also in the normal range confirming euthyroidism.
Figure 3.1.2.3, Figure 3.1.2.4 and Figure 3.1.2.5 show the plotted serum
TSH concentrations versus FT4 concentrations data against gestational age
in pregnant women with normal (n=161) and with elevated (n=23) TPO-Ab
antibody concentrations (>35 IU/mL) in three trimesters of pregnancy.
Figure 3.1.2.3. The spreadsheet showing distribution of FT4 versus TSH
serum concentrations in pregnant women with normal (n=161) and elevated
(>35 IU/ml, n=23) TPO-Ab concentrations in the 1st trimester of
pregnancy. The solid lines show manufacturers’s reference interval for
nonpregnant adults, the dotted lines show trimester specific distribution in
healthy pregnant women
53
Figure 3.1.2.4. The spreadsheet showing distribution of FT4 versus TSH
serum concentrations in pregnant women with normal (> 35 IU/ml, n=161)
and elevated (n=23) TPO-Ab concentrations in the 2nd trimester of
pregnancy. The solid lines show manufacturers’s reference interval for
nonpregnant adults, the dotted lines show trimester specific distribution in
healthy pregnant women
54
Figure 3.1.2.5. The spreadsheet showing distribution of FT4 versus TSH
serum concentrations in pregnant women with normal (n=161) and elevated
(>35 IU/ml, n=23) TPO-Ab concentrations in the 3rd trimester of
pregnancy. The solid lines show manufacturers’s reference interval for
nonpregnant adults, the dotted lines show trimester specific distribution in
healthy pregnant women
The individual plotted values (filled circles) represent the results in the 23
pregnancy cases with positive TPO-Ab of whom there were two (8.6%) value in the first trimester, and 4 (17.3%) value in both second and third trimester clearly outside (to the right) of the 97.5 percentile range of serum
TSH concentration for TPO-Ab negative pregnant women.
A linear relationship between the log transformed TSH and FT4 values
during pregnancy was observed (Figure 3.1.2.6).
55
First trimester lnFT4
3,2
A
3,0
2,8
2,6
-6,0
-4,0
-2,0
0,0
2,0
First trimester lnTSH
Second trimester lnFT4
3,2
B
3,0
2,8
2,6
2,4
-6,0
-4,0
-2,0
0,0
2,0
Second trimester lnTSH
Third trimester lnFT4
3,2
C
3,0
2,8
2,6
2,4
2,2
2,0
-6,0
-4,0
-2,0
0,0
2,0
Third trimester lnTSH
Figure 3.1.2.6. Scatter plots of TSH vs. FT4 (based on logarithmicallytransformed value) at 12–16 (A), 22–26 (B) and 32–36 (C) week of gestation in pregnant women with normal (open circle, n=161) and elevated
(filled circle, n=23) TPO-Ab concentrations (>35 IU/ml) in the three trimesters of pregnancy
56
Correlations between the two hormone concentrations were moderate in
the first trimester (A) at 12–16 wk (r2=0.125, r=–0.356, p<0.001) and weak
in the two others: (B) at 22–26 week (r2=0.045, r=–0.21, p=0.004) and (C)
at 32–36 week (r2=0.018, r=–0.136, p=0.066) indicating that FT4 concentrations were poorly predicted by TSH concentrations during second and
third trimesters of pregnancy (Figure 3.1.2.6).
3.1.3. Effect of thyroid peroxidase antibodies on thyroid stimulating
hormone reference limits
TSH and FT4 reference ranges were calculated when TPO-Ab positive
patients were included in reference population.
Table 3.1.3.1. TSH, FT4 – median, 2.5th and 97.5th percentiles in the
pregnant women after including those positive for thyroid peroxidase (TPOAb) antibody (N=184)
TSH, mIU/L
FT4, pmol/L
Trimester of gestation
Trimester of gestation
1st
2nd
3rd
1st
2nd
3rd
Median
0.76
0.96
0.92
17.00
14.50
13.85
2.5 percentile
0.02
0.24
0.28
13.20
11.80
10.50
97.5 percentile
2.91
2.82
2.52
22.66
18.54
17.93
TSH, thyroid stimulating hormone; FT4, free thyroxine
The lower TSH reference limit was not affected by the inclusion of TPOAb positive women, but resulted in higher upper reference limits during
pregnancy. On including the 23 pregnancies cases with positive TPO-Ab,
the 97.5 percentiles for TSH increased to 2.91, 2.82 and 2.52 mIU/L, respectively (Table 3.1.3.1).
In pregnant women without a history of thyroid disease the median, 2.5
and 97.5 percentiles for TSH (mIU/L) were 0.70 and 0.02–2.72 (first trimester), 0.93 and 0.22–2.51 (second trimester), 0.91 and 0.28–2.36 (third
trimester). On including women with positive TPO-Ab, the 97.5 percentiles
for TSH increased to 2.91, 2.82 and 2.52 mIU/L, respectively.
3.2. The newborn thyroid stimulating hormone (Study II, III)
The data obtained for newborn TSH showed Gaussian distribution, enabling the paired t test to be used to compare the mean measurements. Histo-
57
gram showing the Gaussian distribution of newborns TSH (K–S test p=0.1)
is presented (Figure 3.2.1).
40
Frequency
30
Mean =3,13
Std. Dev. =1,046
N =173
20
10
0
0,00
1,00
2,00
3,00
4,00
5,00
6,00
Newborn TSH
Figure 3.2.1. Histogram showing the Gaussian distribution of newborns
TSH, mIU/L (Kolmogorov–Smirnov test, p=0.1)
The study sample consisted of 173 newborns. The median, interquartile
ranges, range of the TSH at the third day of life, gestational age and birth
weight of the 96 male and 77 female newborns are presented in Table 3.2.1.
There was 1 (1.1%) male newborn born at <37 weeks of gestation (maternal
age 21 year, gestational age 35 week, birth weight 2176 g, TSH 2.21
mIU/L). Two newborns, one female and one male, were with birthweight
less than 2500 g. The values of TSH were 2.21 (female, gestation age 39
week, birth weight 2176 g, Apgar 9 at 5 minutes) and 3.47 mIU/L (male, 36
week, 2176 g, Apgar 9 at 5 minutes). There was no gender effect of newborns on birthweight (F(1,172)=2.4; p=0.121).
Table 3.2.1. Descriptive continuous data showing the median, IQRa and
range (minimum and maximum values) for newborn TSH, birthweight and
gestational age in male and female infants
All (N=173)
mediana
IQR (range)
TSH, mIU/L
3.23
2.55–3.79 (0.23–6.03)
Birthweight, g
3540
3265–3832 (2176–4650)
40
39–40 (35–41)
Gestation, weeks
58
Table 3.2.1. (continued)
Males (M) N=96
mediana
TSH, mIU/L
3.38
Birthweight, g
3586
Gestation,
weeks
40
pb
Females (F) N=77
IQR (range)
3.26–3.95
(0.23–6.03)
3307–3880
(2176–4650)
mediana
39–40 (35–41)
40
3.12
3500
IQR (range)
2.28–3.59
(1.05–5.37)
3230–3722
(2176–4410)
M vs. F
39–40 (37–41)
0.284
0.054
0.075
TSH, thyrotrophin
a
IQR, interquartile range, the range from the 25th to 75th percentile
b
Mann–Whitney tests
In study III, IV, V 125 women had vaginal delivery and 44 (25%) underwent cesarean section. Newborn delivery mode data are presented Table
3.2.2.
Mean (SD) infant weight was 3.55 (0.45) kg, mean newborn TSH was
3.1 mIU/L (SD 1.0). The median concentrations (and interquartile ranges) of
TSH in babies born by Cesarean section (25%), was 3.19 (IQR 1.37)
mIU/L. This value was not significantly different from the corresponding
ones in babies born by normal vaginal delivery (p=0.73) (Table 3.2.2)
Table 3.2.2. Newborn TSH according to the mode of delivery
Newborn TSH N=173
Delivery type
IQRa
Median
N (%)
Normal vaginal
3.33
1.37
125 (72.7)
Vacuum extraction
2.37
1.54
4 (2.3)
Cesarean section
3.19
1.22
44 (25.0)
Emergency cesareanb
3.53
1.14
28 (16.2)
Elective cesarean
2.8
1.9
16 (9.2)
Cesarean section, N=44
Breech presentation
2.6
1.9
5 (2.8)
IQR, interquartile range, the range from the 25th to 75th percentile
b
Mann-Whitney U test between acute and elective cesarean section p=0.056
a
TSH in babies delivered by emergency Cesarean section tended to be
higher than in delivered by elective Cesarean section (median, 3.53 versus
2.8 mIU/L, p=0.056). The differences of TSH concentration in babies
59
delivered by normal, vacuum extraction or Cesarean section were not
significant (KruskalWallis test p=0.18) (Table 3.2.2).
The mode of delivery does not have considerable influence on TSH in the
newborns, although minor differences exist. The mean serum TSH level
following elective cesarean section was lower (but not significantly) than
after normal vaginal delivery.
All newborn TSH values were below cut–off value for congenital hypothyroidism (10 mIU/L). The prevalence of newborn thyrotropin >5 mIU/L
(%) was 2.8 % (four males and one female). The values were from 5.03 to
6.03 mIU/L. Figure 3.2.2 shows cumulative frequencies of TSH values.
Cumulative Percent
100
80
60
40
20
0
0
1
2
3
4
5
6
7
Newborn TSH, mIU/l
Figure 3.2.2. Cumulative frequency of the TSH of the newborns
The distribution of TSH was close to statistical significance different between males and females, with males tended to have a higher median TSH
(3.38 compared with 3.12 in females, p=0.054).
Median (range) first minute Apgar score was 9 (6–10) and fifth minute
was 9.5 (8–10). Apgar scores at 1 minute were not related to neonatal TSH,
however, there was Apgar scores at 5 minutes effect on TSH (gender adjusted F(2,162)=4.9; p=0.027). Infants with Apgar of ≤8 at 5 minutes had higher levels of TSH as compared to those with Apgar of 9–10 at 5 minutes
(mean 3.78 ± 1.02 and 3.06 ± 1.04, respectively; p=0.027).
60
3.2.1. Iodine deficiency assessed by the newborn TSH concentrations
(Study II)
Whole-blood TSH values were available for 213 newborns. TSH value
ranged 0.23–6.03 mIU/L, with a median of 3.23 (interquartile range, 1.17
mIU/L), mean (SD) - 3.14 (0.99). A total of 6 newborns (2.8%) had TSH
values >5 mIU/L.
Age-specific 2SD range (mean ± 2SD) necessary for interpretation of
newborn TSH levels at the third day of life was established 1.15–5.13
mIU/L.
3.2.2. The newborn TSH levels in relation to maternal age, gestation,
birthweight and gender (Study III)
Mean newborn TSH, mUI/l
The descriptive newborn data, medians and interquartile ranges (IRQ) are
presented in Table 3.2.1.
An effect of gestational age on TSH levels was established at the p-value
below 0.1 (=0.14, p=0.07). Gender specific analyses showed that gestational age was not correlated with TSH levels when stratified by gender
(p=0.41 and 0.33 for males and females, respectively).
3,25
3,00
2,75
2,50
2,25
35
36
37
38
39
40
41
Gestational age, week
Figure 3.2.2.1. Thyroid stimulating hormone (TSH) value in infants with
different gestational age
There were also no effects of birth weight on newborn TSH levels
(=0.02, p=0.871). Two newborns were lighter than 2500 grams at birth.
61
The values of TSH were 2.21 (female, gestation age 39 week, birthweight
2176 g) and 3.47 mIU/L (male, 36 week, 2176 g).
Newborn TSH levels were associated with maternal age (=0.17,
p=0.029). Spearman rank correlation analysis showed a significant positive
correlation between birth weight and gestational age (=0.398, p<0.001).
Sex–specific analyses showed similar correlation coefficients as for the
combined analysis (p<0.001 and p=0.006 for males and females, respectively). There was no gender effect of newborns on birthweight (F(1,168)=2.4;
p=0.121) and on maternal age (F(1,168)=1.1; p=0.287). Gestational age correlated significantly with maternal age (=0.15, p=0.032) and birth weight
(=0.33, p<0.001).
Multivariate analyses. Since birth weight is dependent on gestational age,
we conducted a multivariate analysis simultaneously to examine the relationship between neonatal TSH levels and maternal age (modeled continuously), newborn gender, gestational age and birth weight. The outcome variable in the analysis was the TSH level and the results are shown in Table
3.2.2.1. The model (F(3,170)=2.99; p=0.020) showed a significant adjusted
associations with TSH levels for maternal age (p=0.022) and gestational age
(p=0.035), but not for birth weight (p=0.267), and newborn gender
(p=0.086).
Table 3.2.2.1. Adjusted coefficients for factors simultaneously included in a
multiple linear regression model with the newborn TSH as the outcome variable
Factor
Beta ()
p
Maternal age, year
0.18
0.022
Gestational age, week
0.18
0.035
Gender (1, female; 2, male)
0.13
0.086
Birth weight, g
–0.09
0.267
Dependent variable: newborn TSH; – standardized regression coefficient
R2 adjusted = 0.069; p<0.02
Adjusted for maternal age, child gender, gestational age, and birth weight
Gestational age was associated with TSH level in multivariate but not in
univariate models. Positive association between maternal age and newborn
TSH levels persisted in both univariate and multivariate models. In this
model for TSH levels, the inclusion of all predictive covariates explained
6.9% of the total variation.
62
Linear multivariate regression analysis was performed in order to test
the relationships between TSH level, newborn birth weight, newborn gender, and gestational age yielded the following regression equation:
TSH (mIU/L) = [–0.00022 (p = 0.27) x birth weight (g)] + [0.182 (p =
0.035) x gestational age (weeks)] + [0.038 (p=0.022) x maternal age (years)]
+ [0.279 (p = 0.086) x gender (1, female; 2, male)] – 4.86 (R2 = 0.069).
The effect of birth weight and newborn gender was not significant.
3.2.3. The newborn TSH levels in relation to maternal thyroid function
When the neonatal and maternal thyroid function was compared (173
pair mother–newborn) the median neonatal serum concentrations of TSH
were significantly higher than the maternal values in all trimesters of
pregnancy (all p<0.001) (Table 3.2.3.1).
Table 3.2.3.1. Maternal and infant thyroid functioning
Variable
(N = 173)
Mean maternal FT4 first trimester (SD)
17.12 (2.27)
Mean maternal TSH first trimester (SD)
0.91 (0.7)
Prevalence of TPO–Ab >35 U/mL, %
12.5
Mean maternal FT4 second trimester (SD)
14.55 (1.73)
Mean maternal TSH second trimester (SD)
1.12 (0.65)
Mean maternal FT4 third trimester (SD)
13.93 (1.78)
Mean maternal TSH third trimester (SD)
1.04 (0.56)
TSH of infant heel blood sample
3.13 (1.00)
Notes: Maternal serum TSH (based on square root–transformed value) and serum FT4
(arithmetic means) concentrations
Mean maternal FT4 at 2nd trimester was higher in women who delivered
male than female newborns (14.6 and 14.2 pmol/L, respectively; p=0.011).
There were no significant correlations between TSH of infant heel blood
samples and maternal TSH (both square root and log transformed) and FT4
in the first, second, or third trimester. Infant heel blood samples for TSH
were significantly correlated with gestational age (r=0.2; p=0.042) but not
with TPO-Ab, gender, and birth weight.
Gestational age and birth weight were also highly intercorrelated in newborns. Therefore, only the former was included in multiple regression mod-
63
els, where appropriate, because it was a better predictor of TSH concentrations. The data were analysed by multiple regression using as regressors maternal age, gestational age, birth weight, sex, the maternal concentrations of
TSH or FT4 during all three trimesters and TPO-Ab measured in early
pregnancy (modeled categorical: negative and positive). The overall relationship was significant (F(3,170)=2.79, p<0.05) only for model with maternal and gestational age, and maternal TPO-Ab as regressors. The effect of
maternal and gestational age on newborn TSH was significant (t173=2.02,
p<0.05 and t173=2.18, p<0.05, respectively). Controlling for maternal TSH
and FT4 the models were not statistically significant.
Table 3.2.3.2. Adjusted coefficients for factors included in a multiple linear
regression model with the newborn TSH as the outcome variable
Modela
Factor
1
(Constant)
t
Sig.
–1.034
0.302
Maternal age, years
0.149
1.984
0.049
Gestational age, wk
R2 = 0.032
F = 3.858 p = 0.023
2
(Constant)
0.153
2.038
0.043
–1.200
0.232
Maternal age, years
0.152
2.018
0.045
Gestational age, wk
0.170
2.182
0.031
–0.065
–0.834
0.406
TPO–Ab, negative
R2 = 0.049
F = 2.79 p = 0.038
a
Standardized
coefficients
Beta
Dependent variable: newborn TSH; model 2 adjusted for maternal TPO-Ab
In this study of 173 children born with normal thyroid function, we saw
no evidence that newborn TSH concentrations were associated with maternal TSH, FT4, or elevated TPO-Ab.The effect of maternal and gestational
age on newborn TSH was significant.
64
3.3. Maternal thyroid function during pregnancy in the interference
with anthropometric parameters of newborn
A total of 173 birth delivery medical case histories were analyzed. Correlation analysis (Table 3.3.1 by variable) revealed that gestational age and all
maternal anthropometric measurements (and BMI) were positively correlated (p<0.01) with birth weight and height. Older maternal age was related to
greater maternal BMI (but not to weight and height separately).
Table 3.3.1. Correlations between the primary variables
Weight, kg
Newbornweight
1
Newborn
height
0.57**
0.02
Maternal
age
0.12
Gestation
age
0.35**
Height, cm
0.57**
–0.002
0.06
0.08
0.35**
–0.07
Apgar 1.
–0.002
1
0.68**
0.11
0.04
0.01
Apgar 5
Maternal age,
years
Gestational age,
years
Gender (1, female; 2, male)
Maternal BMI
Maternal height,
cm
Pre–pregnancy
Weight, kg
Weight gain,
kg/week
0.02
0.06
0.68**
1
0.16*
0.05
0.02
0.12
0.08
0.11
0.16*
1
–0.10
0.52**
0.28**
0.31**
0.04
0.05
–0.10
1
–0.07
0.11
0.11
–0.06
0.004
0.07
–0.04
–0.04
0.21**
0.17*
–0.05
–0.08
0.162*
0.01
–0.03
0.21**
0.14*
0.06
–0.04
–0.08
0.08
–0.08
0.29**
0.22**
–0.02
–0.09
0.11
0.04
–0.03
0.26**
0.11
0.02
–0.06
–0.13
0.01
-0.13
Apgar
1 min.
Apgar
5 min.
0.06
1
0.05
Paritya
–0.08
parity, 0 – nullipara, 1 – multipara
** Correlation is significant at the 0.01 level (2–tailed).
* Correlation is significant at the 0.05 level (2–tailed).
a
The results of univariate linear regression analysis of the associations of
birthweight with maternal TSH and FT4 levels by trimesters (n=173) are
shown in Table 3.3.2.
65
Table 3.3.2. Univariate analysis of the relationship of birthweight with maternal thyroid function parameters by trimesters (n = 173)
Maternal TSHa
Maternal FT4
β
Sig.
β
Sig.
1st
–0.09
0.23
0.06
0.47
2nd
0.02
0.82
–0.16
0.036
3rd
–0.05
0.51
–0.12
0.12
Trimester
Dependent variable: newborn birthweight; – standardized regression coefficient
a
after square root transformation
Newborn birthweight, g
Of maternal thyroid function parameters only FT4 concentration at 2nd
trimester was negatively correlated with newborn birthweight (β=–0.16,
p=0.036).
5000
4500
4000
3500
3000
2500
R Sq Quadratic
=0,053
2000
15
20
25
30
35
40
45
Maternal age, year
Figure 3.3.1. Relationship between maternal age and newborn birthweight
(filled circle, male gender)
66
Newborn birthweight, g
5000
R Sq Quadratic =0,107
4500
4000
3500
3000
2500
2000
35
36
37
38
39
40
41
Gestational age, week
Newborn birthweight, g
Figure 3.3.2. Relationship between maternal age (above), gestational age
(bottom) and birthweight (filled circle, male gender)
5000
4500
4000
3500
3000
2500
R Sq Quadratic
=0,137
2000
50
60
70
80
90
100
110
120
Pre-pregnancy weight, kg
Figure 3.3.3. Relationship between maternal pre–pregnancy weight and
birthweight
In the multivariate models for predicting newborn antropometric and maternal thyroid function parameters (TSH and FT4) in all trimesters of pregnancy, linear and quadratic terms (a quadratic term for gestational age and
for maternal age was included in the final analysis to improve model fit) of
maternal age at the time of delivering the birth (Figure 3.3.1–3.3.3), number
of gestations, duration of pregnancy, gender and TSH of the newborn were
used as independent variables.
67
Table 3.3.3. Multiple linear regression analysis of newborn birth weight,
height, BMI and Apgar
Betaa
t
Sig.
0.240
3.606
0.000
FT4 concentration at 2nd trimester, pmol/L
–0.134
–2.014
0.046
Maternal age, year
–1.338
–2.055
0.041
Gestational age, week
7.404
2.543
0.012
Quadratic term of maternal age
1.413
2.170
0.031
Quadratic term of gestational age
Birth height
R2 = 0.194, adjusted R2 = 0.176
F (4,172) = 10.38 p<0.001
Maternal age, year
–7.068
–2.427
0.016
–1.519
–2.258
0.025
Quadratic term of maternal age
1.679
2.494
0.014
Gestational age, week
0.363
5.289
0.000
0.146
2.107
0.037
–0.149
–2.071
0.040
Gestational age, week
6.447
2.076
0.039
Pre–pregnancy weight, kg
0.208
2.898
0.004
Quadratic term of gestational age
Apgar 1 score
R2 = 0.067, adjusted R2 = 0.046
F (4, 172) = 3.1 p = 0.017
TSH concentration at 1st trimestre, mIU/L
–6.291
–2.026
0.044
0.156
2.101
0.037
FT4 concentration at 3rd trimestre, pmol/L
0.137
1.822
0.070
Gestational age, year
8.224
2.564
0.011
–8.253
–2.572
0.011
0.230
3.08
0.002
Model
Birth weight
R2 = 0.265, adjusted R2 = 0.239
F (6,170) = 10.76 p<0.001
Pre–pregnancy weight, kg
Weight gain, kg
Newborn‘s BMI
R2 = 0.119, adjusted R2 = 0.099
F (4,172) = 5.81 p<0.001
FT4 concentration at 2nd trimester, pmol/L
Quadratic term of gestational age, week
Apgar 5 score
R2 = 0.143, adjusted R2 = 0.122
F (1, 175) = 10.07 P < 0.002
Maternal age, year
a
standardized coefficient; BMI, body mass index
68
Multivariate regression with backward elimination (Table 3.3.3.) revealed that gestational age (β=7.4, p=0.012), pre–pregnancy weight (β=0.24,
p<0.001) were the strongest positive predictors of birth weight and FT4
concentrations in the 2nd trimester of pregnancy (β=– 0.134, p=0.046) was
negative predictor and together with maternal age and quadratic term for
gestational age covered 23.9% of variance.
Weight gain of mother during pregnancy was a better predictor of newborn height than pre-pregnancy weight (β=0.146, p=0.037). Gestational age
(β=0.363, p<0.001) was the strongest positive predictor of height of newborn whereas FT4 concentrations in the 2nd trimester of pregnancy (β=–
0.149, p=0.040) was negative predictor of neonatal BMI and together with
gestational age and pre–pregnancy weight covered 10% of variance.
Regardless of the Apgar scores in 5th postpartum minutes of extrauterine
life the protective effect of maternal age was observed as significant
(β=0.23, p=0.002) and covered 12% of variance.
One of the thyroid function measurements, FT4 (but not TSH) concentration at 2nd trimester of pregnancy, was negatively affecting birth weight and
BMI. TSH concentration at 1st trimester was positively associated with Apgar scores at first minute.
3.4. Antenatal maternal personality and mental state and
anthropometric characteristics of the newborns (Study IV, V)
Symptoms of depression (EDS≥12) were found in 17 (9.8%) women in
the first trimester of pregnancy, in 8 (4.6%) women in the second trimester
of pregnancy and in 12 (6.9%) women in the third trimester of pregnancy.
The differences in the prevalence of depressive disorder in the three phases
of pregnancy were not statistically significant (2=5.08, df=2, p=0.079).
Of the all 173 women 146 (84.4%) did not perceive symptoms of depression during pregnancy, 20 (11.6%) were established as having symptoms of
depression at least one trimester, 4 (2.3%) – at two trimesters, and 3 (1.7%)
– at all three trimesters (Figure 3.4.1).
Symptoms of anxiety (45 and a more score in STAI) were found in 32
(18.5%), in 23 (13.3%) and in 17 (9.8%) pregnant women in the first, second and third trimesters of pregnancy, respectively. The differences in the
decreasing prevalence of symptoms of anxiety in the three phases of pregnancy were statistically significant (2=8.77, df=2, p=0.012).
Of the all 173 women 128 (74%) did not perceived symptoms of anxiety
during pregnancy, 24 (13.9%) were established as having symptoms of anx-
69
Percent
iety at least one trimester, 15 (8.7%) – at two trimesters, and 6 (3.5%) – at
all three trimesters (Figure 3.4.1).
100
80
60
40
20
0
74
84.4
No
13.9 11.6
8.7 2.3
3.5 1.7
At least one
trimester
At two
trimesters
At all trimesters
Symptoms of anxiety
Symptoms of depression
Figure 3.4.1. Frequency of perceived symptoms of anxiety and depression
during pregnancy
The differences in severity of acute stress among the three trimesters of
pregnancy were not statistically significant (Friedman test, p=0.08). Severity
of chronic stress was higher at first trimester, then decreased during second
and then remained stable in the third (Friedman test, p<0.001).
27.2
30
Percent
25
20.2
16.2 17.3
20
15
12.7 13.9
Acute stress
Chronic stress
10
5
0
First
Second
Third trimester
Figure 3.4.2. Frequency of perceived acute and chronic stress during
pregnancy
Of the all 173 women 35 (20.2%) at first trimestre, 28 (16.5%) at second,
and 22 (12.7%) at third were established as having acute stress, and 47
(27.2%), 30 (17.3%), 24 (13.9%) as having chronic stress, respectively
(Figure 3.4.2).
70
40
31.5
27.7
30
Score
35.3
33.1
23.5
20
10
0
Extroversion
Agreeableness Consciousness
Neuroticism
Openness
Figure 3.4.3. Maternal Big-Five personality dimensions (range 8–40,
measured in the second trimester of pregnancy)
Personality dimensions (Figure 3.4.3) were not significantly associated
with both perceived acute or chronic stress. Conscientiousness was negatively related to depression and anxiety symptomology during pregnancy.
Neuroticism was strongly related to anxiety and moderately to depression;
extraversion was inversely associated with anxiety during pregnancy (Table
3.4.1)
Table 3.4.1. Big-Five personality dimensions relation with perceived symptomology of depression (by EDS) and anxiety (by STAI) by trimester of
pregnancy
1st
trimester
-0.09
EDS
2nd
trimester
-0.09
3rd
trimester
-0.06
1st
trimester
-0.30**
STAI
2nd
trimester
-0.25**
3rd
trimester
-0.19*
Agreeableness
-0.16*
-0.16*
-0.14
-0.13
-0.14
-0.20*
Conscientiousness
-0.18*
-0.18*
-0.2*
-0.29**
-0.32**
-0.29**
Neuroticism
0.40**
0.46**
0.36**
0.62**
0.67**
0.59**
-0.10
-0.09
-0.15*
-0.21**
-0.16*
Extraversion
Openness
-0.03
* p<0.05; ** p<0.01
The chronic stress in the second trimester correlated with newborn birthweight (r=0.17, p=0.025) and perceived acute stress in the third trimester
correlated with Apgar scores in 5th minutes (r=–0.17, p=0.029).
71
We evaluated five maternal personality traits, but only one, namely conscientiousness, was positively associated with newborn birthweight and
height (r=0.15 and r=0.22, respectively).
Multivariate analysis
Five separate regression models were created for neonatal weight, height,
BMI and Apgar scores in the 1st and 5th minutes of extrauterine life using
as regressors maternal age and pre-pregnancy weight, parity, gestational
age, maternal TSH and FT4 concentration, perceived symptoms of depression and symptoms of anxiety, perceived acute and chronic psychosocial
stress in all three trimesters of pregnancy and personality traits in the second
trimester of pregnancy (Table 3.4.2).
Gestational age (β=0.304, p=0.00) and chronic stress in the 2nd trimester of
pregnancy (β=0.276, p=0.001) were the strongest positive predictors whereas chronic stress (β=-0.191, p=0.019) and FT4 concentration (β=-0.145,
p=0.028) in the 3rd trimester of pregnancy were the strongest negative predictors of birth weight and together with other significant variables covered
31% of variance (Table 3.4.2). Conscientiuosness score in the 2nd trimester
and EDS score in the 1st trimester of pregnancy were weak positive predictors of birth weight (β=0.154, p=0.019 and β=0.143, p=0.033; respectively).
Gestational age (β=0.338, p=0.000) and Conscientiuosness score
(β=0.201, p=0.005) were the strongest positive predictors of birth height and
together with other significant variables covered 19% of variance.
Pre-pregnancy weight of mother (β=0.210, p=0.004), chronic stress in the
2nd trimester of pregnancy (β=0.207, p=0.018) and EDS score in the 1st
trimester of pregnancy (β=0.174, p=0.015) were the strongest positive predictors of BMI of newborns whereas chronic stress in the 3rd trimester of
pregnancy (β=-0.198, p=0.023) and FT4 concentrations in the 3rd trimester
of pregnancy (β=-0.165, p=0.023) were negative predictors of neonatal BMI
and together with gestational age covered 15% of variance.
Anxiety score in the 3rd trimester of pregnancy (β=0.305, p=0.001), maternal age (β=0.268, p=0.000) and neuroticism score (β=0.267, p=0.004)
were positive predictors whereas acute stress in the 3rd trimester of pregnancy (β=-0.177, p=0.016) was negative predictor of Apgar score in the 5th
minute of extrauterine life and covered 14% of variance.
72
Table 3.4.2. Multiple linear regression analysis of newborn birth weight,
height, BMI, Apgar scores
Beta, β
Model
Birth weight
R2 = 0.349, adjusted R2 = 0.309
F (10,161) = 8.630 p<0.001
Maternal age
t
Sig.
-1.729
-2.656
0.009
Quadratic term of maternal age
1.806
2.779
0.006
Gestational age
0.304
4.680
0.000
Chronic stress at 2nd trimester
0.276
3.458
0.001
Pre-pregnancy weight
0.221
3.368
0.001
Chronic stress at 3rd trimester
-0.191
-2.360
0.019
Big Five Conscientiousness score
0.162
2.463
0.015
EDS score at 1st trimester
0.154
2.377
0.019
FT4 concentration at 3rd trimester
-0.145
-2.213
0.028
Acute stress at 2nd trimester
Birth height
R2 = 0.211, adjusted R2 = 0.192
F (4,167) = 11.182 p<0.001
Maternal age
0.143
2.153
0.033
-1.843
-2.648
0.009
Quadratic term of maternal age
1.965
2.827
0.005
Gestational age
0.338
4.883
0.000
Big Five Conscientiousness score
Newborn‘s BMI
R2 = 0.175, adjusted R2 = 0.145
F (6,165) = 5.822 p<0.001
Pre-pregnancy weight, kg
0.201
2.879
0.005
0.210
2.917
0.004
Chronic stress at 2nd trimester
0.207
2.382
0.018
Chronic stress at 3rd trimester
-0.198
-2.292
0.023
EDS score at 1st trimester
0.174
2.458
0.015
FT4 concentration at 3rd trimester
-0.165
-2.289
0.023
Gestational age
Apgar 5 score
R2 = 0.143, adjusted R2 = 0.122
F (4, 167) = 6.949 P < 0,001
Anxiety score at 3rd trimester
0.159
2.216
0.028
0.305
-3.426
0.001
Maternal age
0.268
3.651
0.000
Big Five Neuroticism score
0.267
2.940
0.004
Acute stress at 3rd trimester
-0.177
-2.436
0.016
73
4. DISCUSSION
4.1. Longitudinaly assessed maternal thyroid axis changes during pregnancy and comparisons of reference intervals
This longitudinal cohort study examining the pattern of serum TSH concentrations and FT4 concentrations in three trimesters of pregnancy in
healthy, TPO-Ab negative women confirmed that thyroid axis hormone reference interval differs from assay specific referral ranges used in nonpregnant populations, supporting recommendations that trimester-specific
reference ranges should be used (77). Moreover, changes in thyroid status in
healthy Lithuanian women during pregnancy can be compared to similar
studies for an in-land geopgraphical area. The second and third trimesters
upper reference limit found in our study corresponds to the TSH ranges proposed by the Endocrine Society Pregnancy Guidelines (8) and falls below
3.0 mIU/L. Though, our upper reference limit 2.72 mIU/L for the first trimester is higher than 2.5 mIU/L proposed by the Endocrine Society Pregnancy Guidelines.
Misdiagnosis of thyroid dysfunction during pregnancy may be crucial for
mother and for child (248) (19). There is a controversy over the most
reliable reference interval and cuff-of values to differentiate normal thyroid
function from abnormality associated with thyroid dysfunction (127). In
clinical practice, several parameters have been identified to represent useful
markers of thyroid function during pregnancy, including changes in serum
TSH and in serum FT4 concentrations (305). During early pregnancy TSH
secretion is suppressed by hCG induced by thyroid gland stimulation (79).
During the second half of gestation, serum TSH concentrations return progressively to pre-pregnancy values and remain stable, unless additional underlying factors cause thyroid dysfunction. For instance, iodine deficiency
or autoimmune thyroid disease may cause thyroid insufficiency resulting in
progressive increase in serum TSH concentrations (306). Specifically, both
the Belgian (78) and Danish (307) studies carried out in well defined areas
with a marginal iodine deficiency, have showed an increase in serum TSH
near term. The same investigators proved that iodine supplementation
during pregnancy significantly prevented these alterations in serum TSH.
Conversely, a Dutch study performed in an iodine replete area failed to
show a discrepancy in serum TSH between the third trimester and
nonpregnant values (308).
Using the assay specific reference interval for serum TSH one might suspect hyperthyroidism in normal women who have a low serum TSH value
74
early in pregnancy, and one might miss hypothyroidism in women who have
a slight TSH elevation (205). With the assay specific reference interval for
TSH almost a quarter of pregnant women might be incorrectly diagnosed
with hyperthyroidism in the first trimester of pregnancy. In the second and
in third trimesters some women would also have been classified wrongly.
Similar findings have been noted by Dashe et al. (139).
A direct comparison of our reference intervals to other published data is
problematic for several reasons. Selection of normal subjects may account
for variations in reference interval by different authors, despite the use of
the same methodology for testing (137). The establishment of reference
interval can be influenced significantly by age, ethnicity, season, cigarette
smoking, exercise, sleep deprivation, fasting, phlebotomy timing, methods
of analysis, iodine status, selection of subjects and calculation method (99,
120, 137, 309-313).
There is evidence that serum TSH concentration decreases markedly during the morning from 8:00 to 9:30 AM, thereafter the concentration remains
relatively constant until evening, with a smaller nadir in the late afternoon
(314). In this respect we performed blood sampling, trying to eliminate the
effect of diurnal TSH variation. As time of sampling is unknown in most
studies (315), sampling time differences between studies may be an
important reason for the differencies in published reference intervals. We
obtained reference interval for FT4 and TSH from healthy and ethnically
homogeneous pregnant women, as reference values tend to vary according
to the ethnic group (99-100, 316). TSH concentrations decrease significantly
in twin pregnancies compared to singleton during the first trimester (139).
Therefore, only singleton pregnancies were included in our assessment. As
FT3 was not measured, the full range of thyroidal metabolism during pregnancy could not be evaluated and hormonal measurement even earlier in the
first trimester would have been of interest. Although our hormonal change
observations were limited to the late first assessment (12–16 weeks), TSH
reached a nadir in the first trimester, while later on, in the pregnancy, values
increased, as been noted by other researchers (316). TSH suppression is associated with the elevation in circulating hCG (78-79, 317-318), peaking at
around 11-12th gestational week, whereas estrogen production increases the
mean TBG concentration 2–3 times the pre-pregnancy level by 16 to 20
weeks of gestation (23, 319), causing a shift in total T4 to approximately 1.5
times the non-pregnant level by 16 weeks (3, 23, 78). The latter, could partially explain our relatively high upper FT4 reference interval at 12–16
weeks or it might be the effect of iodine containing vitamine use during
pregnancy, though we cannot provide the data on extent of their usage. Our
lower FT4 reference interval was comparable to the study in Spain at 11–20
75
weeks (13.2 vs 13.1 pmol/L, respectively), but our upper limit was still
higher (23.1 vs 17.24 pmol/L, respectively) (320). First, trimester median
FT4 values were 16.9 and 19.9 pmol/L, respectively, for the nonsupplemented and potassium iodide supplemented women from the area of
mild iodine deficiency in Spain (321).
Variations in reference interval for TSH and FT4 might be observed due
to inclusion of different gestational weeks in trimesters and calculation
methods used, also different manufacturer methods used.
There was a dearth of comparable data available in the literature because
of many different methods used to calculate reference intervals. Reference
intervals for TSH and FT4 varied according to different manufacturer methods and between authors, even when the same manufacturer method was
applied. Table 4.1.1 shows the comparisons of reference intervals for TSH
and FT4 between different authors and different manufacturer methods used
for analysis. All reference intervals are trimester-based, and the same calculation method (i.e. a central 95% interval with the 2.5th and 97.5th percentile values) was used with the exception of three authors who used 5th and
98th percentile values, and 5th and 95th percentiles, respectively.
Compared with other authors, our data revealed a relatively lower cut–off
values for the upper TSH reference limit, in particular when compared with
the data reported by the authors that used the Immulite platforms. Some variations were also found in FT4 reference intervals. Our FT4 reference intervals had higher cut-off values (11.8–18.5 pmol/L) compared with the data
reported by Lambert-Messerlian et al. (9.3–16.2 pmol/L), particularly during the second trimester.
Our reported reference interval, especially lower TSH and higher FT4
values in the first trimester is close to the ones observed from a previously
mildly iodine-deficient area in Italy by Moleti et al. (322), in Spain by Boccos-Terraz et al. (320) and in China by Panesar et al. (81), compared to other authors (26, 38, 135, 323). The biggest disparity in the upper values of
TSH reference intervals was oberved in the above mentioned studies. Moreover, there are differences in reference intervals between authors, even when
the same manufacturer method is applied, described by Yan et al. (137). We
used Immulite analyzer and revealed lower TSH and higher FT4 reference
intervals than described by two studies (136, 323) using the same analyzer.
76
Table 4.1.1. Comparisons of trimester–specific reference intervals for TSH
and FT4 (data were calculated as 2.5th and 97.5th percentiles)
Trimester of pregnancy
Method used, authors
Immulite 2000 analyzer
Haddow et al. (USA, 2004)a
Lambert–Messerlian et al.
(USA, 2008) a
Abbott ARCHITECT
analyzer
i2000
Stricker et al. (Switzerland,
2007)
Analyte
1st
2nd
3rd
Manufacturer’s reference interval for nonpregnant adults:
TSH:0.4–4.0 mIU/L; 10.3–24.5 pmol/L
TSH
0.08–3.61
0.39–3.71
TSH
0.12–3.37
0.35–3.35
FT4
10.4–17.8
9.3–16.2
Manufacturer’s reference interval for nonpregnant adults:
TSH:0.35–4.94 mIU/L; 9.0–19.1 pmol/L
TSH
0.09–2.83
0.20–2.79
0.31–2.90
FT4
10.5–18.3
9.5–15.7
8.6–13.6
Boccos et al. (Spain, 2009)
TSH
0.03–2.57
0.12–2.64
0.23–3.56
Gilbert et al. (Australia, 2009)
TSH
0.02–2.15
FT4
10.4–17.8
TSH
0.07–3.20
Mannisto et al. (Finland, 2011)
Roche Elecsys 1010/2010 or
Roche Modular E170
Marwaha et al. (India,2008)b
Gong et al. (Canada, 2008)
ACS:180; Chiron Diagnostics
Corporation, East Walpole,
MA, USA
Panesar et al. (Hong Kong,
China, 2001)
Bayer ADVIA Centaur analyzer
Springer et al. (Czech
Republic, 2009)
Yan et al. (China, 2010)
0.35–3.32
FT4
11.86–21.85
11.2–18.86
Manufacturer’s reference interval for nonpregnant adults:
TSH:0.27–4.20 mIU/L; 12.0–22.0 pmol/L
TSH
0.6–5.0
0.44–5.78
0.74–5.7
FT4
12–19.45
9.48–19.58
11.3–17.71
FT4
11–19
9.7–17.5
8.1–15.3
Manufacturer’s reference interval for nonpregnant adults:
TSH:0.3–4.0 mIU/L; 10.2–19.0 pmol/
TSH
0.03–2.3
0.03–3.1
0.13–3.5
FT4
11.1–22.9
8.1–16.7
9.1–15.6
Manufacturer’s reference intervals for nonpregnant
adults: TSH: 0.35–5.50 mIU/L, FT4: 11.5–22.7 pmol/L
TSH
0.06–3.67
TSH
0.03–4.51
0.05–4.50
FT4
11.8–21.0
10.6–17.6
TSH, thyrotrophin; FT4, free thyroxine
a
The referee intervals were calculated as 5th and 98th percentiles
b
The reference intervals were calculated as 5th and 95th percentiles
77
0.47–4.54
9.2–16.7
Thyroid autoimmunity suppresses thyroid function significantly as evident in our study in the TPO-Ab positive women during all three trimesters
of pregnancy. We found that TPO-Ab were positive in 12.5% of pregnant
women. The prevalence of TPO-Ab in the pregnant population is comparable to that found in the general female population with a similar age range
between 5–15 % (324). We looked at TSH ranges when TPO-Ab positive
patients were included into the data sample. Interestingly, women with positive TPO-Ab levels had significantly higher the 97.5 percentiles of TSH in
all three trimesters to 2.91, 2.82 and 2.52 mIU/L, respectively, when compared to those with TPO-Ab negativity. Thought there were no statistically
significant differences found in TSH between trimesters in TPO-Ab positive
pregnant women. Thus we excluded TPO-Ab positive women from the assessment of thyroid parameters reference range sample. Consequentely,
TSH values defining the selected upper centiles were lower (2.72, 2.51, 2.36
mIU/L, respectively) when TPO-Ab positive women had been removed
from the reference population. Our data is in agreement with the studies in
this concern (136-137, 323). TPO-Ab positive women might be at risk for
hypothyroidism, especially those with high-normal TSH concentrations,
when reference interval for non-pregnant population is used. Interesting data
has been published by Negro et al.(159) where thyroxine–treated women
with autoimmune thyroiditis maintained the euthyroid status, while in the
untreated group with TPO-Ab positivity FT4 decreased by 30% and TSH
levels increased progressively during gestation. Consequently, 19% of the
latter women became subclinically hypothyroid at the time of delivery.
Guidelines say that women with thyroid autoimmunity who are euthyroid in
the early stages of pregnancy are at risk of developing hypothyroidism and
should be monitored for elevation of TSH above the normal range and that
TPO-Ab is the most useful marker for the prediction of postpartum thyroid
dysfunction (1, 14). Overall we could conclude that the immune status of
the women influences thyroidal changes throughout the course of gestation
and a proper approach of evaluation is needed. The reference interval to rely
on carries a special concern on diagnosis and iniciation of thyroxine treatment in TPO-Ab positive euthyroid woman as it improves pregnancy outcomes (159). Moreover, the increased incidence of pregnancy loss in pregnant women with TSH levels between 2.5 and 5.0 mIU/L provides evidence
to support redefining the TSH upper limit of normal to 2.5 mIU/L in the first
trimester (164).
Serum FT4 concentrations also have a characteristic pattern during normal pregnancy. This pattern includes a slight and temporary rise in FT4
concentrations during the first trimester and a tendency towards progressive
decline in FT4 concentrations during later gestation (82) . This pattern was
78
observed in our study as well as other recent publications (323). This may
be associated with an increase in serum thyroid-binding globulin concentrations during pregnancy (325) and with iodine deficiency (174). In our FT4
results showed significant variation between trimesters with values decreasing from first to second trimester, but thereafter remaining, similar to those
reported by other studies. (26, 320, 326) Conversely, study in pregnant
women in the iodine-deficient area showed an absence of the usual FT4
spike (41). In our study FT4 was not influenced by antibody status, and this
was observed in the Switzerland study by Stricker et al. (135).
In addition, FT4 results in pregnancy are influenced by assay performance due to method-dependent artefacts (124) and vary among different
assay manufacturers (88, 133, 327), with the results falling in the lower part
of the non-pregnant reference interval or below the lower limit (123). Consequently, method specific reference interval is required for FT4 assays (77,
120).
In iodine-sufficient conditions, the physiologic FT4 decrement during the
second and third trimester does not exceed 10% (88), while in iodinedeficient nutritional conditions it reaches 20–25% (23). In line with this,
Laurberg et al. suggested that a moderate, 10–20% fall in the serum FT4
concentrations during pregnancy is not a sign of maternal dietary iodine deficiency (92). Our study indicates that a borderline 19% decrease in FT4
concentrations provides no clear answer regarding dietary iodine deficiency.
A study in Sweden, iodine-sufficient country, has shown the mean FT4 decrease by 15% from the first trimester to the second (134). Our earlier report
(328) on TSH concentrations taken on the third day after birth in a sample
of 177 newborns from the same cohort of pregnant women established a
2.8% prevalence of increased TSH concentrations above 5 mIU/L, which
did not exceed the prevalence rate under iodine-sufficient conditions, which
is usually below 3% (329-330), neither indicated dietary iodine deficiency
in this sample, nor did maternal TSH profiles in our study. In iodine deficient areas increases in TSH concentrations during late pregnancy have been
reported (26, 92).
Lithuania was considered a mild iodine deficient region (330) and severe
iodine deficiency was previously reported in pregnant women (32-33). Thus
there are counties within Lithuania, where iodine deficiency assessed by the
prevalence of goiter using different evaluation criteria in schoolchildren is
still moderate or severe (192). Data presented by Barzda et al. (331) show
newborn screening TSH over 5.1 mIU/L in 4.3–5.3% of cases during 2002–
2005, respectively. A slightly lower newborn TSH in our study might be
due to inclusion newborns with risk free for maternal thyroid disorders, assessing only maturely born newborns form exclusively one Lithuanian re79
gion. Our findings support the statement that iodide deficiency is not always
uniform across a nation (77). Studies in both Europe and the United States
suggest that iodide deficiency should be considered more as a "pocket disorder", meaning that it can be more prevalent in some areas of a country
compared with others (21, 191). In 2003 the governmental recommendations for the use of iodized salt were introduced in Lithuania and since 2005
are mandatory according to the Ministry of Health regulations. Sustained
salt iodization maintains an adequate iodine status in all population groups,
even in pregnant women despite their increased requirements (332).
Therefore, the consequences of iodization programs should be evaluated
precisely in respect to the region within the country as well as reporting reference interval for thyroid function should address this issue.
Our longitudinal cohort study examining the pattern of serum TSH concentrations and FT4 concentrations in healthy, TPO-Ab negative pregnant
women in three trimesters of pregnancy, have confirmed that during pregnancy thyroid axis hormone reference ranges differ from referral ranges
used in non–pregnant population.
Our study confirms successful iodinization in Lithuania. We had no
chance to measure iodine urine concentration, no data available on additional vitamin use during pregnancy and this is a limitation of the study as well
as relatively small sample-size. On the other hand, the longitudinal design is
a strength giving better indication of what occurs in thyroid function during
pregnancy and how reference ranges should be constructed. A study from a
mildly iodine-deficient area revealed that prolonged iodized salt significantly improves maternal thyroid economy and reduces the risk of maternal thyroid insufficiency during gestation (322). We support the need for gestational age specific reference interval when assessing thyroid function in pregnancy.
4.2. Iodine deficiency assessed by the newborn thyroid stimulating
hormone concentrations
We analyzed dry blood spot TSH data from the CH screening program in
newborns from Kaunas region to assess iodine deficiency. Four methods are
generally recommended for assessment of iodine nutrition in populations:
urinary iodine concentration (UI), the goiter rate, serum TSH, and TGB.
These indicators are complementary in that UI is a sensitive indicator of recent iodine intake (days) and Tg shows an intermediate response (weeks to
months), whereas changes in the goiter rate reflect long–term iodine nutrition (months to years)(3).
80
Generally, TSH can be used as an indicator of iodine nutrition because
serum TSH concentration is determined mainly by the level of circulating
thyroid hormone, which in turn reflects iodine intake. TSH is a sensitive indicator of iodine status in the newborn period (198, 318). The newborn thyroid contains less iodine but has higher rates of iodine turnover. Particularly,
when iodine supply is low, the maintenance of high iodine turnover requires
increased TSH stimulation. Serum TSH concentrations are therefore increased in iodine deficient infants for the first few weeks of life, a condition
termed transient newborn hypothyroidism (3). Therefore we used neonatal
TSH measures obtained three days after birth in our analysis.
According to the statement by WHO/UNICEF/ICCIDD, we evaluated
dry blood spot TSH measures, and found 2.8 percent of newborns being
above the 5 mIU/L. In the Table 1.1, a frequency of 3–19.9% indicates a
mild iodine deficiency (329). Our data showed that the assessed sample is at
the margin of iodine sufficiency, thus being a serious hallmark for
healthcare providers, assuring and maintaining the sufficient iodine intake
for women during pregnancy. The most recent NHANES survey (2003–
2004) reported that UI values are decreasing from 294 to 128 μg/L in women of childbearing age, with 37.2% of them having UI values below 100
μg/L, which suggests mild iodine deficiency (333).
It is known that iodine deficiency affects all stages of human life, however, pregnant women, lactating women, women of reproductive age, and
children younger than 3 years are considered to be at high risk (334). According to the data of 1995, Lithuania is in the low iodine deficiency area
(48, 330) with 22% of pregnant women in 2002 having a severe iodine deficiency (32). Therefore data on the neonatal thyroid screening appear to be
particularly interesting in the monitoring of iodine supply at a population
level. The data presented by Barzda et al. (207) demonstrated 4.3–5.3% of
cases of newborn screening TSH over 5.1 mIU/L during 2002–2005. A
slightly lower TSH in our study might be due to inclusion newborns with
risk free for maternal thyroid disorders, assessing only maturely born newborns form exclusively one Lithuanian region.
The study by Mickuviene et al. (192) assessed the prevalence of goiter in
school-age children (7–11 years) and found that the mean thyroid volume
exceeded 97th percentile in 72–82% (counted by M.B. Zimmermann (335)),
alerting severe iodine defficiency northeast of Lithuania. According to
WHO, a total number of children with goiter exeeding 30%, represents severe iodine defficiency in population (43). Studies in Lithuania are needed
to assess the relationship between the iodine status of schoolchildren and the
iodine status of pregnant women in the same location, as school-age children, the usual indicator group, are the most appropriate group to reflect the
81
iodine status of pregnant women (203), especially evaluating concequencies
of long run mandatory USI program in Lithuania. The national study on the
use of iodized salt in Lithuania was undertaken during August – October
2005 by the National Nutrition Center and the results indicated that 67.8%
of households were using iodized salt. An improvement over previous studies was seen, e.g. less than 10% of households used iodized salt in 1998,
which increased to 39% in 2002 (336). Iodine deficient countries especially,
should monitor the state of their iodine nutrition every three years and report
to the World Health Assembly on their progress (95).
The limitation of our study is that we cannot currently provide the data
on iodine in urine of pregnant women as well as their multivitamin pill use
during pregnancy. Nevertheless, we suppose, that women participating in
our study could have been self-motivated towards appropriate iodine use,
since they knew the aim of the study. We propose that the local situation
should be correctly evaluated before starting on medical recommendations
for adequate iodine supplementation programs during pregnancy. Finally,
healthcare providers should be cautious recommending certain brands of
multivitamins for pregnant women as it may not contain all the iodine they
claim. Multivitamins contain levels of iodine that are discordant by 50%
stated on their label (337). Moreover, there is a final general epidemiological concept that iodine deficiency requires constant monitoring, even after
the implementation of iodine supplementation in pregnant women (42, 338).
4.3. The newborn thyroid stimulating hormone levels in relation to
maternal age, gestation, birth weight and gender
As it was mentioned above, multiple factors can influence measurements
of TSH concentrations in newborns.We observed that older maternal age in
pregnancy and newborn gestational age were associated with elevated newborn bloodspot TSH levels on the third day of life. Therefore, a careful consideration of these factors should be drawn while assessing blood spot TSH
levels and providing antenatal care.
There is scanty research data available on the dynamics of the newborn
thyroid function during the prenatal period and the factors potentially influencing newborn TSH levels. Our data on the relation between newborn TSH
levels and maternal age is in close agreement with the study by Herbstman
et al. where older maternal age was independently associated with lower
umbilical cord total T4 level; nevertheless they did not show the same association with umbilical cord serum TSH levels in multivariate analysis (214).
We can only speculate on different study design used as well as different
82
geographical region and nutrition environment of the newborns and their
mothers studied. We can also hypothesize that cord blood TSH levels could
be influenced by the wide range of delivery factors.
It is noted that maternal age is increasing among pregnant Lithuanian
women. According to statistics of 2001 and 2008, the proportion of delivering women over 30 years of age was 30.9 and 37.7 percent, respectively
(339). In our study 31.1 percent of delivering women were after 30 years of
age. Older pregnant women have a higher risk of having a baby with a genetic abnormality, such as Down's syndrome, Edwards' syndrome or Patau's
syndrome (340). According to the worldwide database, The International
Clearinghouse for Birth Defects (341) and EUROCAT (342) collecting information on infants born with congenital malformations, and Italian study
from the Italian Registry for Congenital Hypothyroidism (343) show that
anomalies of the heart, nervous system, eyes (representing precocious structures in the developing embryo) and multiple congenital malformations are
significantly associated with CH (209, 344-345). These findings strongly
suggest a very early impairment in the first stages of embryo development
with a consequent involvement of different organs and structures. As the
fetus progresses into the third trimester, it develops the ability to produce its
own thyroid hormones but it is still dependent on maternal iodine for hormone synthesis (80, 238). While most women in Europe are classified as
iodine deficient during pregnancy (achieving only approximately half of the
recommended daily iodine intake), only 13–50% receive iodine supplementation (346). Therefore, we presume that maternal age and elevated neonatal
TSH levels acting jointly might have a significant impact on fetal intrauterine development and hormonal status of the newborn. There are known benefits of folic acid supplementation three months before and during early
stages of pregnancy in terms of preventing neural tube defects alone and reducing the incidence of other birth abnormalities such as congenital heart
disease, urinary tract problems, oral facial clefts, limb defects, and some
others (347-348). On the other hand, there are recommendations that women
should increase their daily iodine intake during pregnancy and breastfeeding
(1, 31, 190).
In our study we observed that gestational age was associated with increased bloodspot TSH levels in multivariate but not univariate models. In
agreement with our study, the relationship between gestational age and TSH
concentrations was shown by Korada et al. but multiple regression analysis
confirmed that this was a reflection of the close link between gestational age
and birth weight (215). On the contrary, Herbstman et al. concluded that
gestational age was independently associated with lower cord TSH, higher
cord total T4, and higher neonatal and subsequent bloodspot total T4 (214).
83
In the study by Miyamoto et al. the TSH levels varied widely and had no
correlation with gestational age because they were affected by the mode of
delivery (225). It is known, that as gestational age increases, the fetus increases the synthesis of both T4 and TSH (238). That statement was confirmed in the study by McElduff et al., where higher TSH values had been
associated with older gestational age (200). Studies of fetal and neonatal
thyroid function show that thyroid hormone levels rise as pregnancy advances (195, 349) with levels of TSH in cord blood and neonatal blood spot
samples positively related to gestational age (214).
In our study, the distribution of TSH was not significantly different between males and females, with males tended to have a higher median blood
spot TSH. Theoreticaly, estrogens and testosterone have the scanty direct
effects on TSH synthesis and secretion in humans (350). Nevertheless, similar observation on correlation between gender and bloodspot TSH was made
by Korada et al. (215). The studies by Herbstman et al. (214) and Chan et al.
(351) found the positive association between elevation of cord blood TSH
and male gender, but other researchers (195, 308) did not find significant
difference in TSH levels between males and females. Interestingly, a study
in Greece (352) assessed thyroid hormones in schoolchildren and found that
girls had lower TSH values than boys at puberty. The data on hypothyroidism and infertility presents (353) that hypothyroidism influences ovarian
function by decreasing levels of sex-hormone-binding globulin, thereby
increasing the number of bioavailable androgens (354). By this aproach, we
may hypothetically presume that possibly gender specific hormones have an
impact on the pituitary-thyroid axis and TSH regulation, therefore male
gender expressing higher TSH values.
Our data revealed that gestational age and maternal age were the strongest predictors of newborn TSH on the third day of life. We suppose health
care providers to be cautious providing antenatal care to the older woman in
terms of fetal and neonatal thyroid function, specially, when there is no consensus on universal screening for hypothyroidism in pregnancy (1). A case
finding approach is recommended (1) in women at high risk for thyroid dysfunction, but maternal age is not included in the criteria. Moreover, there is
a recent report on screening for CH and defining upper threshold limit for
newborn TSH (217), thus evaluating maternal age and neonatal TSH associations, we propose to be alert while interpreting newborns TSH during the
first days postpartum, born to older pregnant women.We suppose maternal
age factor could also be taken into account while deciding on iodine supplementation during pregnancy as well.
84
4.4. Delivery mode impact on newborn thyroid stimulating hormone
concentrations
We measured blood spot levels of TSH in newborns delivered by mothers who had no thyroid disorders, and did not find significant differences of
TSH concentration in newborns delivered vaginally, by vacuum extraction
or cesarean section. The same was concluded by other researchers (308,
318). Nevertheless, we have found diverse data on newborn thyroid funtion
effects and the delivery mode.
Few studies comfirmed that TSH levels were higher in newborns born by
cesarean section (199)(193-194). Interestingly, in the study by McElduff et
al, babies delivered by cesarean section were significantly more likely to
have TSH levels greater than 5 mIU/L on the third day of life than those delivered vaginally (200). Moreover, the incidence of false positive TSH tests
at screening (> or =15.0 mIU/L) was higher in newborns born by cesarean
section (351). With the rise in the rate of births by cesarean, this could be an
important factor in assessing population iodine deficiency using neonatal
TSH levels. One mechanism to explain this stimulatory effect on newborn
TSH is that topical iodine skin preparation for cesarean section deliveries
has an iodine load to the mother, part of which is transferred to the infant
resulting in acute inhibition of thyroid function (Wolff-Chaikoff effect). A
similar, but more marked elevation in neonatal TSH has been documented
with topical iodine antiseptic use on the newborn in some (311-314), but not
all reports (315-316).
In contrast, the results by other studies (190-192, 301) reported higher
cord blood TSH concentrations in infants born after normal vaginal delivery
than newborns born by caesarean section, although Miyamoto et al. (225)
reported that this did not persist to interfere with congenital hypothyroidism
screening. Thus, TSH levels tended to be higher in the vaginal delivery
group compared to the elective cesarean section group (355). Our data is in
agreement with the above researchers, by stating that mean serum TSH level
following normal vaginal delivery was higher than elective cesarean section
(but not significantly). Moreover, emergency cesarean section tended to
show higher newborn TSH levels than elective cesarean section. We can
only suppose that delivery stress was lowest in born by elective cesarean
section, thereby, presented newborn lower TSH could be stress related.
Moreover, similar parallel could be drawn between newborn TSH, Apgar
scores and delivery stress, discussed later on.
The mean cord serum TSH level in newborns delivered by vacuum extraction was significantly higher than the level following normal vaginal delivery (191, 319) or caesarean section (356). However, the mean TSH levels
85
of newborns on the third day in heel blood spotted filter paper had no significant differences among normal vaginal delivery, vacuum extraction and
caesarean section (356).
We also observed Apgar scores at 5 minutes effect on TSH. Infants with
Apgar of ≤8 at 5 minutes had higher mean levels of TSH as compared to
those with Apgar of 9–10 at 5 minutes, in consistent with the findings by
Herbstman (214). Additionally, it has been reported by other studies that the
Apgar score at 1 and 5 minutes is inversely associated with cord blood and
bloodspot TSH (197-198). Moreover, infants with asphyxia at birth (Apgar
score <4 at 5 min) had significantly higher cord blood TSH levels as compared to those without (228). Such findings rise the hypothesis that perinatal-delivery stress might have an impact on TSH elevation.
We reported for the first time dry blood spot TSH measures in association with some delivery data in the sample of newborns delivered by the
thyroid disease wise healthy Lithuanian women during pregnancy, that now
can be compared to the similarly designed studies. Although, the mode of
delivery have not had considerable influence on TSH in the newborns might
be due to a small sample size, but minor differences exist. We suggest that
the mode of delivery should be taken into consideration while interpreting
newborn blood spot TSH results.
4.5. Antenatal maternal mental state and anthropometric characteristics of newborns
Our present study demonstrates the strongest predictors alterating newborn anthropometric parameters in relation to certain psychological factors,
as well as maternal thyroid hormones throughout different time points in
pregnancy.
Firstly, we assessed maternal thyroid axis relation to newborn TSH. We
found that median newborn blood spot TSH concentrations were slightly
higher than the maternal values. As mentioned before, perinatal stress, environment temperature changes might have influenced the difference in values. It is noticed that throughout gestation, the serum TSH values are greater
in fetus than are present in maternal circulation and higher than would be
expected in adults with normal thyroid function (45). Moreover, we did not
find correlations between maternal thyroid axis hormones in all trimesters of
pregnancy. This finding suggests that the development and function of the
fetal thyroid depends on TSH stimulation from the fetal pituitary itself and
is unrelated to maternal pituitary stimulation. As our maternal thyroid axis
hormones were assessed relatively late in gestation, starting from 12th
86
week, there remains a question on maternal-fetal regulations early in gestation. However, in the sudy performed in marginaly low iodine defficiency
area, mean newborn TSH level was found to be significantly higher than
maternal values, but newborn TSH levels increased in parallel and were
highly correlated with maternal data, suggesting a regulatory link between
both thyroid economies (357). Presence of thyroid antibodies in euthyroid
women is associated with misscariage (157), thus we looked at associations
of TPO-Ab and newborn thyroid. We found no evidence that elevated TPOAb would be associated with newborn TSH concentrations, in a way confirming the fetal immune tolerance to maternal factors (286).
Secondly, we analysed maternal antropometric measurements in relation
to newborn anthropometry. Our study found a positive relation between maternal weight, height, BMI and newborn birthweight and height. A positive
relationship between maternal BMI and the birth weight of the off-spring
was also found in the other studies (358-360). As it was expected, gestational age was strongly associated with newborns birthweight, height and BMI.
Pregestational maternal body size indices and weight gain during pregnancy
have repeatedly been shown to be independent determinants of the size of
the offspring (253-254). We found that maternal pre-pregnancy weight has
the positive effect on newborn birthweight in multiple regression analysis.
Studies that reported pre-pregnancy weight and height found a significant
association with either low birth weight (less than 2500 g) or the birthweight
(361-363). This asociation is broadly adressed in the contries with socioeconomic deprivation (68). Poor maternal weight status is a risk factor for
growth restriction and low weight births and adverse pregnancy outcomes
(364-365). On the other hand, maternal body weight gain during pregnancy
is associated with increased birth weight of the offspring (366), greater incidence of pregnancy complications (367-368), the greater weight gain, the
greater risks (369). We also analyzed maternal weight gain during pregnancy and found it to be a strong positive predictor of newborn height. Having
in mind that maternal prenatal obesity in developed countries has increased
significantly over the past 15 years with maternal body weight at the first
prenatal visit increased by 20% (370-371), attention should be drawn to the
consequencies of the latter. Moreover, several recent publications have
demonstrated that newborn and infant body weight and BMI are important
factors predicting cardiovascular morbidity, stroke and diabetes in adults
(372-375). Recent gestational weight gain recommendations are based on a
woman's pre-pregnancy BMI (376). Entering pregnancy with a normal BMI
and gaining within the recommended gestational weight gain ranges minimizes maternal, fetal and newborn risks. Thus, maternal pre-pregnancy
87
weight, weight gain should be an important family planing issue and counsel of healthcare specialist on proper nutrition during pregnancy.
In our study higher FT4 concentration at second trimester of pregnancy
predicted lower birthweight and lower BMI of the newborn. Multiple retrospective studies have reported an association of poorly controlled hyperthyroidism with intrauterine growth restriction or low birth weight compared
with treated euthyroid women (20, 377-378). More specifically, hyperthyroidism in the third trimester was an independent risk factor for low birth
weight (379). Similar findings were observed in the first trimester, were hypothyroxinemia was associated with preterm labor and macrosomia (380).
Interestingly, studies in adults suggest that low normal FT4 is associated
with higher BMI (381) and obesity (382), as well as overt hypothyroidism in
adults is associated with weight gain, while hyperthyroidism is associated
with weight loss (383).
Moreover, we found in the multiple regression analysis that FT4 concentration in the third trimester of pregnancy was the strong negative predictor
of birth weight and together with other significant maternal psychological
factors covered 31% of variance. The study by other researchers, assessing
UI found that newborns had lower mean birthweight with UI below 50 μg/L
in the third trimester of pregnancy (384), but they did not find association
between FT4 and TSH measured during the first trimester (384).
Moreover, thyroid hormone changes during pregnancy were noticed to
have an impact on psychological factors (60, 248). We found 9.8% women
in the first, 4.6% in the second and 6.9% women in the third trimester of
pregnancy with depressive symptoms, which is in agreement with a recent
review of the literature (385). Recently published ACOG opinion reflects
the importance of evaluation of depressive symptoms in pregnancy. Although the organization noted that currently, there is insufficient evidence to
support a firm recommendation for antepartum or postpartum screening,
evaluating patients for, diagnosing, and treating depression, it has the potential to benefit a woman and her family and should be strongly considered
(62). As a result of our research, we determined that 11.6% of women expierenced depressive symptoms at least in one assessement throughout three
trimesters of pregnancy. Leaving an open quest for discussion on the usefulness of screening for depression symptoms antenataly, more so as the
EDS is easy to fill-in and not time consuming instrument, giving important
information on the pschychological state of the childbearing women.
We looked at maternal depression as the possible predictor of newborn
anthropometry, since often undetected and uncontrolled maternal depression
in pregnancy puts the developing fetus at harm due to consumption of alcoholic beverages and smoking during pregnancy (386-387), poor prenatal
88
care (388) and suicide attempts (389), including behavioral problems later in
childhood (277). Furthermore, depression occurrence during pregnancy poses further risks to women (390) as it is associated with obstetric complications, such as miscarriage, premature delivery, premature rupture of membranes, preeclampsia, postpartum depression (263, 391-393) and newborn
birthweight and body mass index alternations (64, 269, 394-396).
We observed that higher EPDS score in the first trimester of pregnancy
was a strong predictor together with other cofounders of higher newborn
weight at birth and BMI. In contrast, a recent study in the developing country (Pakistan) shows that depression in the third trimester of pregnancy predicts low birth weight (394). Whereas, Andersson et al. (397) in their Swedish and Berle et al. (398) in their Norwegian large population-based studies
on maternal antenatal depressive disorders and/or antenatal anxiety disorders did not find any differences in newborn birthweight. Similarly, Larsson
et al. did not find associations between antenatal depression low birthweight
(399).
Contradictions between the findings in the studies can be explained by
methodological differences, where assessment of depression and anxiety
was made in different trimesters of pregnancy by different self-assessment
questionnaires and even for the same scales different cut-off points were
applied. Furthermore, contrasting findings in the studies could be explained
by cultural differences and coping with depression under certain socioeconomical conditions which predispose certain behaviors of women, which
may lead to adverse pregnancy outcomes.
It is known that some emotional, psychological responses, such as depression, anger, anxiety might be mediated by stress. In our study we looked
at acute and chronic stress impact on newborn anthropometry, as stress has
profoundly harmful effects on reproduction, particularly during gestation,
and is causally associated with pregnancy failure (400) and adverse development of offspring health (401-402), including craniofacial malformations
and heart defects (403).
Stress increases hormone secretion from the euroendocrine HPA axis.
Psychosocial stress has been shown to be associated with elevated maternal
cortisol levels during pregnancy (404-405), thus there are several possible
mechanisms how signals of maternal stress may reach the fetus. Firstly, by
reduction in blood flow to the uterus and fetus at increased levels of maternal stress (281). Secondly, by transplacental transport of maternal hormones (406). Thirdly, by stress-induced release of placental corticotrophinreleasing hormone to the intrauterine environment (407). All of the mentioned factors restrict the delivery of oxygen and nutrient to the fetus, subsequently, affecting fetal growth and development (408).
89
We analysed acute and chronic stress exposure impact on anthropometrical measures during different gestational time periods and found that
chronic stress in the second trimester of pregnancy was positively associated
with birthweight. Interestingly, when we conducted multivariate regression
together with FT4 and other factors, we found that both chronic stress and
FT4 in the third trimester of pregnancy predicted lower birthweight of the
newborn. Although, maternal chronic stress in the second and third trimester
of pregnancy has a divergent impact on newborn weight at birth, we suppose, it could be partially explained by the mentioned above possible mechanisms how signals of maternal stress may reach the fetus. The time window of the influence of maternal stress induced cortisol secretion on fetal
growth is however, unknown. While it is suggested that early gestation may
be a particular sensitive period for maternal, placental, fetal pathophysiology (408-409), late pregnancy is a critical period as it is known for the accelerated fetal somatic growth (410). Only a few studies focus on the timing
effects of life events on birth outcomes (411-414). However, when the
women are exposured to chronic stress, they fail to show an up-regulation of
placental enzyme activity converting cortisol to the inactive form, cortisone,
indicating that chronic stress may be detrimental for healthy pregnancy
(401, 415). In addition, Hobel et al. have reported that maternal stress at 18–
20 weeks of gestation predicted a rise in corticotropin-releasing hormone
levels at 28–30 weeks of gestation (416). Our findings show that chronic
stress at 22–26 weeks of gestation positively effects fetal growth, but later
on, in pregnancy at 32–36 weeks of gestation has an opposite action. Summarizing all above, we could hypothesize that our findings support the stress
related data on maternal placental fetal pathophysiology on the clinical level, predicting newborns weight.
Moreover, our results show chronic stress impact on the newborn anthropometry that could be compared with the studies on cortisol and neonatal
outcomes. Previous studies observed an association between maternal cortisol levels and fetal growth (417), estimated fetal weight (418-419) or
birthweight (410, 418). Thus, a recent study in Netherland did not observe a
mediation effect of maternal cortisol on the association between maternal
psychosocial problems and offspring birthweight (420). In the other studies
psychosocial stress (421) and adverse life events (422) were not risk factors
for low birthweight newborns. Although Newton et al. (423) reported a significant association between life events and low birthweight, they did not
control for confounding variables.
Our study revealed an impact of acute stress in the second trimester of
pregnancy on the birthweight of the newborn. Interestingly, we noticed that
chronic and acute stress in the second trimester of pregnancy had a positive
90
effect on birthweight, whereas chronic stress in the third thrimestre has a
negative effect on newborn birthweight. Other studies showed that exposure
to acute stress in the first trimestre (424), but not in the second and third
trimesters, had a greater negative effect on the birthweight of newborn (414,
425).
We suppose that the most vulnerable period for the effects of maternal
chronic stress and thyroid hormone actions appears to be in the third trimester, when the fetal growth spurt occurs. Nevertheless, attention should
be drawn to the assessment of exposure to chronic stress during early and
late pregnancy, especially knowing that it precipitates long-term adverse
consequences on offspring (e.g. cardiovascular disease, depression) (285).
The degree of stress response depends also on genetic factors, personality
characteristics, previous experience, support from the social environment,
and the way of coping with stress (265). This applies to pregnant women as
well (265). We evaluated five maternal personality traits and found that personality dimension was not associated with both perceived acute or chronic
stress. Though, we observed that conscientiousness was negatively related
to depression and anxiety symptomology during pregnancy. Similarly to
others, conscientiousness was inversely related to major depressive disorder,
but different from us, demonstrated a positive relationship with generalized
anxiety disorder (426). Moreover, in our study neuroticism was strongly related to anxiety and moderately to depression. Extraversion was inversely
associated with anxiety during pregnancy. The etiological trait approach assumes that personality is an independent risk factor for disease. This means
that various early biological characteristics of the individual are related to
both personality and health (427).
Therefore, we evaluated maternal personality dimensions impact on the
newborn anthropometrical measurements. We found that only one, namely,
conscientiousness, was revealed regardless of positive effect on newborn
birthweight in the second pregnancy trimester. This significant association
persisted after adjusting for maternal age in multivariable analysis. Hereby,
we suppose, that maternal conscientiousness, reflecting dependability, such
as being careful, thorough, responsible, organised and planful, could potentiate a certain behavioral pattern during pregnancy that favors newborn anthropometrical measures.
In summary, our study demonstrates that maternal anthropometrical
measurements, psychological factors and thyroid function acting jointly are
associated with birth outcome, namely, anthropometrical measurements of
the newborns. The protective effect of personality trait - conscientiousness,
was observed, as well as the negative effect of the perceived chronic psychosocial stress and elevated free thyroxine in the third trimester of preg91
nancy, regardless of the birth weight. Therefore, combining different areas,
such as maternal mental health, nutrition, hormonal balance in pregnant
women brings relevant information on the predictors of newborn anthropometrical measures. Health care supervisors should pay attention to woman’s
nutritional status before pregnancy, as it is a strong determinant of newborn
outcomes. We propose that interventions to prevent or reduce stress, diagnosis of anxiety, depression symptoms or dissorder should be started before
conception and should be observed and maintained carefully throughout the
pregnancy.
92
CONCLUSIONS
1. Recommended reference intervals for TSH concentrations were
found to be 0.02–2.72 mIU/L for the first trimester, 0.22–2.51
mIU/L for the second trimester and 0.28–2.36 mIU/L for the third
trimester of pregnancy. Recommended reference intervals for FT4
concentrations were found to be 13.2–23.1 pmol/L for the first trimester, 11.8–18.5 pmol/L for the second trimester and 10.5–18.3
pmol/L for the third trimester of pregnancy. Thyroid autoimmunity
assessed by thyroid–peroxidase antibody concentrations increases
maternal TSH concentration and have no effect on FT4 during all
trimesters of pregnancy.
2. Screening of the iodine deficiency using indirect measure, dry blood
spot thyroid stimulating hormone concentrations in newborns, with
2.8 percent newborns being above the 5 mIU/L, showed iodine sufficiency at the implementation of the universal salt iodisation program in Kaunas, Lithuania. A 19% decrease from peak to nadir in
FT4 concentrations during pregnancy confirms sufficient dietary iodine intake in pregnant women.
3. We have found that older maternal age at delivery and longer gestation is associated with elevated newborn bloodspot TSH levels, but
the mode of delivery has no considerable influence. The third day after birth newborn TSH concentrations failed to show association
with maternal thyroid function and autoimunity.
4. The newborn birth weight and BMI is negatively influenced by
higher maternal thyroxine concentration in the second, perceived
chronic psychosocial stress in the third trimester of pregnancy,
whereas maternal personality trait, conscientiousness, symptoms of
antenatal maternal depression in the first and perceived chronic psychosocial stress in the second trimester have positive effect.
93
SCIENTIFIC SIGNIFICANCE OF THE STUDY
New information of scientific value on psychoendocrine challenge in
pregnancy is contained in this study. We have reported for the first time
changes in thyroid status and presented the trimester-specific reference intervals for thyroid stimulating hormone and free thyroxine in the sample of
healthy Lithuanian women during pregnancy that now can be compared to
the similarly designed studies at the time of gestation and different geographical endpoints.
The longitudinal design of the study provides evidence that maternal
emotional state and thyroid function, as a pshychoendocrine disruptor,
found to be associated with birth outcomes of newborn. The results suggest
an association between maternal psychosocial stress, personality traits, free
thyroxine and newborn anthropometrical measurements. Therefore, combining different areas, such as maternal mental health, nutrition, thyroid hormonal balace in pregnant women brings relevant information on the predictors of newborn anthropometrical measures.
94
PRACTICAL RECOMMENDATIONS
We suggest using trimester-specific reference intervals for thyroid axis
function assessement in pregnancy. Reference intervals for TSH concentrations were found to be 0.02–2.72 mIU/L for the first trimester, 0.22–2.51
mIU/L for the second trimester and 0.28–2.36 mIU/L for the third trimester
of pregnancy. Reference intervals for FT4 concentrations were found to be
13.2–23.1 pmol/L for the first trimester, 11.8–18.5 pmol/L for the second
trimester and 10.5–18.3 pmol/L for the third trimester of pregnancy. We
cannot provide evidence in favor of screening for thyroid dysfunction in
pregnancy, but may advocate research projects concerning this issue.
Thyroid screening of the newborns showed iodine sufficiency using indirect method of blood spot TSH measures, with 2.8 percent newborns being
above the 5 mIU/L. We suppose that the degree of iodine deficiency should
be assessed in each concerned area specifically, and the local situation correctly evaluated before starting on medical recommendations for adequate
iodine supplementation during pregnancy.
Maternal age, newborns gestational age and delivery mode factors should
be carefully considered while interpreting newborn’s blood spot TSH levels.
Health care supervisors should pay attention to woman’s nutritional and
thyroid function status throughout pregnancy, as the determinants of newborn outcomes. We propose that interventions to prevent or reduce stress,
diagnosis of depression symptoms and anxiety should be started before conception and should be observed and maintained carefully throughout the
pregnancy.
95
ACKNOWLEDGEMENTS
I am grateful to everyone who contributed to this thesis and who helped
me in the process of accomplishing it.
I am deeply thankful to my supervisor Assoc. Prof. Dr. Eimantas Svedas
for his constant support, encouragement and advice. Thank you, Eimantas,
for teaching me about research, for beeing constant inspiration, a source of
knowledge and experience, and for welcoming and supporting me right
from the start. Thank you for trusting in me during this research project.
I am grateful to Dr. Habil. Robertas Bunevicius from the Institute of Psychophysiology and Rehabilitation, Lithuanian University of Health Sciences
and Prof. Dr. Victor J. M. Pop from Tilburg University, the Netherlands, the
initiators of this research, for giving the opportunity and inviting me to participate as an investigator in this multidisciplinary study. I especially thank
my consultant Robertas Bunevicius for the help, innovative ideas, advice
and valuable discussions regarding the project, articles and thesis preparation. Prof. Dr. Victor J. M. Pop and the staff at the Laboratory in Tilburg
University have provided the support and equipment I needed to produce
and complete my thesis. Your help was greatly appreciated.
I would not have been able to finish my thesis without the continuous
help and support from Scientist Nijole Raskauskiene at the Institute of Psychophysiology and Rehabilitation, Lithuanian University of Health Sciences. With my deepest respect I thank you for the tremendous help, for staying
with me and encouraging me in every step during the research until the final
stages of writing this thesis. Thank you for each idea and comment delivered with a smile.
I woud like to thank Prof. Dr. Ruta Nadisauskiene for making me feel
welcome in the Obstetric and Gynaecology department from the very first
day and keeping me straight on the right path, showing me how to deal with
every situation in a constructive way.
I am extremely thankful to psychiatrist Dr. Laima Kusminskas for the
key role and overwhelming input into the psychiatric investigation of this
research. I would not have been able to finish this thesis without your contribution. I am grateful for your fruitful collaboration during the research,
for advice and disscussions regarding the thesis. Thank you for beeing a
good friend.
I am indebted to the neonatologist Assoc. Prof. Dr. Egle Markuniene and
psychologists Vitalija Marmiene and Laima Miliukiene for their gratuitous
work in this reasearch project.
96
I thank my other co-authors for their collaboration and help during research, for good advice, critical attitude and valuable comments during the
writing process. Thank you to Dr. Narseta Mickuviene, Adomas Bunevicius,
Dr. Lina Barsiene, Egle Savukyne, Egle Cesnaite.
Thank you to Dr. Egle Barcaite, Dr. Daiva Simanaviciute for constructive comments on writing the manuscript, always being ready to help with
various ideas and for being such good friends.
I am grateful to Prof. Dr. Reynir T. Geirsson for my first and unforgettable lesson in getting started on my research path „on how to write an article“. Thank you for the given opportunity, help and encouragement.
I would like to thank Assoc. Prof. Dr. Ingrida Uloziene and the staff of
the Department of Research Affairs for the help and advice on my study
plan from the early stages till the last minutes of my project. Thank you for
making me feel welcome from the first day of my PhD studies.
I am grateful to Assoc. Prof. Adomas Drazdauskas, Violeta Use, Rita
Kliopmaniene for English and Lithuanian language revision of the manuscript.
I am grateful to Ruta Gruode for helping me in variuos issues while publishing this thesis.
I am thankful to all the doctors, administrators, residents and nurses at
the Obstetrics and Gynaecology department at Lithuanian University of
Health Sciences. I am fortunate to have found such supporting colleagues in
the clinic.
Thank you to Janina Didziuliene and Silainiai primary care staff for beeing helpful and understanding, making the reasearch go smooth in their clinic. It was trully a joy working with colleagues at P. Mažylis Maternity Hospital, Kaunas Christian Maternity Hospital and Kaunas 2nd Clinical Hospital.
Thank you to Prof. Dr. Habil. Vaidutis Kucinskas and the personnel at
The Centre for Medical Genetics of Vilnius University Hospital for poviding me the opportunity to use the data from National Neonatal Screening
Program Registry.
All the pregnant women who participated in the study are deeply thanked
for their broad attitude towards medical research.
In my daily work I have been blessed with a friendly and cheerful group
of fellow colleagues. Thank you.
My family and my friends have been very supporting and understanding
throughout these past five years. My parents Elena and Antanas, sister Iveta,
grandmother Elena, I love you.
Thank you all for your help. You have given me more help and support
than you know.
97
REFERENCE LIST
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
Abalovich M, Amino N, Barbour LA, Cobin RH, De Groot LJ, Glinoer D, et
al. Management of thyroid dysfunction during pregnancy and postpartum: an
Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2007
Aug;92(8 Suppl):S1-47.
Glinoer D, Spencer CA. Serum TSH determinations in pregnancy: how, when
and why? Nat Rev Endocrinol. 2010 Sep;6(9):526-9.
Chapter 20. The Iodine Deficiency Disorders Endocrine education Inc, South
Dartmouth, MA 02748 2009; Available from: www.thyroidmanager.org.
Field T, Diego M, Hernandez-Reif M, Figueiredo B, Deeds O, Ascencio A, et
al. Comorbid depression and anxiety effects on pregnancy and neonatal
outcome. Infant Behav Dev. 2010 Feb;33(1):23-9.
Groome LJ, Swiber MJ, Bentz LS, Holland SB, Atterbury JL. Maternal
anxiety during pregnancy: effect on fetal behavior at 38 to 40 weeks of
gestation. J Dev Behav Pediatr. 1995 Dec;16(6):391-6.
Bunevicius R, Kusminskas L, Bunevicius A, Nadisauskiene RJ, Jureniene K,
Pop VJ. Psychosocial risk factors for depression during pregnancy. Acta
Obstet Gynecol Scand. 2009;88(5):599-605.
Stagnaro-Green A. Can a high-risk case-finding approach identify all women
with thyroid dysfunction during pregnancy? Nat Clin Pract Endocrinol
Metab. 2007 Mar;3(3):216-7.
Glinoer D. Thyroid hyperfunction during pregnancy. Thyroid. 1998 Sep;8(9):
859-64.
Mandel SJ, Cooper DS. The use of antithyroid drugs in pregnancy and
lactation. J Clin Endocrinol Metab. 2001 Jun;86(6):2354-9.
Krassas GE, Poppe K, Glinoer D. Thyroid function and human reproductive
health. Endocr Rev. 2010 Oct;31(5):702-55.
Abalovich M, Gutierrez S, Alcaraz G, Maccallini G, Garcia A, Levalle O.
Overt and subclinical hypothyroidism complicating pregnancy. Thyroid. 2002
Jan;12(1):63-8.
Allan WC, Haddow JE, Palomaki GE, Williams JR, Mitchell ML, Hermos
RJ, et al. Maternal thyroid deficiency and pregnancy complications:
implications for population screening. J Med Screen. 2000;7(3):127-30.
Glinoer D. The systematic screening and management of hypothyroidism and
hyperthyroidism during pregnancy. Trends Endocrinol Metab. 1998
Dec;9(10):403-11.
Klein RZ, Haddow JE, Faix JD, Brown RS, Hermos RJ, Pulkkinen A, et al.
Prevalence of thyroid deficiency in pregnant women. Clin Endocrinol (Oxf).
1991 Jul;35(1):41-6.
Haddow JE, Palomaki GE, Allan WC, Williams JR, Knight GJ, Gagnon J, et
al. Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. N Engl J Med. 1999 Aug 19;
341(8):549-55.
98
16. Casey BM, Dashe JS, Wells CE, McIntire DD, Byrd W, Leveno KJ, et al.
Subclinical hypothyroidism and pregnancy outcomes. Obstet Gynecol. 2005
Feb;105(2):239-45.
17. Wikner BN, Sparre LS, Stiller CO, Kallen B, Asker C. Maternal use of
thyroid hormones in pregnancy and neonatal outcome. Acta Obstet Gynecol
Scand. 2008;87(6):617-27.
18. Hollowell JG, LaFranchi S, Smallridge RC, Spong CY, Haddow JE, Boyle
CA. 2004 where do we go from here?--Summary of working group discussions on thyroid function and gestational outcomes. Thyroid. 2005 Jan;15(1):
72-6.
19. Matalon S, Sheiner E, Levy A, Mazor M, Wiznitzer A. Relationship of
treated maternal hypothyroidism and perinatal outcome. J Reprod Med. 2006
Jan;51(1):59-63.
20. Mannisto T, Vaarasmaki M, Pouta A, Hartikainen AL, Ruokonen A, Surcel
HM, et al. Perinatal outcome of children born to mothers with thyroid
dysfunction or antibodies: a prospective population-based cohort study. J Clin
Endocrinol Metab. 2009 Mar;94(3):772-9.
21. Glinoer D. Pregnancy and iodine. Thyroid. 2001 May;11(5):471-81.
22. Monteleone P, Parrini D, Faviana P, Carletti E, Casarosa E, Uccelli A, et al.
Female Infertility Related to Thyroid Autoimmunity: The Ovarian Follicle
Hypothesis. Am J Reprod Immunol. 2011 Jan 18.
23. Glinoer D. The regulation of thyroid function in pregnancy: pathways of
endocrine adaptation from physiology to pathology. Endocr Rev. 1997
Jun;18(3):404-33.
24. Casey BM, Dashe JS, Wells CE, McIntire DD, Leveno KJ, Cunningham FG.
Subclinical hyperthyroidism and pregnancy outcomes. Obstet Gynecol. 2006
Feb;107(2 Pt 1):337-41.
25. Glinoer D. Thyroid regulation and dysfunction in pregnant patient. 2008;
Available from: www.thyroidmanager.org.
26. Marwaha RK, Chopra S, Gopalakrishnan S, Sharma B, Kanwar RS, Sastry A,
et al. Establishment of reference range for thyroid hormones in normal
pregnant Indian women. BJOG. 2008 Apr;115(5):602-6.
27. Gyamfi C, Wapner RJ, D'Alton ME. Thyroid dysfunction in pregnancy: the
basic science and clinical evidence surrounding the controversy in management. Obstet Gynecol. 2009 Mar;113(3):702-7.
28. Kooistra L, Crawford S, van Baar AL, Brouwers EP, Pop VJ. Neonatal
effects of maternal hypothyroxinemia during early pregnancy. Pediatrics.
2006 Jan;117(1):161-7.
29. Pop VJ, Brouwers EP, Vader HL, Vulsma T, van Baar AL, de Vijlder JJ.
Maternal hypothyroxinaemia during early pregnancy and subsequent child
development: a 3-year follow-up study. Clin Endocrinol (Oxf). 2003 Sep;
59(3):282-8.
99
30. Morreale de Escobar G, Obregon MJ, Escobar del Rey F. Is neuropsychological development related to maternal hypothyroidism or to maternal
hypothyroxinemia? J Clin Endocrinol Metab. 2000 Nov;85(11):3975-87.
31. Report of a WHO Technical Consultation on prevention and control of iodine
defficiency in pregnancy, lactation, and in children less than 2 years of age
(Geneva, 24-26 January 2005). Public Health Nutr (Special Issue). 2007(10
(12A)):1527-611.
32. Bėrontienė R. Vaikų skydliaukės struktūriniai ir funkciniai pokyčiai jodo
trūkumo sąlygomis. Daktaro disertacija: Kauno Medicinos Universitetas;
2002.
33. Berontiene R, Sidlauskas V, Jusciene D, Bourdoux P. Iodine investigation in
Lithuania: the data of TTH > 5mIU/L in newborns, schoolchildren thyroid
and urinary iodine concentration. Lietuvos endokrinologija. 2001(9):197-202.
34. Lazarus JH, Premawardhana LD. Screening for thyroid disease in pregnancy.
J Clin Pathol. 2005 May;58(5):449-52.
35. Brent GA. Maternal thyroid function: interpretation of thyroid function tests
in pregnancy. Clin Obstet Gynecol. 1997 Mar;40(1):3-15.
36. ACOG practice bulletin. Thyroid disease in pregnancy. Number 37, August
2002. American College of Obstetrics and Gynecology. Int J Gynaecol
Obstet. 2002 Nov;79(2):171-80.
37. Gong Y, Hoffman BR. Free thyroxine reference interval in each trimester of
pregnancy determined with the Roche Modular E-170 electrochemiluminescent immunoassay. Clin Biochem. 2008 Jul;41(10-11):902-6.
38. Springer D, Zima T, Limanova Z. Reference intervals in evaluation of
maternal thyroid function during the first trimester of pregnancy. Eur J
Endocrinol. 2009 May;160(5):791-7.
39. Price A, Weetman AP. Thyroid function tests. Thyroid stimulating hormone
outside the normal range has important implications. BMJ. 2000 Oct 28;
321(7268):1080; author reply 1-2.
40. Yu B, Wang QW, Huang RP, Cao F, Zhu ZQ, Sun DC, et al. Establishment
of self-sequential longitudinal reference intervals of maternal thyroid function
during pregnancy. Exp Biol Med (Maywood). 2010 Oct 1;235(10):1212-5.
41. Costeira MJ, Oliveira P, Ares S, Roque S, de Escobar GM, Palha JA.
Parameters of thyroid function throughout and after pregnancy in an iodinedeficient population. Thyroid. 2010 Sep;20(9):995-1001.
42. Andersson M, de Benoist B, Darnton-Hill I, DeLange F. Iodine deficiency in
Europe. A continuing public health problem: WHO2007.
43. WHO, UNICEF, ICCIDD. Assessment of iodine deficiency disorders and
monitoring their elimination: A guide for programme managers: Geneva,
World Health Organization (WHO/NHD/01.1).2001.
44. Iodine status worldwide. WHO Global Database on Iodine Deficiency
[database on the Internet]. Geneva, World Health Organization. 2004.
Available from: http://www.who.int.
100
45. Kronenberg HM, Melmed S, Polonsky SK, Larsen PR, editors. Williams
Textbook of Endocrinology. 11th ed. Philadelphia: Saunders; 2008.
46. Hollowell JG, Staehling NW, Hannon WH, Flanders DW, Gunter EW,
Maberly GF, et al. Iodine nutrition in the United States. Trends and public
health implications: iodine excretion data from National Health and Nutrition
Examination Surveys I and III (1971-1974 and 1988-1994). J Clin Endocrinol
Metab. 1998 Oct;83(10):3401-8.
47. Hollowell JG, Haddow JE. The prevalence of iodine deficiency in women of
reproductive age in the United States of America. Public Health Nutr. 2007
Dec;10(12A):1532-9; discussion 40-1.
48. Petrauskaitė A, Bartkevičiūtė R, Imbrasienė A. Išskiriamo jodo koncentracijos nustatymas tiriant Lietuvos moksleivių sveikatos būklę. Medicina.
1995(31):714-6.
49. Vitti P, Rago T, Aghini-Lombardi F, Pinchera A. Iodine deficiency disorders
in Europe. Public Health Nutr. 2001 Apr;4(2B):529-35.
50. Dėl Lietuvos Respublikos Apsaugos Ministro 2003 m. liepos 1 d. įsakymo
Nr. V-392 „DĖL LIETUVOS HIGIENOS NORMOS HN 15:2003 „Maisto
higiena“ Tvirtinimo pakeitimo V-255 (April 22, 2004 ).
51. Delange F. Screening for congenital hypothyroidism used as an indicator of
the degree of iodine deficiency and of its control. Thyroid. 1998 Dec;
8(12):1185-92.
52. Joffe RT. Hormone treatment of depression. Dialogues Clin Neurosci. 2011;
13(1):127-38.
53. Bauer M, Goetz T, Glenn T, Whybrow PC. The thyroid-brain interaction in
thyroid disorders and mood disorders. J Neuroendocrinol. 2008 Oct;20(10):
1101-14.
54. Bunevicius R. Thyroid disorders in mental patients. Curr Opin Psychiatry.
2009 Jul;22(4):391-5.
55. Bunevicius A, Peceliuniene J, Mickuviene N, Valius L, Bunevicius R.
Screening for depression and anxiety disorders in primary care patients.
Depress Anxiety. 2007;24(7):455-60.
56. Carta MG, Loviselli A, Hardoy MC, Massa S, Cadeddu M, Sardu C, et al.
The link between thyroid autoimmunity (antithyroid peroxidase
autoantibodies) with anxiety and mood disorders in the community: a field of
interest for public health in the future. BMC Psychiatry. 2004;4:25.
57. Fountoulakis KN, Iacovides A, Grammaticos P, St Kaprinis G, Bech P.
Thyroid function in clinical subtypes of major depression: an exploratory
study. BMC Psychiatry. 2004 Mar 15;4:6.
58. Kuijpens JL, Vader HL, Drexhage HA, Wiersinga WM, van Son MJ, Pop VJ.
Thyroid peroxidase antibodies during gestation are a marker for subsequent
depression postpartum. Eur J Endocrinol. 2001 Nov;145(5):579-84.
59. Pedersen CA, Johnson JL, Silva S, Bunevicius R, Meltzer-Brody S, Hamer
RM, et al. Antenatal thyroid correlates of postpartum depression. Psychoneuroendocrinology. 2007 Apr;32(3):235-45.
101
60. Pop VJ, Wijnen HA, Lapkienne L, Bunivicius R, Vader HL, Essed GG. The
relation between gestational thyroid parameters and depression: a reflection
of the downregulation of the immune system during pregnancy? Thyroid.
2006 May;16(5):485-92.
61. Austin MP, Priest SR, Sullivan EA. Antenatal psychosocial assessment for
reducing perinatal mental health morbidity. Cochrane Database Syst Rev.
2008(4):CD005124.
62. Committee opinion no. 453: Screening for depression during and after
pregnancy. Obstet Gynecol. 2010 Feb;115(2 Pt 1):394-5.
63. Gjerdingen DK, Yawn BP. Postpartum depression screening: importance,
methods, barriers, and recommendations for practice. J Am Board Fam Med.
2007 May-Jun;20(3):280-8.
64. Dayan J, Creveuil C, Herlicoviez M, Herbel C, Baranger E, Savoye C, et al.
Role of anxiety and depression in the onset of spontaneous preterm labor. Am
J Epidemiol. 2002 Feb 15;155(4):293-301.
65. Barker DJ. The intrauterine environment and adult cardiovascular disease.
Ciba Found Symp. 1991;156:3-10; discussion -6.
66. Lucas A. Programming by early nutrition in man. Ciba Found Symp.
1991;156:38-50; discussion -5.
67. Hales CN, Barker DJ. Type 2 (non-insulin-dependent) diabetes mellitus: the
thrifty phenotype hypothesis. Diabetologia. 1992 Jul;35(7):595-601.
68. Wardlaw T, Blanc A, Zupan J, Åhman E. Low birthweight: country, regional
and global estimates. Geneva, Switzeland: UNICEF and WGO2004.
69. Pearce MS, Unwin NC, Relton CL, Alberti KG, Parker L. Lifecourse
determinants of fasting and post-challenge glucose at age 50 years: the
Newcastle Thousand Families Study. Eur J Epidemiol. 2005;20(11):915-23.
70. Obesity and overweight. Fact sheet N°311: WHO2011.
71. Normal birthweight is critical to future health and development: Childinfo/UNICEF2009.
72. Hassan M. Consideration on some hormone binding proteins patterns during
pregnancy. Horm Metab Res. 1991(23):85-7.
73. Sapin R, Schlienger JL. [Thyroxine (T4) and tri-iodothyronine (T3) determinations: techniques and value in the assessment of thyroid function]. Ann
Biol Clin (Paris). 2003 Jul-Aug;61(4):411-20.
74. Larsen PR, Silva JE, Kaplan MM. Relationships between circulating and
intracellular thyroid hormones: physiological and clinical implications.
Endocr Rev. 1981 Winter;2(1):87-102.
75. Roti E, Fang SL, Green K, Emerson CH, Braverman LE. Human placenta is
an active site of thyroxine and 3,3'5-triiodothyronine tyrosyl ring deiodination. J Clin Endocrinol Metab. 1981 Sep;53(3):498-501.
76. Spencer CA, LoPresti JS, Patel A, Guttler RB, Eigen A, Shen D, et al.
Applications of a new chemiluminometric thyrotropin assay to subnormal
measurement. J Clin Endocrinol Metab. 1990 Feb;70(2):453-60.
102
77. Demers LM, Spencer CA. Laboratory medicine practice guidelines: laboratory support for the diagnosis and monitoring of thyroid disease. Clin
Endocrinol (Oxf). 2003 Feb;58(2):138-40.
78. Glinoer D, de Nayer P, Bourdoux P, Lemone M, Robyn C, van Steirteghem
A, et al. Regulation of maternal thyroid during pregnancy. J Clin Endocrinol
Metab. 1990 Aug;71(2):276-87.
79. Glinoer D, De Nayer P, Robyn C, Lejeune B, Kinthaert J, Meuris S. Serum
levels of intact human chorionic gonadotropin (HCG) and its free alpha and
beta subunits, in relation to maternal thyroid stimulation during normal
pregnancy. J Endocrinol Invest. 1993 Dec;16(11):881-8.
80. Burrow GN. Thyroid function and hyperfunction during gestation. Endocr
Rev. 1993 Apr;14(2):194-202.
81. Panesar NS, Li CY, Rogers MS. Reference intervals for thyroid hormones in
pregnant Chinese women. Ann Clin Biochem. 2001 Jul;38(Pt 4):329-32.
82. Kurioka H, Takahashi K, Miyazaki K. Maternal thyroid function during
pregnancy and puerperal period. Endocr J. 2005 Oct;52(5):587-91.
83. Soldin OP. Thyroid function testing in pregnancy and thyroid disease:
trimester-specific reference intervals. Ther Drug Monit. 2006 Feb;28(1):8-11.
84. Glinoer D. Increased TBG during pregnancy and increased hormonal
requirements. Thyroid. 2004 Jun;14(6):479-80; author reply 80-1.
85. Smallridge RC, Glinoer D, Hollowell JG, Brent G. Thyroid function inside
and outside of pregnancy: what do we know and what don't we know?
Thyroid. 2005 Jan;15(1):54-9.
86. Bartalena L. Recent achievements in studies on thyroid hormone-binding
proteins. Endocr Rev. 1990 Feb;11(1):47-64.
87. Glinoer D, Delange F, Laboureur I, de Nayer P, Lejeune B, Kinthaert J, et al.
Maternal and neonatal thyroid function at birth in an area of marginally low
iodine intake. J Clin Endocrinol Metab. 1992 Sep;75(3):800-5.
88. Kahric-Janicic N, Soldin SJ, Soldin OP, West T, Gu J, Jonklaas J. Tandem
mass spectrometry improves the accuracy of free thyroxine measurements
during pregnancy. Thyroid. 2007 Apr;17(4):303-11.
89. Glinoer D. The regulation of thyroid function during normal pregnancy:
importance of the iodine nutrition status. Best Pract Res Clin Endocrinol
Metab. 2004 Jun;18(2):133-52.
90. Glinoer D. The importance of iodine nutrition during pregnancy. Public
Health Nutr. 2007 Dec;10(12A):1542-6.
91. Glinoer D. Feto-maternal repercussions of iodine deficiency during
pregnancy. An update. Ann Endocrinol (Paris). 2003 Feb;64(1):37-44.
92. Laurberg P, Nohr SB, Pedersen KM, Hreidarsson AB, Andersen S, Bulow
Pedersen I, et al. Thyroid disorders in mild iodine deficiency. Thyroid. 2000
Nov;10(11):951-63.
93. Kung AW, Lao TT, Chau MT, Tam SC, Low LC. Goitrogenesis during
pregnancy and neonatal hypothyroxinaemia in a borderline iodine sufficient
area. Clin Endocrinol (Oxf). 2000 Dec;53(6):725-31.
103
94. Sack J, Goldstein A, Charpak N, Rozin A, Ruiz-Pelaez JG, Figueroa de
Calume Z, et al. Postpartum maternal hyperthyrotropinemia in an area in
which iodine supplementation is required. Thyroid. 2003 Oct;13(10):959-64.
95. WHO. WHA58.24: Sustaining the elimination of iodine deficiency disorders.
2005; Available from:http://apps.who.int/gb/ebwha/pdf_files/WHA58/WHA
58_24-en.pdf.
96. Marco A, Vicente A, Castro E, Perez CE, Rodríguez O, Merchan MA, et al.
Patterns of Iodine Intake and Urinary Iodine Concentrations During
Pregnancy and Blood Thyroid-Stimulating Hormone Concentrations in the
Newborn Progeny. Thyroid. [doi: 10.1089/thy.2010.0046]. 2010:null-null.
97. Ladenson PW, Singer PA, Ain KB, Bagchi N, Bigos ST, Levy EG, et al.
American Thyroid Association guidelines for detection of thyroid dysfunction. Arch Intern Med. 2000 Jun 12;160(11):1573-5.
98. Laboratory assessment of thyroid function [database on the Internet]2010
Available from: http://www.uptodate.com/contents/laboratory-assessment-ofthyroid-function?source=search_result&selectedTitle=13~150.
99. Hollowell JG, Staehling NW, Flanders WD, Hannon WH, Gunter EW,
Spencer CA, et al. Serum TSH, T(4), and thyroid antibodies in the United
States population (1988 to 1994): National Health and Nutrition Examination
Survey (NHANES III). J Clin Endocrinol Metab. 2002 Feb;87(2):489-99.
100. Boucai L, Hollowell JG, Surks MI. An approach for development of age-,
gender-, and ethnicity-specific thyrotropin reference limits. Thyroid. 2011
Jan;21(1):5-11.
101. Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History,
Physical, and Laboratory Examinations. 3rd edition ed. Boston1990.
102. Caldwell G, Kellett HA, Gow SM, Beckett GJ, Sweeting VM, Seth J, et al. A
new strategy for thyroid function testing. Lancet. 1985 May 18;1(8438):11179.
103. Nicoloff JT, Spencer CA. Clinical review 12: The use and misuse of the
sensitive thyrotropin assays. J Clin Endocrinol Metab. 1990 Sep;71(3):553-8.
104. Ross DS, Ardisson LJ, Meskell MJ. Measurement of thyrotropin in clinical
and subclinical hyperthyroidism using a new chemiluminescent assay. J Clin
Endocrinol Metab. 1989 Sep;69(3):684-8.
105. Spencer CA, Takeuchi M, Kazarosyan M. Current status and performance
goals for serum thyroglobulin assays. Clin Chem. 1996 Jan;42(1):164-73.
106. Surks MI, Goswami G, Daniels GH. The thyrotropin reference range should
remain unchanged. J Clin Endocrinol Metab. 2005 Sep;90(9):5489-96.
107. National Academy of Clinical Biochemistry. NACB laboratory medicine
practice
guidelines [database on the Internet]. Available from: www.nacb.org/lmpg/
main.stm.
108. Andersen S, Pedersen KM, Bruun NH, Laurberg P. Narrow individual
variations in serum T(4) and T(3) in normal subjects: a clue to the
104
109.
110.
111.
112.
113.
114.
115.
116.
117.
118.
119.
120.
121.
understanding of subclinical thyroid disease. J Clin Endocrinol Metab. 2002
Mar;87(3):1068-72.
Browning MC, Ford RP, Callaghan SJ, Fraser CG. Intra- and interindividual
biological variation of five analytes used in assessing thyroid function:
implications for necessary standards of performance and the interpretation of
results. Clin Chem. 1986 Jun;32(6):962-6.
Beck-Peccoz P, Amr S, Menezes-Ferreira MM, Faglia G, Weintraub BD.
Decreased receptor binding of biologically inactive thyrotropin in central
hypothyroidism. Effect of treatment with thyrotropin-releasing hormone. N
Engl J Med. 1985 Apr 25;312(17):1085-90.
Xie J, Pannain S, Pohlenz J, Weiss RE, Moltz K, Morlot M, et al. Resistance
to thyrotropin (TSH) in three families is not associated with mutations in the
TSH receptor or TSH. J Clin Endocrinol Metab. 1997 Dec;82(12):3933-40.
Alberti L, Proverbio MC, Costagliola S, Romoli R, Boldrighini B, Vigone
MC, et al. Germline mutations of TSH receptor gene as cause of nonautoimmune subclinical hypothyroidism. J Clin Endocrinol Metab. 2002 Jun;
87(6):2549-55.
Tonacchera M, Perri A, De Marco G, Agretti P, Banco ME, Di Cosmo C, et
al. Low prevalence of thyrotropin receptor mutations in a large series of
subjects with sporadic and familial nonautoimmune subclinical hypothyroidism. J Clin Endocrinol Metab. 2004 Nov;89(11):5787-93.
Brennan MD, Klee GG, Preissner CM, Hay ID. Heterophilic serum
antibodies: a cause for falsely elevated serum thyrotropin levels. Mayo Clin
Proc. 1987 Oct;62(10):894-8.
Wood JM, Gordon DL, Rudinger AN, Brooks MM. Artifactual elevation of
thyroid-stimulating hormone. Am J Med. 1991 Feb;90(2):261-2.
Ward G, McKinnon L, Badrick T, Hickman PE. Heterophilic antibodies
remain a problem for the immunoassay laboratory. Am J Clin Pathol. 1997
Oct;108(4):417-21.
Howanitz PJ, Howanitz JH, Lamberson HV, Ennis KM. Incidence and
mechanism of spurious increase in serum thyrotropin. Clin Chem. 1982
Mar;28(3):427-31.
Zweig MH, Csako G, Benson CC, Weintraub BD, Kahn BB. Interference by
anti-immunoglobulin G antibodies in immunoradiometric assays of thyrotropin involving mouse monoclonal antibodies. Clin Chem. 1987 Jun;33(6):
840-4.
Midgley JE. Direct and indirect free thyroxine assay methods: theory and
practice. Clin Chem. 2001 Aug;47(8):1353-63.
Baloch Z, Carayon P, Conte-Devolx B, Demers LM, Feldt-Rasmussen U,
Henry JF, et al. Laboratory medicine practice guidelines. Laboratory support
for the diagnosis and monitoring of thyroid disease. Thyroid. 2003
Jan;13(1):3-126.
Stockigt JR. Free thyroid hormone measurement. A critical appraisal.
Endocrinol Metab Clin North Am. 2001 Jun;30(2):265-89.
105
122. Forzy G, d'Herbomez M, Gasser F, Massart C, Beaudonnet A, Sapin R.
[Proposed reference values for nine methods for measurement of free
thyroxin]. Ann Biol Clin (Paris). 2004 May-Jun;62(3):325-9.
123. Sapin R, D'Herbomez M, Schlienger JL. Free thyroxine measured with
equilibrium dialysis and nine immunoassays decreases in late pregnancy. Clin
Lab. 2004;50(9-10):581-4.
124. d'Herbomez M, Forzy G, Gasser F, Massart C, Beaudonnet A, Sapin R.
Clinical evaluation of nine free thyroxine assays: persistent problems in
particular populations. Clin Chem Lab Med. 2003 Jul;41(7):942-7.
125. Nelson JC, Weiss RM, Wilcox RB. Underestimates of serum free thyroxine
(T4) concentrations by free T4 immunoassays. J Clin Endocrinol Metab. 1994
Jul;79(1):76-9.
126. Lee RH, Spencer CA, Mestman JH, Miller EA, Petrovic I, Braverman LE, et
al. Free T4 immunoassays are flawed during pregnancy. Am J Obstet
Gynecol. 2009 Mar;200(3):260 e1-6.
127. Waise A, Price HC. The upper limit of the reference range for thyroidstimulating hormone should not be confused with a cut-off to define
subclinical hypothyroidism. Ann Clin Biochem. 2009 Mar;46(Pt 2):93-8.
128. Kratzsch J, Fiedler GM, Leichtle A, Brugel M, Buchbinder S, Otto L, et al.
New reference intervals for thyrotropin and thyroid hormones based on
National Academy of Clinical Biochemistry criteria and regular
ultrasonography of the thyroid. Clin Chem. 2005 Aug;51(8):1480-6.
129. Vanderpump MP, Tunbridge WM, French JM, Appleton D, Bates D, Clark F,
et al. The incidence of thyroid disorders in the community: a twenty-year
follow-up of the Whickham Survey. Clin Endocrinol (Oxf). 1995
Jul;43(1):55-68.
130. Surks MI, Ortiz E, Daniels GH, Sawin CT, Col NF, Cobin RH, et al.
Subclinical thyroid disease: scientific review and guidelines for diagnosis and
management. JAMA. 2004 Jan 14;291(2):228-38.
131. Mandel SJ, Spencer CA, Hollowell JG. Are detection and treatment of
thyroid insufficiency in pregnancy feasible? Thyroid. 2005 Jan;15(1):44-53.
132. Cooper DS. Subclinical thyroid disease: consensus or conundrum? Clin
Endocrinol (Oxf). 2004 Apr;60(4):410-2.
133. Soldin OP, Hilakivi-Clarke L, Weiderpass E, Soldin SJ. Trimester-specific
reference intervals for thyroxine and triiodothyronine in pregnancy in iodinesufficient women using isotope dilution tandem mass spectrometry and
immunoassays. Clin Chim Acta. 2004 Nov;349(1-2):181-9.
134. Soldin OP, Tractenberg RE, Hollowell JG, Jonklaas J, Janicic N, Soldin SJ.
Trimester-specific changes in maternal thyroid hormone, thyrotropin, and
thyroglobulin concentrations during gestation: trends and associations across
trimesters in iodine sufficiency. Thyroid. 2004 Dec;14(12):1084-90.
135. Stricker R, Echenard M, Eberhart R, Chevailler MC, Perez V, Quinn FA.
Evaluation of maternal thyroid function during pregnancy: the importance of
106
136.
137.
138.
139.
140.
141.
142.
143.
144.
145.
146.
147.
148.
using gestational age-specific reference intervals. Eur J Endocrinol. 2007
Oct;157(4):509-14.
Haddow JE, Knight GJ, Palomaki GE, McClain MR, Pulkkinen AJ. The
reference range and within-person variability of thyroid stimulating hormone
during the first and second trimesters of pregnancy. J Med Screen.
2004;11(4):170-4.
Yan YQ, Dong ZL, Dong L, Wang FR, Yang XM, Jin XY, et al. Trimesterand method-specific reference intervals for thyroid tests in pregnant Chinese
women: methodology, euthyroid definition and iodine status can influence the
setting of reference intervals. Clin Endocrinol (Oxf). 2011 Feb;74(2):262-9.
Moreno-Reyes R, Carpentier YA, Macours P, Gulbis B, Corvilain B, Glinoer
D, et al. Seasons but not ethnicity influence urinary iodine concentrations in
Belgian adults. Eur J Nutr. 2010 Oct 20.
Dashe JS, Casey BM, Wells CE, McIntire DD, Byrd EW, Leveno KJ, et al.
Thyroid-stimulating hormone in singleton and twin pregnancy: importance of
gestational age-specific reference ranges. Obstet Gynecol. 2005 Oct;106(4):
753-7.
Pearce EN, Oken E, Gillman MW, Lee SL, Magnani B, Platek D, et al.
Association of first-trimester thyroid function test values with thyroperoxidase antibody status, smoking, and multivitamin use. Endocr Pract. 2008
Jan-Feb;14(1):33-9.
Galofre JC, Davies TF. Autoimmune thyroid disease in pregnancy: a review.
J Womens Health (Larchmt). 2009 Nov;18(11):1847-56.
Jurczynska J, Zieleniewski W. [Clinical implications of occurrence of
antithyroid antibodies in pregnant women and in the postpartum period].
Przegl Lek. 2004;61(8):864-7.
Sinclair D. Clinical and laboratory aspects of thyroid autoantibodies. Ann
Clin Biochem. 2006 May;43(Pt 3):173-83.
Blazer S, Moreh-Waterman Y, Miller-Lotan R, Tamir A, Hochberg Z. Maternal hypothyroidism may affect fetal growth and neonatal thyroid function.
Obstet Gynecol. 2003 Aug;102(2):232-41.
Glinoer D, Soto MF, Bourdoux P, Lejeune B, Delange F, Lemone M, et al.
Pregnancy in patients with mild thyroid abnormalities: maternal and neonatal
repercussions. J Clin Endocrinol Metab. 1991 Aug;73(2):421-7.
Premawardhana LD, Parkes AB, John R, Harris B, Lazarus JH. Thyroid
peroxidase antibodies in early pregnancy: utility for prediction of postpartum
thyroid dysfunction and implications for screening. Thyroid. 2004 Aug;14(8):
610-5.
Bonds DE, Freedberg KA. Cost-effectiveness of prenatal screening for
postpartum thyroiditis. J Womens Health Gend Based Med. 2001 Sep;10(7):
649-58.
Muller AF, Drexhage HA, Berghout A. Postpartum thyroiditis and autoimmune thyroiditis in women of childbearing age: recent insights and
107
149.
150.
151.
152.
153.
154.
155.
156.
157.
158.
159.
160.
161.
consequences for antenatal and postnatal care. Endocr Rev. 2001 Oct;
22(5):605-30.
Laurberg P, Andersen S, Bjarnadottir RI, Carle A, Hreidarsson A, Knudsen
N, et al. Evaluating iodine deficiency in pregnant women and young infantscomplex physiology with a risk of misinterpretation. Public Health Nutr.
2007 Dec;10(12A):1547-52; discussion 53.
Fukayama H, Nasu M, Murakami S, Sugawara M. Examination of antithyroid
effects of smoking products in cultured thyroid follicles: only thiocyanate is a
potent antithyroid agent. Acta Endocrinol (Copenh). 1992 Dec;127(6):520-5.
Ashoor G, Maiz N, Rotas M, Jawdat F, Nicolaides KH. Maternal thyroid
function at 11 to 13 weeks of gestation and subsequent fetal death. Thyroid.
2010 Sep;20(9):989-93.
Haddow JE, Cleary-Goldman J, McClain MR, Palomaki GE, Neveux LM,
Lambert-Messerlian G, et al. Thyroperoxidase and thyroglobulin antibodies
in early pregnancy and preterm delivery. Obstet Gynecol. 2010 Jul;116(1):5862.
Mannisto T, Vaarasmaki M, Suvanto E. Pregnancy outcomes in women with
thyroid peroxidase antibodies. Obstet Gynecol. 2011 Jan;117(1):174-5; author
reply 5-6.
Poppe K, Glinoer D. Thyroid autoimmunity and hypothyroidism before and
during pregnancy. Hum Reprod Update. 2003 Mar-Apr;9(2):149-61.
Poppe K, Glinoer D, Van Steirteghem A, Tournaye H, Devroey P,
Schiettecatte J, et al. Thyroid dysfunction and autoimmunity in infertile
women. Thyroid. 2002 Nov;12(11):997-1001.
Toulis KA, Goulis DG, Venetis CA, Kolibianakis EM, Negro R, Tarlatzis
BC, et al. Risk of spontaneous miscarriage in euthyroid women with thyroid
autoimmunity undergoing IVF: a meta-analysis. Eur J Endocrinol. 2010
Apr;162(4):643-52.
Stagnaro-Green A, Glinoer D. Thyroid autoimmunity and the risk of
miscarriage. Best Pract Res Clin Endocrinol Metab. 2004 Jun;18(2):167-81.
Negro R, Mangieri T, Coppola L, Presicce G, Casavola EC, Gismondi R, et
al. Levothyroxine treatment in thyroid peroxidase antibody-positive women
undergoing assisted reproduction technologies: a prospective study. Hum
Reprod. 2005 Jun;20(6):1529-33.
Negro R, Formoso G, Mangieri T, Pezzarossa A, Dazzi D, Hassan H.
Levothyroxine treatment in euthyroid pregnant women with autoimmune
thyroid disease: effects on obstetrical complications. J Clin Endocrinol
Metab. 2006 Jul;91(7):2587-91.
Mannisto T, Vaarasmaki M, Pouta A, Hartikainen AL, Ruokonen A, Surcel
HM, et al. Thyroid dysfunction and autoantibodies during pregnancy as
predictive factors of pregnancy complications and maternal morbidity in later
life. J Clin Endocrinol Metab. 2010 Mar;95(3):1084-94.
Gartner R. Thyroid diseases in pregnancy. Curr Opin Obstet Gynecol. 2009
Dec;21(6):501-7.
108
162. Pop VJ, Maartens LH, Leusink G, van Son MJ, Knottnerus AA, Ward AM, et
al. Are autoimmune thyroid dysfunction and depression related? J Clin
Endocrinol Metab. 1998 Sep;83(9):3194-7.
163. Bergink V, Kushner SA, Pop V, Kuijpens H, Lambregtse-van den Berg MP,
Drexhage RC, et al. Prevalence of autoimmune thyroid dysfunction in
postpartum psychosis. Br J Psychiatry. 2011 Feb 22.
164. Negro R, Schwartz A, Gismondi R, Tinelli A, Mangieri T, Stagnaro-Green A.
Increased pregnancy loss rate in thyroid antibody negative women with TSH
levels between 2.5 and 5.0 in the first trimester of pregnancy. J Clin
Endocrinol Metab. 2010 Sep;95(9):E44-8.
165. Poppe K, Glinoer D, Tournaye H, Devroey P, Schiettecatte J, Haentjens P, et
al. Thyroid autoimmunity and female infertility. Verh K Acad Geneeskd
Belg. 2006;68(5-6):357-77.
166. ACOG Practice Bulletin. Clinical management guidelines for obstetriciangynecologists. Number 37, August 2002. (Replaces Practice Bulletin Number
32, November 2001). Thyroid disease in pregnancy. Obstet Gynecol. 2002
Aug;100(2):387-96.
167. Screening for thyroid disease: recommendation statement. Ann Intern Med.
2004 Jan 20;140(2):125-7.
168. Baskin HJ, Cobin RH, Duick DS, Gharib H, Guttler RB, Kaplan MM, et al.
American Association of Clinical Endocrinologists medical guidelines for
clinical practice for the evaluation and treatment of hyperthyroidism and
hypothyroidism. Endocr Pract. 2002 Nov-Dec;8(6):457-69.
169. Gharib H, Tuttle RM, Baskin HJ, Fish LH, Singer PA, McDermott MT.
Consensus Statement #1: Subclinical thyroid dysfunction: a joint statement on
management from the American Association of Clinical Endocrinologists, the
American Thyroid Association, and The Endocrine Society. Thyroid. 2005
Jan;15(1):24-8; response 32-3.
170. Brent GA. Diagnosing thyroid dysfunction in pregnant women: Is case
finding enough? J Clin Endocrinol Metab. 2007 Jan;92(1):39-41.
171. Vaidya B, Anthony S, Bilous M, Shields B, Drury J, Hutchison S, et al.
Detection of thyroid dysfunction in early pregnancy: Universal screening or
targeted high-risk case finding? J Clin Endocrinol Metab. 2007 Jan;92(1):
203-7.
172. Keeling JW, Khong TY, editors. Fetal and neonatal pathology. 4th edition ed.
London: Springer-Verlang; 2007.
173. Contempre B, Jauniaux E, Calvo R, Jurkovic D, Campbell S, de Escobar GM.
Detection of thyroid hormones in human embryonic cavities during the first
trimester of pregnancy. J Clin Endocrinol Metab. 1993 Dec;77(6):1719-22.
174. Morreale de Escobar G, Obregon MJ, Escobar del Rey F. Role of thyroid
hormone during early brain development. Eur J Endocrinol. 2004 Nov;151
Suppl 3:U25-37.
175. Utiger RD. Maternal hypothyroidism and fetal development. N Engl J Med.
1999 Aug 19;341(8):601-2.
109
176. Bianco AC, Salvatore D, Gereben B, Berry MJ, Larsen PR. Biochemistry,
cellular and molecular biology, and physiological roles of the iodothyronine
selenodeiodinases. Endocr Rev. 2002 Feb;23(1):38-89.
177. de Jesus LA, Carvalho SD, Ribeiro MO, Schneider M, Kim SW, Harney JW,
et al. The type 2 iodothyronine deiodinase is essential for adaptive thermogenesis in brown adipose tissue. J Clin Invest. 2001 Nov;108(9):1379-85.
178. Glinoer D. Potential repercussions for the progeny of maternal
hypothyroxinemia during pregnancy. Thyroid. 2000 Jan;10(1):59-62.
179. Ohara N, Tsujino T, Maruo T. The role of thyroid hormone in trophoblast
function, early pregnancy maintenance, and fetal neurodevelopment. J Obstet
Gynaecol Can. 2004 Nov;26(11):982-90.
180. Laurberg P, Bulow Pedersen I, Pedersen KM, Vestergaard H. Low incidence
rate of overt hypothyroidism compared with hyperthyroidism in an area with
moderately low iodine intake. Thyroid. 1999 Jan;9(1):33-8.
181. Nohr SB, Laurberg P. Opposite variations in maternal and neonatal thyroid
function induced by iodine supplementation during pregnancy. J Clin
Endocrinol Metab. 2000 Feb;85(2):623-7.
182. Dunn JT. Endemic goiter and cretinism: an update on iodine status. J Pediatr
Endocrinol Metab. 2001;14 Suppl 6:1469-73.
183. Delange F, de Benoist B, Pretell E, Dunn JT. Iodine deficiency in the world:
where do we stand at the turn of the century? Thyroid. 2001 May;11(5):43747.
184. Auso E, Lavado-Autric R, Cuevas E, Del Rey FE, Morreale De Escobar G,
Berbel P. A moderate and transient deficiency of maternal thyroid function at
the beginning of fetal neocorticogenesis alters neuronal migration.
Endocrinology. 2004 Sep;145(9):4037-47.
185. Bunevicius R, Prange AJ, Jr. Thyroid disease and mental disorders: cause and
effect or only comorbidity? Curr Opin Psychiatry. 2010 Jul;23(4):363-8.
186. Melse-Boonstra A, Jaiswal N. Iodine deficiency in pregnancy, infancy and
childhood and its consequences for brain development. Best Pract Res Clin
Endocrinol Metab. 2010 Feb;24(1):29-38.
187. Berbel P, Navarro D, Auso E, Varea E, Rodriguez AE, Ballesta JJ, et al. Role
of late maternal thyroid hormones in cerebral cortex development: an experimental model for human prematurity. Cereb Cortex. 2010 Jun;20(6):146275.
188. Zoeller RT, Rovet J. Timing of thyroid hormone action in the developing
brain: clinical observations and experimental findings. J Neuroendocrinol.
2004 Oct;16(10):809-18.
189. Kempers MJ, van der Sluijs Veer L, Nijhuis-van der Sanden RW, Lanting CI,
Kooistra L, Wiedijk BM, et al. Neonatal screening for congenital hypothyroidism in the Netherlands: cognitive and motor outcome at 10 years of
age. J Clin Endocrinol Metab. 2007 Mar;92(3):919-24.
190. WHO/ICCIDD/UNICEF. Assessment of the iodine deficiency disorders and
monitoring their elimination. Geneva: World Health Organization,2007.
110
191. Nohr SB, Laurberg P, Borlum KG, Pedersen KM, Johannesen PL, Damm P,
et al. Iodine deficiency in pregnancy in Denmark. Regional variations and
frequency of individual iodine supplementation. Acta Obstet Gynecol Scand.
1993 Jul;72(5):350-3.
192. Mickuvienė N, Krasauskienė A, Kazanavičius G. [The results of thyroid
ultrasound examination in randomly selected schoolchildren]. Medicina
(Kaunas). 2006;42(9):751-8.
193. de Luis DA, Aller R, Izaola O. [Iodine deficiency during pregnancy ]. An
Med Interna. 2005 Sep;22(9):445-8.
194. Waller DK, Anderson JL, Lorey F, Cunningham GC. Risk factors for
congenital hypothyroidism: an investigation of infant's birth weight, ethnicity,
and gender in California, 1990-1998. Teratology. 2000 Jul;62(1):36-41.
195. LaFranchi S. Congenital hypothyroidism: etiologies, diagnosis, and management. Thyroid. 1999 Jul;9(7):735-40.
196. Dėl visuotinio naujagimių tikrinimo dėl įgimtų medžiagų apykaitos ligų
tvarkos aprašo patvirtinimo, V-865 (2004 12 06).
197. Indicators for Assessing Iodine Deficiency Disorders and Their Control
through Salt Iodization. World Health Organization, United Nations Children’s Fund: International Council for Control of Iodine Deficiency Disorders, WHO NUT/94 Geneva, World Health Organization; 1994. p. 1-55.
198. Zimmermann MB, Aeberli I, Torresani T, Burgi H. Increasing the iodine
concentration in the Swiss iodized salt program markedly improved iodine
status in pregnant women and children: a 5-y prospective national study. Am
J Clin Nutr. 2005 Aug;82(2):388-92.
199. Fagela-Domingo C, Padilla CD. Newborn screening for congenital hypothyroidism in early discharged infants. Southeast Asian J Trop Med Public
Health. 2003;34 Suppl 3:165-9.
200. McElduff A, McElduff P, Wiley V, Wilcken B. Neonatal thyrotropin as
measured in a congenital hypothyroidism screening program: influence of the
mode of delivery. J Clin Endocrinol Metab. 2005 Dec;90(12):6361-3.
201. Mikelsaar RV, Viikmaa M. Neonatal thyroid-stimulating hormone screening
as an indirect method for the assessment of iodine deficiency in Estonia.
Horm Res. 1999;52(6):284-6.
202. Travers CA, Guttikonda K, Norton CA, Lewis PR, Mollart LJ, Wiley V, et al.
Iodine status in pregnant women and their newborns: are our babies at risk of
iodine deficiency? Med J Aust. 2006 Jun 19;184(12):617-20.
203. Andersson M, de Benoist B, Delange F, Zupan J. Prevention and control of
iodine deficiency in pregnant and lactating women and in children less than
2-years-old: conclusions and recommendations of the Technical Consultation.
Public Health Nutr. 2007 Dec;10(12A):1606-11.
204. Becker DV, Braverman LE, Delange F, Dunn JT, Franklyn JA, Hollowell JG,
et al. Iodine supplementation for pregnancy and lactation-United States and
Canada: recommendations of the American Thyroid Association. Thyroid.
2006 Oct;16(10):949-51.
111
205. Glinoer D, De Nayer P, Delange F, Lemone M, Toppet V, Spehl M, et al. A
randomized trial for the treatment of mild iodine deficiency during pregnancy: maternal and neonatal effects. J Clin Endocrinol Metab. 1995
Jan;80(1):258-69.
206. Glinoer D. Maternal and fetal impact of chronic iodine deficiency. Clin
Obstet Gynecol. 1997 Mar;40(1):102-16.
207. Barzda A, Kučinskas V, Kazanavičius G, Krasauskienė A, Bartkevičiūtė R.
Jodo trūkumas: problema ir sprendimo būdai. Lietuvos sveikata. 2005 2005
11 17-23.
208. Delange F. Neonatal thyroid screening as a monitoring tool for the control of
iodine deficiency. Acta Paediatr Suppl. 1999 Dec;88(432):21-4.
209. Reddy PA, Rajagopal G, Harinarayan CV, Vanaja V, Rajasekhar D, Suresh
V, et al. High prevalence of associated birth defects in congenital
hypothyroidism. Int J Pediatr Endocrinol. 2010;2010:940980.
210. Cassio A, Tatò L, Colli C, Spolettini E, Costantini E, Cacciari E. Incidence of
congenital malformations in congenital hypothyroiidsm. Screening.
1994(3):125-30.
211. Boivin J, Bunting L, Collins JA, Nygren KG. International estimates of
infertility prevalence and treatment-seeking: potential need and demand for
infertility medical care. Hum Reprod. 2007 Jun;22(6):1506-12.
212. Boivin J, Rice F, Hay D, Harold G, Lewis A, van den Bree MM, et al.
Associations between maternal older age, family environment and parent and
child wellbeing in families using assisted reproductive techniques to
conceive. Soc Sci Med. 2009 Jun;68(11):1948-55.
213. Copeland DL, Sullivan KM, Houston R, May W, Mendoza I, Salamatullah Q,
et al. Comparison of neonatal thyroid-stimulating hormone levels and
indicators of iodine deficiency in school children. Public Health Nutr. 2002
Feb;5(1):81-7.
214. Herbstman J, Apelberg BJ, Witter FR, Panny S, Goldman LR. Maternal,
infant, and delivery factors associated with neonatal thyroid hormone status.
Thyroid. 2008 Jan;18(1):67-76.
215. Korada M, Pearce MS, Avis E, Turner S, Cheetham T. TSH levels in relation
to gestation, birth weight and sex. Horm Res. 2009;72(2):120-3.
216. Lao TT, Panesar NS. Neonatal thyrotrophin and mode of delivery. Br J Obstet
Gynaecol. 1989 Oct;96(10):1224-7.
217. Korada SM, Pearce M, Ward Platt MP, Avis E, Turner S, Wastell H, et al.
Difficulties in selecting an appropriate neonatal thyroid stimulating hormone
(TSH) screening threshold. Arch Dis Child. 2010 Mar;95(3):169-73.
218. Chan LY, Chiu PY, Lau TK. Cord blood thyroid-stimulating hormone level
in high-risk pregnancies. Eur J Obstet Gynecol Reprod Biol. 2003 Jun 10;
108(2):142-5.
219. Cha LYS, Lau TK, Chiu PY, Wing-KinWong G, Leung TN. Levels of cord
blood thyroid stimulating hormone after external cephalic version. BJOG.
2001 Oct;108(10):1076-80.
112
220. Gitau R, Menson E, Pickles V, Fisk NM, Glover V, MacLachlan N. Umbilical cortisol levels as an indicator of the fetal stress response to assisted
vaginal delivery. Eur J Obstet Gynecol Reprod Biol. 2001 Sep;98(1):14-7.
221. Mears K, McAuliffe F, Grimes H, Morrison JJ. Fetal cortisol in relation to
labour, intrapartum events and mode of delivery. J Obstet Gynaecol. 2004
Feb;24(2):129-32.
222. Vogl SE, Worda C, Egarter C, Bieglmayer C, Szekeres T, Huber J, et al.
Mode of delivery is associated with maternal and fetal endocrine stress
response. BJOG. 2006 Apr;113(4):441-5.
223. Charmandari E, Tsigos C, Chrousos G. Endocrinology of the stress response.
Annu Rev Physiol. 2005;67:259-84.
224. Fukuda S. Correlation between function of the pituitary-thyroid axis and
metabolism of catecholamines by the fetus at delivery. Clin Endocrinol (Oxf).
1987 Sep;27(3):331-8.
225. Miyamoto N, Tsuji M, Imataki T, Nagamachi N, Hirose S, Hamada Y.
Influence of mode of delivery on fetal pituitary-thyroid axis. Acta Paediatr
Jpn. 1991 Jun;33(3):363-8.
226. Lao TT, Li CY, Panesar NS. Transient neonatal hyperthyrotropinaemia. Early
Hum Dev. 1992 Jan;28(1):19-25.
227. Gasparoni A, Ciardelli L, De Amici D, Castellazzi AM, Autelli M, Bottino R,
et al. Effect of general and epidural anaesthesia on thyroid hormones and
immunity in neonates. Paediatr Anaesth. 2002 Jan;12(1):59-64.
228. Rashmi, Seth A, Sekhri T, Agarwal A. Effect of perinatal factors on cord
blood thyroid stimulating hormone levels. J Pediatr Endocrinol Metab. 2007
Jan;20(1):59-64.
229. Thorpe-Beeston JG, Nicolaides KH, Snijders RJ, Felton CV, McGregor AM.
Thyroid function in small for gestational age fetuses. Obstet Gynecol. 1991
May;77(5):701-6.
230. Sullivan KM, May W, Nordenberg D, Houston R, Maberly GF. Use of
thyroid stimulating hormone testing in newborns to identify iodine deficiency. J Nutr. 1997 Jan;127(1):55-8.
231. Lao TT, Lee CP. Gestational diabetes mellitus and neonatal hyperthyrotropinemia. Gynecol Obstet Invest. 2002;53(3):135-9.
232. Clemens PC, Neumann S. Thyroid test abnormalities in birth-traumatic
injury: correlation with Apgar score. Am J Med. 1988 Sep;85(3):459-60.
233. Lee SS, Lao TT. Cord blood thyrotrophin and foetal presentation at delivery
in singleton pregnancies. Gynecol Obstet Invest. 1997;43(2):94-7.
234. Carrascosa A, Ruiz-Cuevas P, Potau N, Almar J, Salcedo S, Clemente M, et
al. Thyroid function in seventy-five healthy preterm infants thirty to thirtyfive weeks of gestational age: a prospective and longitudinal study during the
first year of life. Thyroid. 2004 Jun;14(6):435-42.
235. Fisher DA, Nelson JC, Carlton EI, Wilcox RB. Maturation of human
hypothalamic-pituitary-thyroid function and control. Thyroid. 2000 Mar;
10(3):229-34.
113
236. Fisher DA, Schoen EJ, La Franchi S, Mandel SH, Nelson JC, Carlton EI, et
al. The hypothalamic-pituitary-thyroid negative feedback control axis in
children with treated congenital hypothyroidism. J Clin Endocrinol Metab.
2000 Aug;85(8):2722-7.
237. Thorpe-Beeston JG, Nicolaides KH, Felton CV, Butler J, McGregor AM.
Maturation of the secretion of thyroid hormone and thyroid-stimulating
hormone in the fetus. N Engl J Med. 1991 Feb 21;324(8):532-6.
238. Burrow GN, Fisher DA, Larsen PR. Maternal and fetal thyroid function. N
Engl J Med. 1994 Oct 20;331(16):1072-8.
239. Sutandar M, Garcia-Bournissen F, Koren G. Hypothyroidism in pregnancy. J
Obstet Gynaecol Can. 2007 Apr;29(4):354-6.
240. Leung AS, Millar LK, Koonings PP, Montoro M, Mestman JH. Perinatal
outcome in hypothyroid pregnancies. Obstet Gynecol. 1993 Mar;81(3):34953.
241. LaFranchi SH, Haddow JE, Hollowell JG. Is thyroid inadequacy during
gestation a risk factor for adverse pregnancy and developmental outcomes?
Thyroid. 2005 Jan;15(1):60-71.
242. Idris I, Srinivasan R, Simm A, Page RC. Maternal hypothyroidism in early
and late gestation: effects on neonatal and obstetric outcome. Clin Endocrinol
(Oxf). 2005 Nov;63(5):560-5.
243. Wolfberg AJ, Lee-Parritz A, Peller AJ, Lieberman ES. Obstetric and neonatal
outcomes associated with maternal hypothyroid disease. J Matern Fetal
Neonatal Med. 2005 Jan;17(1):35-8.
244. Tan TO, Cheng YW, Caughey AB. Are women who are treated for
hypothyroidism at risk for pregnancy complications? Am J Obstet Gynecol.
2006 May;194(5):e1-3.
245. Pop VJ, Kuijpens JL, van Baar AL, Verkerk G, van Son MM, de Vijlder JJ, et
al. Low maternal free thyroxine concentrations during early pregnancy are
associated with impaired psychomotor development in infancy. Clin
Endocrinol (Oxf). 1999 Feb;50(2):149-55.
246. Kasatkina EP, Samsonova LN, Ivakhnenko VN, Ibragimova GV, Ryabykh
AV, Naumenko LL, et al. Gestational hypothyroxinemia and cognitive
function in offspring. Neurosci Behav Physiol. 2006 Jul;36(6):619-24.
247. Ashoor G, Kametas NA, Akolekar R, Guisado J, Nicolaides KH. Maternal
thyroid function at 11-13 weeks of gestation. Fetal Diagn Ther. 2010;
27(3):156-63.
248. Bunevicius R, Kusminskas L, Mickuviene N, Bunevicius A, Pedersen CA,
Pop VJ. Depressive disorder and thyroid axis functioning during pregnancy.
World J Biol Psychiatry. 2009 Aug 12:1-6.
249. Ashworth A. Effects of intrauterine growth retardation on mortality and
morbidity in infants and young children. Eur J Clin Nutr. 1998 Jan;52 Suppl
1:S34-41; discussion S-2.
114
250. Barker DJ, Thornburg KL, Osmond C, Kajantie E, Eriksson JG. The surface
area of the placenta and hypertension in the offspring in later life. Int J Dev
Biol. 2010;54(2-3):525-30.
251. Henriksen T. The macrosomic fetus: a challenge in current obstetrics. Acta
Obstet Gynecol Scand. 2008;87(2):134-45.
252. Barker DJ. The origins of the developmental origins theory. J Intern Med.
2007 May;261(5):412-7.
253. Rosenberg TJ, Garbers S, Chavkin W, Chiasson MA. Prepregnancy weight
and adverse perinatal outcomes in an ethnically diverse population. Obstet
Gynecol. 2003 Nov;102(5 Pt 1):1022-7.
254. Jensen DM, Damm P, Sorensen B, Molsted-Pedersen L, Westergaard JG,
Ovesen P, et al. Pregnancy outcome and prepregnancy body mass index in
2459 glucose-tolerant Danish women. Am J Obstet Gynecol. 2003 Jul;
189(1):239-44.
255. Clausen T, Burski TK, Oyen N, Godang K, Bollerslev J, Henriksen T.
Maternal anthropometric and metabolic factors in the first half of pregnancy
and risk of neonatal macrosomia in term pregnancies. A prospective study.
Eur J Endocrinol. 2005 Dec;153(6):887-94.
256. Verhaeghe J, Pintiaux A, Van Herck E, Hennen G, Foidart JM, Igout A.
Placental GH, IGF-I, IGF-binding protein-1, and leptin during a glucose
challenge test in pregnant women: relation with maternal body weight,
glucose tolerance, and birth weight. J Clin Endocrinol Metab. 2002 Jun;
87(6):2875-82.
257. Watkins AJ, Wilkins A, Cunningham C, Perry VH, Seet MJ, Osmond C, et al.
Low protein diet fed exclusively during mouse oocyte maturation leads to
behavioural and cardiovascular abnormalities in offspring. J Physiol. 2008
Apr 15;586(8):2231-44.
258. Watkins AJ, Lucas ES, Torrens C, Cleal JK, Green L, Osmond C, et al.
Maternal low-protein diet during mouse pre-implantation development
induces vascular dysfunction and altered renin-angiotensin-system
homeostasis in the offspring. Br J Nutr. 2010 Jun;103(12):1762-70.
259. Godfrey K, Robinson S, Barker DJ, Osmond C, Cox V. Maternal nutrition in
early and late pregnancy in relation to placental and fetal growth. BMJ. 1996
Feb 17;312(7028):410-4.
260. Barker DJ, Bergmann RL, Ogra PL. Concluding remarks. The Window of
Opportunity: Pre-Pregnancy to 24 Months of Age. Nestle Nutr Workshop Ser
Pediatr Program. 2008;61:255-60.
261. Talge NM, Neal C, Glover V. Antenatal maternal stress and long-term effects
on child neurodevelopment: how and why? J Child Psychol Psychiatry. 2007
Mar-Apr;48(3-4):245-61.
262. Bulik CM, Sullivan PF, Kendler KS. Medical and psychiatric morbidity in
obese women with and without binge eating. Int J Eat Disord. 2002 Jul;
32(1):72-8.
115
263. Heron J, O'Connor TG, Evans J, Golding J, Glover V. The course of anxiety
and depression through pregnancy and the postpartum in a community
sample. J Affect Disord. 2004 May;80(1):65-73.
264. Cott AD, Wisner KL. Psychiatric disorders during pregnancy. Int Rev
Psychiatry. 2003 Aug;15(3):217-30.
265. Mulder EJ, Robles de Medina PG, Huizink AC, Van den Bergh BR, Buitelaar
JK, Visser GH. Prenatal maternal stress: effects on pregnancy and the
(unborn) child. Early Hum Dev. 2002 Dec;70(1-2):3-14.
266. Alder J, Fink N, Bitzer J, Hosli I, Holzgreve W. Depression and anxiety
during pregnancy: a risk factor for obstetric, fetal and neonatal outcome? A
critical review of the literature. J Matern Fetal Neonatal Med. 2007 Mar;
20(3):189-209.
267. Dole N, Savitz DA, Hertz-Picciotto I, Siega-Riz AM, McMahon MJ, Buekens
P. Maternal stress and preterm birth. Am J Epidemiol. 2003 Jan 1;157(1):1424.
268. Copper RL, Goldenberg RL, Das A, Elder N, Swain M, Norman G, et al. The
preterm prediction study: maternal stress is associated with spontaneous
preterm birth at less than thirty-five weeks' gestation. National Institute of
Child Health and Human Development Maternal-Fetal Medicine Units
Network. Am J Obstet Gynecol. 1996 Nov;175(5):1286-92.
269. Rondo PH, Ferreira RF, Nogueira F, Ribeiro MC, Lobert H, Artes R.
Maternal psychological stress and distress as predictors of low birth weight,
prematurity and intrauterine growth retardation. Eur J Clin Nutr. 2003
Feb;57(2):266-72.
270. Grote NK, Bridge JA, Gavin AR, Melville JL, Iyengar S, Katon WJ. A metaanalysis of depression during pregnancy and the risk of preterm birth, low
birth weight, and intrauterine growth restriction. Arch Gen Psychiatry. 2010
Oct;67(10):1012-24.
271. Anderson SE, Cohen P, Naumova EN, Must A. Association of depression and
anxiety disorders with weight change in a prospective community-based
study of children followed up into adulthood. Arch Pediatr Adolesc Med.
2006 Mar;160(3):285-91.
272. Bunevicius A, Kusminskas L, Bunevicius R. Validation of the Lithuanian
version of the Edinburgh Postnatal Depression Scale. Medicina (Kaunas).
2009;45(7):544-8.
273. Austin MP, Tully L, Parker G. Examining the relationship between antenatal
anxiety and postnatal depression. J Affect Disord. 2007 Aug;101(1-3):169-74.
274. O'Connor TG, Heron J, Glover V. Antenatal anxiety predicts child behavioral/emotional problems independently of postnatal depression. J Am Acad
Child Adolesc Psychiatry. 2002 Dec;41(12):1470-7.
275. Cannon M, Jones PB, Murray RM. Obstetric complications and schizophrenia: historical and meta-analytic review. Am J Psychiatry. 2002 Jul;
159(7):1080-92.
116
276. Glover V, O'Connor TG. Effects of antenatal stress and anxiety: Implications
for development and psychiatry. Br J Psychiatry. 2002 May;180:389-91.
277. O'Connor TG, Heron J, Golding J, Beveridge M, Glover V. Maternal
antenatal anxiety and children's behavioural/emotional problems at 4 years.
Report from the Avon Longitudinal Study of Parents and Children. Br J
Psychiatry. 2002 Jun;180:502-8.
278. Hosseini SM, Biglan MW, Larkby C, Brooks MM, Gorin MB, Day NL. Trait
anxiety in pregnant women predicts offspring birth outcomes. Paediatr
Perinat Epidemiol. 2009 Nov;23(6):557-66.
279. Steptoe A, Wardle J, Pollard TM, Canaan L, Davies GJ. Stress, social support
and health-related behavior: a study of smoking, alcohol consumption and
physical exercise. J Psychosom Res. 1996 Aug;41(2):171-80.
280. Reynolds RM, Walker BR, Syddall HE, Andrew R, Wood PJ, Whorwood
CB, et al. Altered control of cortisol secretion in adult men with low birth
weight and cardiovascular risk factors. J Clin Endocrinol Metab. 2001
Jan;86(1):245-50.
281. Teixeira JM, Fisk NM, Glover V. Association between maternal anxiety in
pregnancy and increased uterine artery resistance index: cohort based study.
BMJ. 1999 Jan 16;318(7177):153-7.
282. Kent A, Hughes P, Ormerod L, Jones G, Thilaganathan B. Uterine artery
resistance and anxiety in the second trimester of pregnancy. Ultrasound
Obstet Gynecol. 2002 Feb;19(2):177-9.
283. Pluess M, Bolten M, Pirke KM, Hellhammer D. Maternal trait anxiety,
emotional distress, and salivary cortisol in pregnancy. Biol Psychol. 2010
Mar;83(3):169-75.
284. Cohen H, Kaplan Z, Kozlovsky N, Gidron Y, Matar MA, Zohar J.
Hippocampal microinfusion of oxytocin attenuates the behavioural response
to stress by means of dynamic interplay with the glucocorticoid-catecholamine responses. J Neuroendocrinol. 2010 Aug;22(8):889-904.
285. Parker VJ, Douglas AJ. Stress in early pregnancy: maternal neuro-endocrineimmune responses and effects. J Reprod Immunol. 2010 May;85(1):86-92.
286. Douglas AJ. Mother-offspring dialogue in early pregnancy: Impact of adverse
environment on pregnancy maintenance and neurobiology. Prog Neuropsychopharmacol Biol Psychiatry. 2010 Aug 3.
287. Zuluaga MJ, Agrati D, Pereira M, Uriarte N, Fernandez-Guasti A, Ferreira A.
Experimental anxiety in the black and white model in cycling, pregnant and
lactating rats. Physiol Behav. 2005 Feb 15;84(2):279-86.
288. Toufexis DJ, Davis C, Hammond A, Davis M. Progesterone attenuates
corticotropin-releasing factor-enhanced but not fear-potentiated startle via the
activity of its neuroactive metabolite, allopregnanolone. J Neurosci. 2004
Nov 10;24(45):10280-7.
289. Macbeth AH, Gautreaux C, Luine VN. Pregnant rats show enhanced spatial
memory, decreased anxiety, and altered levels of monoaminergic neurotransmitters. Brain Res. 2008 Nov 19;1241:136-47.
117
290. Rini CK, Dunkel-Schetter C, Wadhwa PD, Sandman CA. Psychological
adaptation and birth outcomes: the role of personal resources, stress, and
sociocultural context in pregnancy. Health Psychol. 1999 Jul;18(4):333-45.
291. Poudevigne MS, O'Connor PJ. A review of physical activity patterns in
pregnant women and their relationship to psychological health. Sports Med.
2006;36(1):19-38.
292. Doremus-Fitzwater TL, Varlinskaya EI, Spear LP. Social and non-social
anxiety in adolescent and adult rats after repeated restraint. Physiol Behav.
2009 Jun 22;97(3-4):484-94.
293. Adams SH, Cartwright LK, Ostrove JM, Stewart AJ, Wink P. Psychological
predictors of good health in three longitudinal samples of educated midlife
women. Health Psychol. 1998 Sep;17(5):412-20.
294. John OP, Pervin LA, editors. Handbook of personality: theory and research.
Guilford, New York1999.
295. O'Leary MM, Loney BR, Eckel LA. Gender differences in the association
between psychopathic personality traits and cortisol response to induced
stress. Psychoneuroendocrinology. 2007 Feb;32(2):183-91.
296. Oswald LM, Zandi P, Nestadt G, Potash JB, Kalaydjian AE, Wand GS.
Relationship between cortisol responses to stress and personality. Neuropsychopharmacology. 2006 Jul;31(7):1583-91.
297. Buyukgebiz A. Newborn screening for congenital hypothyroidism. J Pediatr
Endocrinol Metab. 2006 Nov;19(11):1291-8.
298. Diagnostic and Statistical Manual of Mental Disorders. 3rdEdition-Revised
(DSM-III-R) ed. Washington, DC: American Psychiatric Association; 1987.
299. Lapkiene L, Mockute I, Nadisauskiene R. Edinburgo pogimdymines
depresijos skales (EPDS) adaptavimas naudoti Lietuvoje. Lietuvos akuserija
ir ginekologija. 2004;7:280-4.
300. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression.
Development of the 10-item Edinburgh Postnatal Depression Scale. Br J
Psychiatry. 1987 Jun;150:782-6.
301. Figueiredo B, Pacheco A, Costa R. Depression during pregnancy and the
postpartum period in adolescent and adult Portuguese mothers. Arch Womens
Ment Health. 2007;10(3):103-9.
302. Cattel RB, Scheier IH, editors. The meaning and measurement of neoroticism
and anxiety. New York, Ronald1961.
303. Van den Bergh BR, Van Calster B, Smits T, Van Huffel S, Lagae L.
Antenatal maternal anxiety is related to HPA-axis dysregulation and selfreported depressive symptoms in adolescence: a prospective study on the fetal
origins of depressed mood. Neuropsychopharmacology. 2008 Feb;33(3):53645.
304. Solberg HE. International Federation of Clinical Chemistry (IFCC), Scientific
Committee, Clinical Section, Expert Panel on Theory of Reference Values,
and International Committee for Standardization in Haematology (ICSH),
Standing Committee on Reference Values. Approved Recommendation
118
305.
306.
307.
308.
309.
310.
311.
312.
313.
314.
315.
316.
317.
(1986) on the theory of reference values. Part 1. The concept of reference
values. J Clin Chem Clin Biochem. 1987 May;25(5):337-42.
Preedy VR, Burrow GN, Watson R, editors. Comprehensive Handbook of
Iodine: Nutritional, Biochemical, Pathological and Therapeutic Aspects.
Amsterdam: Elsevier; 2009.
Glinoer D, Delange F. The potential repercussions of maternal, fetal, and
neonatal hypothyroxinemia on the progeny. Thyroid. 2000 Oct;10(10):87187.
Pedersen KM, Laurberg P, Iversen E, Knudsen PR, Gregersen HE,
Rasmussen OS, et al. Amelioration of some pregnancy-associated variations
in thyroid function by iodine supplementation. J Clin Endocrinol Metab. 1993
Oct;77(4):1078-83.
Berghout A, Endert E, Ross A, Hogerzeil HV, Smits NJ, Wiersinga WM.
Thyroid function and thyroid size in normal pregnant women living in an
iodine replete area. Clin Endocrinol (Oxf). 1994 Sep;41(3):375-9.
Buxton OM, Frank SA, L'Hermite-Baleriaux M, Leproult R, Turek FW, Van
Cauter E. Roles of intensity and duration of nocturnal exercise in causing
phase delays of human circadian rhythms. Am J Physiol. 1997 Sep;273(3 Pt
1):E536-42.
Scobbo RR, VonDohlen TW, Hassan M, Islam S. Serum TSH variability in
normal individuals: the influence of time of sample collection. W V Med J.
2004 Jul-Aug;100(4):138-42.
Weibel L, Brandenberger G, Goichot B, Spiegel K, Ehrhart J, Follenius M.
The circadian thyrotropin rhythm is delayed in regular night workers.
Neurosci Lett. 1995 Mar 3;187(2):83-6.
Brabant G, Prank K, Ranft U, Schuermeyer T, Wagner TO, Hauser H, et al.
Physiological regulation of circadian and pulsatile thyrotropin secretion in
normal man and woman. J Clin Endocrinol Metab. 1990 Feb;70(2):403-9.
Gary KA, Winokur A, Douglas SD, Kapoor S, Zaugg L, Dinges DF. Total
sleep deprivation and the thyroid axis: effects of sleep and waking activity.
Aviat Space Environ Med. 1996 Jun;67(6):513-9.
Weeke J, Gundersen HJ. Circadian and 30 minutes variations in serum TSH
and thyroid hormones in normal subjects. Acta Endocrinol (Copenh). 1978
Dec;89(4):659-72.
Jensen E, Blaabjerg O, Petersen PH, Hegedus L. Sampling time is important
but may be overlooked in establishment and use of thyroid-stimulating
hormone reference intervals. Clin Chem. 2007 Feb;53(2):355-6.
La'ulu SL, Roberts WL. Second-trimester reference intervals for thyroid tests:
the role of ethnicity. Clin Chem. 2007 Sep;53(9):1658-64.
Pekonen F, Alfthan H, Stenman UH, Ylikorkala O. Human chorionic
gonadotropin (hCG) and thyroid function in early human pregnancy:
circadian variation and evidence for intrinsic thyrotropic activity of hCG. J
Clin Endocrinol Metab. 1988 Apr;66(4):853-6.
119
318. Ballabio M, Poshychinda M, Ekins RP. Pregnancy-induced changes in
thyroid function: role of human chorionic gonadotropin as putative regulator
of maternal thyroid. J Clin Endocrinol Metab. 1991 Oct;73(4):824-31.
319. Glinoer D. What happens to the normal thyroid during pregnancy? Thyroid.
1999 Jul;9(7):631-5.
320. Bocos-Terraz JP, Izquierdo-Alvarez S, Bancalero-Flores JL, AlvarezLahuerta R, Aznar-Sauca A, Real-Lopez E, et al. Thyroid hormones according to gestational age in pregnant Spanish women. BMC Res Notes. 2009;
2:237.
321. de Escobar GM, Obregon MJ, del Rey FE. Iodine deficiency and brain
development in the first half of pregnancy. Public Health Nutr. 2007
Dec;10(12A):1554-70.
322. Moleti M, Lo Presti VP, Campolo MC, Mattina F, Galletti M, Mandolfino M,
et al. Iodine prophylaxis using iodized salt and risk of maternal thyroid failure
in conditions of mild iodine deficiency. J Clin Endocrinol Metab. 2008 Jul;
93(7):2616-21.
323. Lambert-Messerlian G, McClain M, Haddow JE, Palomaki GE, Canick JA,
Cleary-Goldman J, et al. First- and second-trimester thyroid hormone
reference data in pregnant women: a FaSTER (First- and Second-Trimester
Evaluation of Risk for aneuploidy) Research Consortium study. Am J Obstet
Gynecol. 2008 Jul;199(1):62 e1-6.
324. Damjanovic SS, Stojic RV, Lalic NM, Jotic AZ, Macut DP, Ognjanovic SI, et
al. Relationship between basal metabolic rate and cortisol secretion throughout pregnancy. Endocrine. 2009 Apr;35(2):262-8.
325. Roti E, Gardini E, Minelli R, Bianconi L, Flisi M. Thyroid function
evaluation by different commercially available free thyroid hormone measurement kits in term pregnant women and their newborns. J Endocrinol
Invest. 1991 Jan;14(1):1-9.
326. Mannisto T, Surcel HM, Ruokonen A, Vaarasmaki M, Pouta A, Bloigu A, et
al. Early pregnancy reference intervals of thyroid hormone concentrations in a
thyroid antibody-negative pregnant population. Thyroid. 2011 Mar;21(3):
291-8.
327. Roberts RF, La'ulu SL, Roberts WL. Performance characteristics of seven
automated thyroxine and T-uptake methods. Clin Chim Acta. 2007 Feb;
377(1-2):248-55.
328. Mockute I, Svedas E, Kusminskas L, Raskauskiene N. Iodine deficiency
assessed by the newborn thyrotropin concentrations. Lietuvos akuserija ir
ginekologija. 2010;XIII(2):131-2.
329. WHO/ICCIDD/UNICEF. World Summit for Children—Mid-Decade Goal:
Iodine Deficiency Disorders. Geneva, Switzerland1994.
330. . Elimination of Iodine Deficiency Disorders (IDD) in Central and Eastern
Europe, the Commonwealth of independant states, and the Baltic States.
WHO/EURO/NUT/981; 1997 3-6 september, 1997; Miunich, Germany.
120
331. Barzda AK, V. Jodo trūkumas: problema ir sprendimo būdai. Lietuvos
sveikata [serial on the Internet]. 2005 lapkričio 17 - 23 d.; (NR. 46 (627)):
Available from: http://www.lsveikata.lt/senas/index.php?page_id=99&s=265.
332. Zimmermann MB. The impact of iodised salt or iodine supplements on iodine
status during pregnancy, lactation and infancy. Public Health Nutr. 2007
Dec;10(12A):1584-95.
333. Caldwell KL, Miller GA, Wang RY, Jain RB, Jones RL. Iodine status of the
U.S. population, National Health and Nutrition Examination Survey 20032004. Thyroid. 2008 Nov;18(11):1207-14.
334. Hetzel BS. Iodine deficiency disorders (IDD) and their eradication. Lancet.
1983 Nov 12;2(8359):1126-9.
335. Zimmermann MB, Hess SY, Molinari L, De Benoist B, Delange F,
Braverman LE, et al. New reference values for thyroid volume by ultrasound
in iodine-sufficient schoolchildren: a World Health Organization/Nutrition for
Health and Development Iodine Deficiency Study Group Report. Am J Clin
Nutr. 2004 Feb;79(2):231-7.
336. Central and Eastern Europe, Commonwealth of Independent States and the
Baltics Region: UNICEF2005.
337. Leung AM, Pearce EN, Braverman LE. Iodine content of prenatal
multivitamins in the United States. N Engl J Med. 2009 Feb 26;360(9):93940.
338. Ciardelli R, Haumont D, Gnat D, Vertongen F, Delange F. The nutritional
iodine supply of Belgian neonates is still insufficient. Eur J Pediatr. 2002
Oct;161(10):519-23.
339. Naujagimių registro duomenys [database on the Internet]. Lietuvos sveikatos
informacijos centras. Available from: http://www.lsic.lt/.
340. Cunningham FG, Norman FG, Kenneth JL. Fetal Abnormalities: Inherited
and Aquired Disorders. In: Seils A, Noujaim SR, Davis K, editors. Williams
Obstetrics. 21st edition ed: The McGraw Hill Companies, Inc; 2001. p. 94186.
341. The International Cleringhouse for Birth Defects. Available from: http://
www.icbdsr.org.
342. European Surveillance of Congenital Anomalies. Available from:
http://www.eurocat-network.eu/HomePage.
343. Olivieri A, Stazi MA, Mastroiacovo P, Fazzini C, Medda E, Spagnolo A, et
al. A population-based study on the frequency of additional congenital
malformations in infants with congenital hypothyroidism: data from the
Italian Registry for Congenital Hypothyroidism (1991-1998). J Clin Endocrinol Metab. 2002 Feb;87(2):557-62.
344. Gu YH, Harada S, Kato T, Inomata H, Aoki K, Hirahara F. Increased
incidence of extrathyroidal congenital malformations in Japanese patients
with congenital hypothyroidism and their relationship with Down syndrome
and other factors. Thyroid. 2009 Aug;19(8):869-79.
121
345. Cassio A, Tatò L, Colli C, Spolettini E, Costantini E, Cacciari E. Incidence of
congenital malformations in congenital hypothyroidism. Screening. 1994
December Volume 3(Issue 3):125-30
346. Zimmermann M, Delange F. Iodine supplementation of pregnant women in
Europe: a review and recommendations. Eur J Clin Nutr. 2004 Jul;58(7):97984.
347. SOGC Clinical Practice Guidelines: The use of folic acid for the prevention
of neural tube defects and other congenital anomalies [database on the
Internet]2003, November. Available from: http://www.sogc.org/guidelines/
public/138E-CPG-November2003.pdf.
348. Periconceptional supplementation with folate and/or multivitamins for
preventing neural tube defects [database on the Internet]. John Wiley & Sons,
Ltd. 2001. Available from: http://www.mrw.interscience.wiley.com/cochrane/
clsysrev/articles/CD001056/frame.html.
349. Murphy N, Hume R, van Toor H, Matthews TG, Ogston SA, Wu SY, et al.
The hypothalamic-pituitary-thyroid axis in preterm infants; changes in the
first 24 hours of postnatal life. J Clin Endocrinol Metab. 2004 Jun;89(6):
2824-31.
350. Mariotti S. Physiology of Hypothalamus-Pituitary-Thyroid System and
Relation to Neural and Endocrine Systems Last revised: January 5, 2006;
Available from: www.thyroidmanager.org.
351. Chan LY, Leung TN, Lau TK. Influences of perinatal factors on cord blood
thyroid-stimulating hormone level. Acta Obstet Gynecol Scand. 2001
Nov;80(11):1014-8.
352. Kaloumenou I, Duntas LH, Alevizaki M, Mantzou E, Chiotis D, Mengreli C,
et al. Gender, age, puberty, and BMI related changes of TSH and thyroid
hormones in schoolchildren living in a long-standing iodine replete area.
Horm Metab Res. 2010 Apr;42(4):285-9.
353. Trimble LS. What the obstetrician/gynecologist should know about thyroid
disorders. Obsterical and gynecological survey. 2011;65(12).
354. Poppe K, Velkeniers B, Glinoer D. The role of thyroid autoimmunity in
fertility and pregnancy. Nat Clin Pract Endocrinol Metab. 2008 Jul;4(7):394405.
355. Turan S, Bereket A, Angaji M, Koroglu OA, Bilgen H, Onver T, et al. The
effect of the mode of delivery on neonatal thyroid function. J Matern Fetal
Neonatal Med. 2007 Jun;20(6):473-6.
356. Shi LX, Ma QL, Zhang JX. [Influence of perinatal factors and sampling
methods on thyroid stimulating hormone and thyroid hormone levels in cord
blood]. Zhonghua Fu Chan Ke Za Zhi. 1994 Dec;29(12):714-6, 60-1.
357. Glinoer D, Delange F, Laboureur I, de Nayer P, Lejeune B, Kinthaert J, et al.
Maternal and neonatal thyroid function at birth in an area of marginally low
iodine intake. 1992. p. 800-5.
122
358. Hull HR, Dinger MK, Knehans AW, Thompson DM, Fields DA. Impact of
maternal body mass index on neonate birthweight and body composition. Am
J Obstet Gynecol. 2008 Apr;198(4):416 e1-6.
359. Ehrenberg HM, Durnwald CP, Catalano P, Mercer BM. The influence of
obesity and diabetes on the risk of cesarean delivery. Am J Obstet Gynecol.
2004 Sep;191(3):969-74.
360. Szostak-Wegierek D, Szamotulska K, Szponar L. [Influence of maternal
nutrition on infant birthweight]. Ginekol Pol. 2004 Sep;75(9):692-8.
361. Burrows RF. Maternal characteristics and their influences on birth weight in a
Melanesian population. Asia Oceania J Obstet Gynaecol. 1988 Mar;14(1):1-5.
362. Dhall K, Bagga R. Maternal determinants of birth weight of north Indian
babies. Indian J Pediatr. 1995 May-Jun;62(3):333-44.
363. Rebagliato M, Florey Cdu V, Bolumar F. Exposure to environmental tobacco
smoke in nonsmoking pregnant women in relation to birth weight. Am J
Epidemiol. 1995 Sep 1;142(5):531-7.
364. Conti J, Abraham S, Taylor A. Eating behavior and pregnancy outcome. J
Psychosom Res. 1998 Mar-Apr;44(3-4):465-77.
365. Micali N, Simonoff E, Treasure J. Risk of major adverse perinatal outcomes
in women with eating disorders. Br J Psychiatry. 2007 Mar;190:255-9.
366. Kirchengast S, Hartmann B. Maternal prepregnancy weight status and
pregnancy weight gain as major determinants for newborn weight and size.
Ann Hum Biol. 1998 Jan-Feb;25(1):17-28.
367. Galtier-Dereure F, Boulot P. [Obstetrical complications of maternal
overweight]. Contracept Fertil Sex. 1994 Feb;22(2):113-6.
368. Galtier-Dereure F, Boegner C, Bringer J. Obesity and pregnancy:
complications and cost. Am J Clin Nutr. 2000 May;71(5 Suppl):1242S-8S.
369. Kajantie E, Osmond C, Barker DJ, Forsen T, Phillips DI, Eriksson JG. Size at
birth as a predictor of mortality in adulthood: a follow-up of 350 000 personyears. Int J Epidemiol. 2005 Jun;34(3):655-63.
370. Lu GC, Rouse DJ, DuBard M, Cliver S, Kimberlin D, Hauth JC. The effect of
the increasing prevalence of maternal obesity on perinatal morbidity. Am J
Obstet Gynecol. 2001 Oct;185(4):845-9.
371. Ehrenberg HM, Dierker L, Milluzzi C, Mercer BM. Prevalence of maternal
obesity in an urban center. Am J Obstet Gynecol. 2002 Nov;187(5):1189-93.
372. Osmond C, Kajantie E, Forsen TJ, Eriksson JG, Barker DJ. Infant growth and
stroke in adult life: the Helsinki birth cohort study. Stroke. 2007 Feb;
38(2):264-70.
373. Wu G, Bazer FW, Cudd TA, Meininger CJ, Spencer TE. Maternal nutrition
and fetal development. J Nutr. 2004 Sep;134(9):2169-72.
374. Joglekar CV, Fall CH, Deshpande VU, Joshi N, Bhalerao A, Solat V, et al.
Newborn size, infant and childhood growth, and body composition and
cardiovascular disease risk factors at the age of 6 years: the Pune Maternal
Nutrition Study. Int J Obes (Lond). 2007 Oct;31(10):1534-44.
123
375. Jaddoe VW, Witteman JC. Hypotheses on the fetal origins of adult diseases:
contributions of epidemiological studies. Eur J Epidemiol. 2006;21(2):91102.
376. Weight Gain During Pregnancy: Reexamining the Guidelines: Institute of
Medicine of National Academies. Food and Nutrition Board2009.
377. Davis LE, Lucas MJ, Hankins GD, Roark ML, Cunningham FG. Thyrotoxicosis complicating pregnancy. Am J Obstet Gynecol. 1989 Jan;160(1):
63-70.
378. Millar LK, Wing DA, Leung AS, Koonings PP, Montoro MN, Mestman JH.
Low birth weight and preeclampsia in pregnancies complicated by
hyperthyroidism. Obstet Gynecol. 1994 Dec;84(6):946-9.
379. Phoojaroenchanachai M, Sriussadaporn S, Peerapatdit T, Vannasaeng S,
Nitiyanant W, Boonnamsiri V, et al. Effect of maternal hyperthyroidism
during late pregnancy on the risk of neonatal low birth weight. Clin
Endocrinol (Oxf). 2001 Mar;54(3):365-70.
380. Cleary-Goldman J, Malone FD, Lambert-Messerlian G, Sullivan L, Canick J,
Porter TF, et al. Maternal thyroid hypofunction and pregnancy outcome.
Obstet Gynecol. 2008 Jul;112(1):85-92.
381. Knudsen N, Laurberg P, Rasmussen LB, Bulow I, Perrild H, Ovesen L, et al.
Small differences in thyroid function may be important for body mass index
and the occurrence of obesity in the population. J Clin Endocrinol Metab.
2005 Jul;90(7):4019-24.
382. Shon HS, Jung ED, Kim SH, Lee JH. Free T4 is negatively correlated with
body mass index in euthyroid women. Korean J Intern Med. 2008
Jun;23(2):53-7.
383. Hoogwerf BJ, Nuttall FQ. Long-term weight regulation in treated
hyperthyroid and hypothyroid subjects. Am J Med. 1984 Jun;76(6):963-70.
384. Alvarez-Pedrerol M, Guxens M, Mendez M, Canet Y, Martorell R, Espada
M, et al. Iodine levels and thyroid hormones in healthy pregnant women and
birth weight of their offspring. Eur J Endocrinol. 2009 Mar;160(3):423-9.
385. Gaynes BN, Gavin N, Meltzer-Brody S, Lohr KN, Swinson T, Gartlehner G,
et al. Perinatal depression: prevalence, screening accuracy, and screening
outcomes. Evid Rep Technol Assess (Summ). 2005 Feb(119):1-8.
386. Pajulo M, Savonlahti E, Sourander A, Helenius H, Piha J. Antenatal depression, substance dependency and social support. J Affect Disord. 2001
Jun;65(1):9-17.
387. Pinheiro SN, Laprega MR, Furtado EF. [Psychiatric morbidity and alcohol
use by pregnant women in a public obstetric service]. Rev Saude Publica.
2005 Aug;39(4):593-8.
388. Kelly RH, Danielsen BH, Golding JM, Anders TF, Gilbert WM, Zatzick DF.
Adequacy of prenatal care among women with psychiatric diagnoses giving
birth in California in 1994 and 1995. Psychiatr Serv. 1999 Dec;50(12):158490.
124
389. Zuckerman B, Amaro H, Bauchner H, Cabral H. Depressive symptoms
during pregnancy: relationship to poor health behaviors. Am J Obstet
Gynecol. 1989 May;160(5 Pt 1):1107-11.
390. Ryan D, Milis L, Misri N. Depression during pregnancy. Can Fam Physician.
2005 Aug;51:1087-93.
391. Kurki T, Hiilesmaa V, Raitasalo R, Mattila H, Ylikorkala O. Depression and
anxiety in early pregnancy and risk for preeclampsia. Obstet Gynecol. 2000
Apr;95(4):487-90.
392. Dayan J, Creveuil C, Marks MN, Conroy S, Herlicoviez M, Dreyfus M, et al.
Prenatal depression, prenatal anxiety, and spontaneous preterm birth: a
prospective cohort study among women with early and regular care. Psychosom Med. 2006 Nov-Dec;68(6):938-46.
393. Da-Silva VA, Moraes-Santos AR, Carvalho MS, Martins ML, Teixeira NA.
Prenatal and postnatal depression among low income Brazilian women. Braz
J Med Biol Res. 1998 Jun;31(6):799-804.
394. Rahman A, Bunn J, Lovel H, Creed F. Association between antenatal
depression and low birthweight in a developing country. Acta Psychiatr
Scand. 2007 Jun;115(6):481-6.
395. Wadhwa PD, Sandman CA, Porto M, Dunkel-Schetter C, Garite TJ. The
association between prenatal stress and infant birth weight and gestational age
at birth: a prospective investigation. Am J Obstet Gynecol. 1993 Oct;169(4):
858-65.
396. Hedegaard M, Henriksen TB, Sabroe S, Secher NJ. Psychological distress in
pregnancy and preterm delivery. BMJ. 1993 Jul 24;307(6898):234-9.
397. Andersson L, Sundstrom-Poromaa I, Wulff M, Astrom M, Bixo M.
Depression and anxiety during pregnancy and six months postpartum: a
follow-up study. Acta Obstet Gynecol Scand. 2006;85(8):937-44.
398. Berle JO, Mykletun A, Daltveit AK, Rasmussen S, Holsten F, Dahl AA.
Neonatal outcomes in offspring of women with anxiety and depression during
pregnancy. A linkage study from The Nord-Trondelag Health Study (HUNT)
and Medical Birth Registry of Norway. Arch Womens Ment Health. 2005
Sep;8(3):181-9.
399. Larsson C, Sydsjo G, Josefsson A. Health, sociodemographic data, and
pregnancy outcome in women with antepartum depressive symptoms. Obstet
Gynecol. 2004 Sep;104(3):459-66.
400. Nakamura K, Sheps S, Arck PC. Stress and reproductive failure: past notions,
present insights and future directions. J Assist Reprod Genet. 2008 FebMar;25(2-3):47-62.
401. Seckl JR, Meaney MJ. Glucocorticoid programming. Ann N Y Acad Sci.
2004 Dec;1032:63-84.
402. Rothenberg SJ, Chicz-DeMet A, Schnaas L, Karchmer S, Salinas V, Guzman
LA. Umbilical cord beta-endorphin and early childhood motor development.
Early Hum Dev. 1996 Sep 20;46(1-2):83-95.
125
403. Hansen D, Lou HC, Olsen J. Serious life events and congenital malformations: a national study with complete follow-up. Lancet. 2000 Sep
9;356(9233):875-80.
404. Obel C, Hedegaard M, Henriksen TB, Secher NJ, Olsen J, Levine S. Stress
and salivary cortisol during pregnancy. Psychoneuroendocrinology. 2005
Aug;30(7):647-56.
405. Nierop A, Bratsikas A, Klinkenberg A, Nater UM, Zimmermann R, Ehlert U.
Prolonged salivary cortisol recovery in second-trimester pregnant women and
attenuated salivary alpha-amylase responses to psychosocial stress in human
pregnancy. J Clin Endocrinol Metab. 2006 Apr;91(4):1329-35.
406. Gitau R, Cameron A, Fisk NM, Glover V. Fetal exposure to maternal cortisol.
Lancet. 1998 Aug 29;352(9129):707-8.
407. Challis JR, Matthews SG, Van Meir C, Ramirez MM. Current topic: the
placental corticotrophin-releasing hormone-adrenocorticotrophin axis. Placenta. 1995 Sep;16(6):481-502.
408. Field T, Diego M. Cortisol: the culprit prenatal stress variable. Int J Neurosci.
2008 Aug;118(8):1181.
409. Sun K, Adamson SL, Yang K, Challis JR. Interconversion of cortisol and
cortisone by 11beta-hydroxysteroid dehydrogenases type 1 and 2 in the
perfused human placenta. Placenta. 1999 Jan;20(1):13-9.
410. Kivlighan KT, DiPietro JA, Costigan KA, Laudenslager ML. Diurnal rhythm
of cortisol during late pregnancy: associations with maternal psychological
well-being and fetal growth. Psychoneuroendocrinology. 2008 Oct;33(9):
1225-35.
411. Nkansah-Amankra S, Luchok KJ, Hussey JR, Watkins K, Liu X. Effects of
maternal stress on low birth weight and preterm birth outcomes across
neighborhoods of South Carolina, 2000-2003. Matern Child Health J. 2010
Mar;14(2):215-26.
412. Precht DH, Andersen PK, Olsen J. Severe life events and impaired fetal
growth: a nation-wide study with complete follow-up. Acta Obstet Gynecol
Scand. 2007;86(3):266-75.
413. Glynn LM, Wadhwa PD, Dunkel-Schetter C, Chicz-Demet A, Sandman CA.
When stress happens matters: effects of earthquake timing on stress
responsivity in pregnancy. Am J Obstet Gynecol. 2001 Mar;184(4):637-42.
414. Zhu P, Tao F, Hao J, Sun Y, Jiang X. Prenatal life events stress: implications
for preterm birth and infant birthweight. Am J Obstet Gynecol. 2010
Jul;203(1):34 e1-8.
415. Holmes MC, Seckl JR. The role of 11beta-hydroxysteroid dehydrogenases in
the brain. Mol Cell Endocrinol. 2006 Mar 27;248(1-2):9-14.
416. Hobel CJ, Dunkel-Schetter C, Roesch SC, Castro LC, Arora CP. Maternal
plasma corticotropin-releasing hormone associated with stress at 20 weeks'
gestation in pregnancies ending in preterm delivery. Am J Obstet Gynecol.
1999 Jan;180(1 Pt 3):S257-63.
126
417. Diego MA, Field T, Hernandez-Reif M, Schanberg S, Kuhn C, GonzalezQuintero VH. Prenatal depression restricts fetal growth. Early Hum Dev.
2009 Jan;85(1):65-70.
418. Field T, Hernandez-Reif M, Diego M, Figueiredo B, Schanberg S, Kuhn C.
Prenatal cortisol, prematurity and low birthweight. Infant Behav Dev. 2006
Apr;29(2):268-75.
419. Diego MA, Jones NA, Field T, Hernandez-Reif M, Schanberg S, Kuhn C, et
al. Maternal psychological distress, prenatal cortisol, and fetal weight.
Psychosom Med. 2006 Sep-Oct;68(5):747-53.
420. Goedhart G, Vrijkotte TG, Roseboom TJ, van der Wal MF, Cuijpers P,
Bonsel GJ. Maternal cortisol and offspring birthweight: results from a large
prospective cohort study. Psychoneuroendocrinology. 2010 Jun;35(5):644-52.
421. Abeysena C, Jayawardana P, Seneviratne Rde A. Effect of psychosocial stress
and physical activity on low birthweight: a cohort study. J Obstet Gynaecol
Res. 2010 Apr;36(2):296-303.
422. Stein A, Campbell EA, Day A, McPherson K, Cooper PJ. Social adversity,
low birth weight, and preterm delivery. Br Med J (Clin Res Ed). 1987 Aug
1;295(6593):291-3.
423. Newton RW, Hunt LP. Psychosocial stress in pregnancy and its relation to
low birth weight. Br Med J (Clin Res Ed). 1984 Apr 21;288(6425):1191-4.
424. Petrou S. Economic consequences of preterm birth and low birthweight.
BJOG. 2003 Apr;110 Suppl 20:17-23.
425. Tuntiseranee P, Olsen J, Chongsuvivatwong V, Limbutara S. Socioeconomic
and work related determinants of pregnancy outcome in southern Thailand. J
Epidemiol Community Health. 1999 Oct;53(10):624-9.
426. Rosellini AJ, Brown TA. The NEO Five-Factor Inventory: Latent Structure
and Relationships With Dimensions of Anxiety and Depressive Disorders in a
Large Clinical Sample. Assessment. 2010 Sep 29.
427. Krantz DS, Hedges SM. Some cautions for research on personality and
health. J Pers. 1987 Jun;55(2):351-7.
127
PUBLICATIONS ON THE DISSERTATION THEME
1. Mockutė I, Švedas E, Raškauskienė N, Mickuvienė N, Pop VJ,
Bunevičius R. Thyroid function tests during pregnancy: a longitudinal
study in the area of compensated mild iodine deficiency. Acta
Obstetricia et gynecologica Scandinavica. 2011. In press under revision.
2. Mockutė, Ingrida; Raškauskienė, Nijolė; Kusminskas, Laima; Švedas,
Eimantas. Iodine deficiency assessed by the newborn thyrotropin
concentration = Jodo stygiaus įvertinimas pagal naujagimių tireotropinio
hormono kiekį // Lietuvos akušerija ir ginekologija = Lithuanian
obstetrics & gynecology 2010, t. 13, Nr. 2, p. 131–136.
3. Mockutė, Ingrida; Švedas, Eimantas; Raškauskienė, Nijolė; Mickuvienė,
Narseta; Bunevičius, Robertas. The newborn thyroid stimulating
hormone levels in relation to maternal age and gestation at birth =
Naujagimio tirostimuliuojančio hormono ryšys su motinos amžiumi bei
nėštumo trukme // Lietuvos akušerija ir ginekologija = Lithuanian
obstetrics & gynecology 2010, t. 13, Nr. 3, p. 278–284.
4. Bunevičius A, Čėsnaitė E, Mockutė I, Kusminskas L, Bunevičius R. Antenatal maternal mental state and anthropometric characteristics of the
newborns: I. Impact of symptoms of depression and anxiety. Biologinė
psichiatrija ir psichofarmakologija 2007;9(1):3–6.
5. Bunevičius A, Kusminskas L, Mockutė I, Bunevičius R Antenatal maternal state and anthropometric characteristics of the newborns: II. Impact of personality dimensions and stress. Biologinė psichiatrija ir
psichofarmakologija 2007;9(2):35–38
128
ANNEXES
Annexe 1
PERMIT FROM BIOETHICS COMMITTEE
129
Annexe 2
130
Annexe 3
131
Annexe 4
132
Annexe 5
Spilbergerio STAI–Trait skalė
Perskaitykite žemiau išvardintus teiginius ir pažymėkite Jums
tinkamiausią atsakymą (skaičių atsakymų grafoje). Teisingų ar neteisingų
atsakymų nėra, todėl ties kiekvienu teiginiu ilgai negalvokite.
Eil.
Nr.
Atsakymas
Teiginys
2
3
Beveik
visada
4
1
2
3
4
Aš lengvai apsiverkiu
1
2
3
4
1
2
3
4
1
2
3
4
1
2
3
4
1
2
3
4
8.
Aš noriu būti toks laimingas (-a) kaip kiti
Būna, kad aš pralaimiu todėl, kad negaliu
greitai apsispręsti
Aš jaučiuosi žvalus (-i)
Aš ramus (-i), šaltakraujiškas (-a), susikaupęs
(-usi)
Sunkumų laukimas man kelia nerimą
1
2
3
4
9.
Aš per daug pergyvenu dėl smulkmenų
1
2
3
4
10
Aš visai laimingas (-a)
1
2
3
4
11
Aš per daug viską imu į širdį
1
2
3
4
1
2
3
4
Aš jaučiuosi saugiai
Aš stengiuosi išvengti sunkumų ir kritiškų
situacijų
Mane apima slogi nuotaika – būnu paniuręs
(-usi)
Aš būnu patenkintas (-a)
1
2
3
4
1
2
3
4
1
2
3
4
1
2
3
4
Visokios smulkmenos blaško ir jaudina mane
Aš taip sunkiai pergyvenu nusivylimus, kad
po to negaliu jų pamiršti
Aš ramus, susitvardantis žmogus
Mane apima sunkus nerimas, kai aš galvoju
apie savo reikalus ir rūpesčius
1
2
3
4
1
2
3
4
1
2
3
4
1
2
3
4
1.
Aš jaučiu pasitenkinimą
2.
Aš greitai pavargstu
3.
4.
5.
6.
7.
Labai
retai
1
12. Man trūksta pasitikėjimo savimi
13
14
15
16
17
18
19
20
133
Kartais Dažnai
Annexe 6
The Big Five Personality Test
Nurodymai: žemiau yra nurodytos kai kurios savybės, kurios jums gali būti būdingos arba nebūdingos. Pavyzdžiui, ar sutiktumėte su teiginiu, kad esate žmogus
mėgstantis leisti laiką su kitais žmonėmis? Prašome prie kiekvieno teiginio parašyti
skaičių nurodantį, kuria dalimi sutinkate ar nesutinkate su tuo teiginiu.
1 – Visiškai nesutinku
2 – Iš dalies nesutinku
3 – Nei sutinku, nei nesutinku
4 – Iš dalies sutinku
5 – Visiškai sutinku
Manau, kad esu...
________ 1. Kalbus(-i).
________ 2. Linkęs(-usi) ieškoti kitų kaltės.
________ 3. Kruopštus.
________ 4. Prislėgtas(-a), liūdnas(-a).
________ 5. Originalus(-i), turintis(-i) naujų idėjų.
________ 6. Santūrus(-i).
________ 7. Paslaugus(-i) ir nesavanaudiškas(-a).
________ 8. Kartais kiek nerūpestingas(-a).
________ 9. Atsipalaidavęs(-usi), lengvai susitvarkantis(-i) su stresu.
________10. Besidomintis(-i) daugeliu įvairiausių dalykų.
________11. Pilnas(-a) energijos.
________12. Žmogus, kuris pradeda ginčus su kitais.
________13. Patikimas(-a) darbuotojas(-a).
________14. Kartais galiu būti įsitempęs(-usi).
________15. Išradingas(-a), giliai mąstantis(-i).
________16. Entuziastingas(-a).
________17. Atlaidus(-i).
________18. Dažnai netvarkingas(-a).
134
________19. Daug nerimaujantis(-i).
________20. Turintis(-i) turtingą vaizduotę.
________21. Linkęs(-usi) būti tylus(-i).
________22. Paprastai pasitikintis(-i) žmonėmis.
_______23. Linkęs(-usi) į tinginystę.
_______24. Emociškai stabilus(-i), nelengvai nuliūdinamas(-a).
_______25. Kūrybingas(-a).
_______26. Ryžtingas(-a).
_______27. Galiu būti šaltas(-a) ir abejingas(-a).
_______28. Atkakliai siekiantis(-i) užbaigti pradėtą darbą.
_______29. Mano nuotaikos gali greitai keistis.
_______30. Vertinantis(-i) meninius, estetinius išgyvenimus.
_______31. Kartais drovus(-i) ir suvaržytas(-a).
_______32. Atidus(-i) ir malonus(-i) beveik visiems.
_______33. Savo darbus dirbu efektyviai.
_______34. Įtemptose situacijose išlieku ramus(-i).
_______35. Teikiu pirmenybę pagal nusistovėjusią tvarką atliekamam darbui.
_______36. Draugiškas(-a) ir mėgstantis(-i) bendrauti.
_______37. Kartais grubiai kalbu su kitais.
_______38. Kuriu planus ir juos įvykdau.
_______39. Lengvai susinervinantis.
_______40. Mėgstu galvoti, žaisti idėjomis.
_______41. Turiu keletą meninių pomėgių.
_______42. Mėgstu bendradarbiauti su kitais.
_______43. Mano dėmesys lengvai nukrypsta į šalį.
_______44. Turiu subtilų meninį, muzikinį ir literatūrinį skonį.
135