Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Artificial gene synthesis wikipedia , lookup
Primary transcript wikipedia , lookup
Long non-coding RNA wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Gene expression profiling wikipedia , lookup
Polycomb Group Proteins and Cancer wikipedia , lookup
Epigenetics of diabetes Type 2 wikipedia , lookup
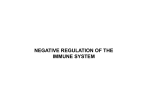
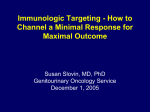
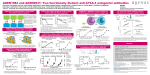
Genes and Immunity (2001) 2, 145–152 2001 Nature Publishing Group All rights reserved 1466-4879/01 $15.00 www.nature.com/gene CTLA-4 gene expression is influenced by promoter and exon 1 polymorphisms A Ligers1,2, N Teleshova1, T Masterman1, W-X Huang1 and J Hillert1 1 Division of Neurology, NEUROTEC, Karolinska Institutet at Huddinge University Hospital, Stockholm, Sweden; 2Center of Biotechnology, Department of Bioscience, NOVUM, Karolinska Institutet, Stockholm, Sweden CTLA-4, expressed mainly on activated T cells, helps maintain, through its inhibitory function, immune-system homeostasis. Polymorphisms in the CTLA-4 gene (CTLA4) are known to be important in several autoimmune diseases, including multiple sclerosis (MS). Here, we have performed genotyping for CTLA4 polymorphisms, and investigated expression by peripheral blood mononuclear cells of CTLA-4 mRNA and protein, in patients with MS and myasthenia gravis and in healthy controls. Expression levels for mRNA and protein were similar in the patient and control groups; however, there was a clear relationship between genotype and CTLA-4 expression. Specifically, individuals carrying thymine at position −318 of the CTLA4 promoter (T−318) and homozygous for adenine at position 49 in exon 1 showed significantly increased expression both of cell-surface CTLA-4 after cellular stimulation and of CTLA-4 mRNA in nonstimulated cells. The association was seen most clearly for unsorted CD3+ cells and was absent in the CD8+ subset. The T−318 allele has been shown to be negatively associated with susceptibility to MS in an earlier study by our group. Thus, we propose that the susceptibility-influencing role of CTLA4 in MS may be related to genotypically conditioned promoter function, whereby high gene expression may decrease the risk of disease. Genes and Immunity (2001) 2, 145–152. Keywords: CTLA-4; gene expression; multiple sclerosis; polymorphism Introduction Multiple sclerosis (MS) is believed to be an autoimmune disease resulting from aberrant immune responses to central nervous system (CNS) antigens, and T cells are thought to be involved in its pathogenesis. In the CNS, organ-specific T cells mediate tissue damage by activating effector immune cells and by regulating recruitment of non-antigen-specific lymphocytes and monocytes to MS lesions.1 Naı̈ve T cells require two signals to proliferate and differentiate. Signal one is antigen-specific and is generated by interaction of the T-cell receptor (TCR) with an antigenic peptide presented on an MHC molecule. Signal two, essential for a functional response in T cells, is transduced most commonly through interaction of CD28 on the T cell with B7 on the antigen-presenting cell. Expression of cytotoxic T lymphocyte-associated molecule4 (CTLA-4) is subsequently up-regulated on T cells activated in this manner. CTLA-4 also binds B7, but this interaction results in down-regulation of the ongoing immune response.2–4 Correspondence: Arturs Ligers, Division of Neurology, NEUROTEC, Karolinska Institutet at Huddinge University Hospital R54, S-141 86 Stockholm, Sweden. E-mail: Arturs.Ligers얀neurotec.ki.se This study was supported by grants from the Swedish Medical Research Council (project numbers 11023 and 11220), the Society for the Neurologically Disabled, the Sigurd and Elsa Goljes Minne Foundation, Karolinska Institutet, the Magn. Bergvall Foundation, the Åke Wiberg Foundation, the Bibbi and Nils Jensen Foundation and the Marcus Borgström Foundation. Received 19 December 2000; revised and accepted 1 March 2001 CTLA-4 was first identified through the screening of a murine cytolytic T-cell cDNA library,5 and the gene encoding the molecule is in humans located on chromosome 2q33-q34, 25–150 kilobases from the CD28 gene, with which it shares extensive sequence homology.6 Expression of CTLA-4 is mainly restricted to CD4+ and CD8+ activated T-lymphocyte subsets,7 but has also been reported on B cells.8 The human CTLA-4 gene (CTLA4) is known to contain polymorphisms in three regions: a cytosine-thymine singlebase substitution in the promoter at position −318 (C−318/T−318), and adenine-guanine dimorphism in the exon 1 leader sequence at position 49 (A49/G49), an a multiallelic dinucleotide repeat in the 3′ untranslated region (UTR) of exon 4 (Figure 1). These three polymorphisms have been investigated for linkage and association in a number of human autoimmune diseases. The G49 allele has been shown to be associated with several organ-specific autoimmune diseases, including type I diabetes mellitus (association with the G49 allele and microsatellite 102 bp allele),9,10 Graves’ disease (association with microsatellite 102 bp allele)11 and MS (association with T−318 allele (negative) and G49 allele)12,13; but results are less clear with regard to the non-organ-specific disease systemic lupus erythematosus (SLE) (lack of association with T−318/C−318 alleles)14 or rheumatoid arthritis (RA) (association with G49 allele after stratification for HLA class II alleles).15 Little is known about the functional involvement of CTLA-4 in human diseases—partly due to the fact that detection of the CTLA-4 protein on non-stimulated cells is difficult due to low density of expression. Previous studies have employed in situ expression, flow cytometry CTLA4 polymorphisms and gene expression A Ligers et al 146 Results CTLA-4 promoter region, exon 1 and exon 4 polymorphisms Five genotypes were identified for the promoter-exon 1 region and 12 alleles for the dinucleotide repeat in exon 4. Of the 72 individuals typed, none was homozygous for T−318; nor did we observe any instance of T−318 occurring on the same chromosome as G49. Precise genotypes counts for MS patients and controls are shown in Table 1. Figure 1 Schematic representation of known polymorphic sites within the CTLA-4 gene (CTLA4): aT/C (thymine/cytosine) dimorphism of the CTLA4 promoter region, located at position –318 from ATG start codon. bA49/G49 (adenine/guanine) dimorphism of the leader sequence of exon 1, located at position 49 from the ATG start codon. c(AT) dinucleotide-repeat sequence, located in the 3′ untranslated region of exon 4. Distance between exon 1 polymorphism and dinucleotide repeat at exon 4 is 5421 bp. The segments represented are not to scale. or reverse transcriptase (RT) PCR methods for detection of CTLA-4 protein or mRNA levels. Expression of CTLA-4 appears to be selectively induced in certain pathological conditions in vivo,16 but the mechanism underlying this induction is unknown. SLE patients were found to have higher expression of CTLA-4 on T cells compared with normal controls, but after cell stimulation, expression levels became similar.17 In patients with RA, increased levels of CTLA-4-positive T cells were observed in synovial fluids and synovial membranes; addition of anti-CTLA-4 antibody led to increased production of TNF-␣ and IL-1, suggesting that CTLA-4 expression plays a down-regulatory role in rheumatoid articular inflammation.18 Mena et al19 found no difference in CTLA-4 expression between IFN-treated and untreated MS patients. The complexity of CTLA-4’s role in cell activation was recently underscored by the identification of a soluble form of the molecule, generated by alternative splicing of the primary transcript. In humans, the soluble form has been shown to be produced by B cells and nonstimulated T cells of both the CD4+ and CD8+ phenotypes; it has been detected in mice and rats as well.20,21 Thus, it appears that the CTLA-4 molecule may be constitutively produced in a soluble form that regulates immune homeostasis by blocking B7 family receptors during both early and late stages of the immune response. Because CTLA-4 appears to be a negative regulator of the normal immune response, it is of interest to investigate whether altered expression of CTLA-4 on T cells may contribute to the impaired immune response seen in MS. The aims of this study were as follows: to measure and compare CTLA-4 mRNA and protein levels in patients with MS and myasthenia gravis (MG) and in healthy controls; to determine whether three well-characterized CTLA4 polymorphisms modulate protein and mRNA levels in these groups; and to analyze CTLA-4 protein levels in different cell populations. Genes and Immunity Flow cytometry analysis Repeated analysis by flow cytometry on unstimulated cells showed that expression of CTLA-4 protein was low intracellularly and undetectable on the cell surface. Therefore, cells used for flow-cytometry analysis were later subjected to mitogen-induced stimulation with ConA (see Materials and methods). For CTLA-4 protein expression, no differences were found between MS patients receiving immunosuppressive therapy and untreated patients (data not shown); treated and untreated MS patient groups were therefore combined for subsequent analysis. In both patients and controls, the number of cells expressing CTLA-4 intracellularly was higher than the number expressing CTLA-4 on the cell surface. When MS patients were compared to controls, no differences were found in intracellular or cell-surface CTLA-4 protein expression in unsorted peripheral blood mononuclear cells (PBMCs) or in any T-cell subpopulation. In addition, Table 1 Distribution of CTLA4 genotypes among MS patients and controls. Allele-specific PCR with simultaneous amplification of dimorphisms at positions −318 and 49 allowed identification of the following promoter-exon 1 ‘haplotypes’: C-A (haplotype 1), C-G (haplotype 2), T-A (haplotype 3); exon 4 dinucleotide-repeat alleles are designated by their length in base-pairs. No significant differences in the distribution of alleles, ‘haplotypes’ or genotypes were observed Promoter-exon 1 1,1 1,2 1,2 1,2 1,2 1,2 1,2 1,2 2,2 2,2 2,2 2,2 2,2 2,2 2,2 2,2 2,2 1,3 1,3 1,3 2,3 2,3 2,3 2,3 Exon 4 (AT)n Patients (ntot = 38) Controls (ntot = 34) 84/84 84/84 84/102 84/104 120/120 104/124 102/106 102/120 102/102 110/120 84/84 84/102 100/104 102/114 84/110 110/110 102/118 118/118 84/84 84/94 84/84 102/118 102/102 130/130 3 2 8 3 1 1 1 0 5 2 1 2 1 0 0 0 0 1 3 1 1 1 1 0 2 5 7 0 0 0 0 1 6 0 0 0 0 1 1 1 1 1 6 0 0 0 1 1 CTLA4 polymorphisms and gene expression A Ligers et al Table 2 Median percentage (and interquartile range) of peripheral blood mononuclear cells expressing CTLA-4 on the cell surface in multiple sclerosis (MS) patients and controls stratified for genotype at promoter and exon 1 dimorphisms and exon 4 dinucleotide repeat MS (n = 38) Controls (n = 34) MS and controls (n = 72) Promoter T/C C/C 3.5 (2.1 to 6.8) 2.2 (1.8 to 4.5) 4.0 (2.9 to 27.0)a 1.7 (1.4 to 2.5) 4.0 (2.4 to 8.0)e 2.0 (1.4 to 3.0) Exon 1 A/A A/G G/G 3.1 (1.4 to 6.8) 2.3 (1.8 to 3.0) 2.6 (1.8 to 6.0) 5.2 (4.0 to 27.0)b,c 1.7 (1.5 to 3.0) 1.5 (1.1 to 2.0) 4.2 (2.0 to 8.0)f,g 2.1 (1.5 to 3.0) 2.0 (1.2 to 2.9) Exon 4 84/84 84/X X/X 2.0 (1.3 to 6.6) 2.9 (2.0 to 5.3) 2.5 (1.8 to 4.0) 4.2 (2.0 to 6.2)d 1.6 (1.5 to 2.3) 1.5 (1.2 to 2.9) 3.1 (1.7 to 6.6) 2.0 (1.5 to 3.7) 2.2 (1.4 to 3.0) T/C vs C/C, P ⬍ 0.01; bA/A vs A/G, P ⬍ 0.05; cA/A vs G/G, P ⬍ 0.01; d84/84 vs 84/X, P ⬍ 0.05; eT/C vs C/C, P ⬍ 0.01; fA/A vs A/G, P ⬍ 0.01; gA/A vs G/G, P ⬍ 0.05. a we found no significant differences between MS patients, MG patients and controls with regard to CTLA-4 mRNA levels. CTLA-4 polymorphisms and expression of CTLA-4 protein and mRNA When individuals were stratified by genotype at the promoter and exon 1 dimorphisms, significant differences in both cell-surface and mRNA expression of CTLA-4 were observed. Both in the control group and in MS patients and controls considered together, CTLA-4 cell-surface expression was significantly increased in individuals carrying T−318, compared to levels in individuals homozygous for C−318, and in A49 homozygotes, compared to levels in carriers of the A49/G49 or G49/G49 genotypes (Table 2). Both in MG patients, MS patients and controls considered together, CTLA-4 mRNA levels were significantly higher in PBMCs from subjects carrying T−318 than levels in cells from subjects lacking the allele (Table 3). For analysis of the influence of the exon 4 microsatellite alleles on CTLA-4 cell-surface expression, we subdivided individuals into three groups, with respect to the presence or absence of the 84 base-pair (bp) allele. Although expression was significantly higher in 84bp/84bp controls than in 84bp/Xbp controls, when controls and MS patients were analyzed together, no significant differences between the 84bp/84bp, 84bp/Xbp and Xbp/Xbp genotypes were found (Table 2). CTLA-4 genotypes and CTLA-4 protein expression Because alleles at position −318 (promoter) and 49 (exon 1) are in strong linkage disequilibrium with one another, it is relevant to analyze the effect of combined genotypes on CTLA-4 expression. Indeed, CTLA-4 cell-surface expression was significantly increased in carriers of T−318 homozygous for A49 (genotype 1/3), compared to levels in carriers of the remaining genotypes (Figure 2), for all cells (P = 0.0026), for unsorted CD3+ cells (P = 0.001) and, to a lesser extent, for CD4+ cells (P = 0.004). For CD8+ cells, the difference was not significant. 147 ANOVA of CTLA-4 polymorphisms and CTLA-4 protein expression To investigate whether either one of the three polymorphic sites was most important for the observed genotype effect on CTLA-4 expression, we performed one-way ANOVA (data not shown) and two-way ANOVA. We found a positive interaction between the promoter and exon 1 polymorphisms for CTLA-4 protein expression on PBNCs. Pair-wise mean difference analysis revealed that differences in numbers of CTLA-4-expressing cells were most pronounced when carriers of T−318 homozygous for A49 (genotype 1/3) were compared to subjects homozygous for C−318 carrying A49/G49 (genotype 1/3) or G49/G49 (genotype 2/2) (Table 4). There was no interaction between exon 4 alleles and promoter or exon 1 alleles. These results indicate that the T−318/C−318–A49/A49 Figure 2 Median values for cell-surface expression of CTLA-4 on peripheral blood mononuclear cells (PBMCs), as determined by flow cytometry, in patients and controls stratified according to genotype. C/C and T/C refer to the two genotypes observed at position −318 of the CTLA4 promoter sequence, whereas A/A, A/G and G/G refer to the three genotypes at position 49 of the first exon of CTLA4. Controls carrying the combined genotype T/C-A/A (genotype 1/3) had significantly higher expression of CTLA-4 on PBMCs than carriers of other genotypes (P = 0.022). No other differences were statistically significant. Table 3 CTLA-4 mRNA expression as determined by competitive reverse transcriptase PCR on unstimulated peripheral blood mononuclear cells from patients with multiple sclerosis (MS; n = 60) and myasthenia gravis (MG; n = 29) and controls (n = 26) stratified by genotype at position −318 in the CTLA4 promoter. Median values (and interquartile ranges) are given, expressed as (CTLA-4 mRNA/-actin mRNA) × 10−3 Genotype T/C C/C MS MG Controls All subjects 0.86 (0.64 to 1.05) (n = 12) 0.8 (0.4 to 1.2) (n = 48) 1.32 (0.84 to 6.45) (n = 4) 0.59 (0.34 to 1.06) (n = 25) 1.74 (0.73 to 2.10) (n = 6) 0.83 (0.47 to 1.23) (n = 20) 0.92 (0.75 to 1.75) (n = 22) 0.78 (0.41 to 1.19) (n = 93) P = NS P ⬍ 0.05 P = NS P ⬍ 0.05 NS, not significant at 5% level. Genes and Immunity CTLA4 polymorphisms and gene expression A Ligers et al 148 Table 4 Analysis of the relative importance for CTLA-4 cell-surface expression of genotypes for dimorphisms at positions −318 (T/C and C/C), and 49 (A/A, A/G and G/G) of CTLA4. Two-way ANOVA matrices (A), as well as pair-wise mean differences (B) with Bonferroni adjustments (C), are shown. The analysis reveals not only that the −318 T/C and 49 A/A genotypes are associated with increased CTLA-4 expression, but also that the simultaneous presence of both genotypes confers higher expression than each of the remaining combined genotypes Groups F-ratio P n A. T/C, C/C A/A, A/G T/C, C/C and A/A, A/G 4.427 3.228 5.087 0.041 0.079 0.029 70 50 50 Groups T/C–A/A T/C–A/G C/C–A/A C/C–A/G C/C–G/G B. T/C–A/A T/C–A/G C/C–A/A C/C–A/G C/C–G/G 0.000 −0.507a −1.621 −1.450 −1.544 0.000 −0.114 0.056 −0.037 0.000 0.171 0.077 0.000 −0.093 0.000 C. T/C–A/A T/C–A/G C/C–A/A C/C–A/G C/C–G/G 1.000 0.032b 0.0160 ⬍0.0005 ⬍0.0005 1.000 1.000 1.000 1.000 1.000 1.000 1.000 1.000 1.000 1.000 a Pair-wise mean differences; bP values. genotype (also expressed as 1/3) is the only genotype associated with increased expression of CTLA-4, and that differences in expression are related to the combined influence of the polymorphisms at positions −318 and 49. Discussion We have shown that cell-surface expression of CTLA-4 protein is influenced by common polymorphisms in the promoter and first-exon sequences. This influence is seen both in unsorted PBMCs, in unsorted CD3+ cells, and in the CD4+ T-cell subtype, but not in the CD8+ T-cell subtype. Furthermore, the effect seems to be related to at least two factors, one associated with position −318 in the promoter and the other with position 49 of the leader sequence. An increase in CTLA-4 mRNA levels was observed for individuals carrying T−318, thus lending additional support to the notion that CTLA-4 levels are influenced at the transcriptional stage in a genotype-dependent fashion. There are at present no reports suggesting that the position −318 polymorphism affects any known consensus sequence in the regulatory region of the CTLA4 promoter in humans. It has been shown, however, that the inducible expression of CTLA-4 detected during Tcell activation is controlled by this region in mice.22 The similarity of CTLA-4 cell-surface expression levels between MS patients and healthy controls regardless of genotype demonstrates that the variation in levels of protein expression is associated not with disease but rather with genotype. Indeed, its has been shown, that CTLA-4 exerts less profound inhibitory effects on proliferation for T cells carrying G49/G49 genotype rather than for cells Genes and Immunity carrying A49/A49 genotype, regardless of the presence of an autoimmune disease.23 We found no genotype-related difference in intracellular CTLA-4 protein expression. Moreover, the observed relationship between cell-surface expression of the CTLA-4 and specific genotypes was confined to unsorted cells and certain T-cell phenotypes. One explanation for this would be that mechanisms other than genotype contribute to the regulation of CTLA-4 cell-surface expression, and that these mechanisms are differentially operative in various T-cell subpopulations. Indeed, two recent studies have demonstrated the existence, in mice, of a subset of regulatory T cells whose immune-suppressive effects are dependent upon signaling via constitutively expressed CTLA-4.24,25 Genotype-conditioned regulation of CTLA-4 cellsurface expression could be explained by the presence of a functionally important variation in the molecule’s amino-acid sequence, possibly located in the Y201 motif of the cytoplasmic tail. This motif has been shown to be an important intracellular regulator of CTLA-4 protein levels through its interaction with the clathrin adaptor complexes AP-1 and AP-2, which mediate, respectively, degradation and endocytosis of the CTLA-4 protein.26,27 Our results show that individuals carrying T−318 express significantly higher levels of CTLA-4 mRNA, compared to C−318/C−318 subjects. Thus, differences in cell-surface expression may simply reflect a situation whereby newly synthesized CTLA-4 neither remains in Golgi or post-Golgi compartments, nor is stored in vesicles in the cytoplasm, but rather is transported directly to the cell surface. In fact, Alegre et al28 have by correlation of protein and mRNA levels demonstrated that Th2 cell clones express both CTLA-4 mRNA and cellsurface CTLA-4 protein at much higher levels than Th1 clones. These results seem to suggest that differential cellsurface expression of CTLA-4 is, at least in part, regulated by mRNA abundance. Data concerning expression of CTLA-4 differed between, on the one hand, all PBMCs, unsorted CD3+ cells and the CD4+ T-cell subsets, and, on the other, CD8+ T cells. CTLA-4 expression in the first three cell groups was clearly influenced by the gene’s polymorphic loci, whereas expression in CD8+ T cells was less genotypedependent. Mena et al19 have reported that, in the absence of stimulation, CD8+ cells exhibit higher levels of CTLA-4 expression than CD4+ cells in untreated MS patients and controls, but lower levels in MS patients undergoing immunosuppressive treatment. In contrast, our results for CTLA-4 expression in CD8+ cells did not differ greatly between groups of subjects. Discrepancies between our results and those of Mena et al19 may reflect the effects in different T-cell populations of treatment and cell stimulation on CTLA-4 expression, but it is unknown what the exact nature of such effects might be. It has been shown that mice depleted of CD8+ T cells from birth develop a lymphoproliferative disorder similar in onset and severity to that seen in unmanipulated CTLA-4−/− mice, whereas lymphoproliferation does not occur in CTLA-4−/− mice depleted of CD4+ T cells from birth.29 Moreover, results from experimental autoimmune encephalomyelitis experiments suggest that CD8+ cells may modulate the disease by eliminating CD4+ effector T cells through direct cytotoxicity.30 Thus, as these CTLA4 polymorphisms and gene expression A Ligers et al reports seem to indicate, CTLA-4 may have different effects in vivo on CD4+ and CD8+ T cells. Our data on CTLA-4 protein and mRNA levels in patients and controls seem to indicate that higher mRNA and protein levels are associated with a particular genotype and not affected with disease. However, this does not exclude the possibility that different CTLA-4 genotypes may be associated with different clinical forms of the same disease entity. Only a few studies evaluating the role of the position −318 polymorphism in autoimmune diseases have been published, and their results need clarification.13,14,31,32 One difficulty confronting future studies will be the low frequency of T−318—an allele that appears to be associated with protection from autoimmune disease—which may necessitate recruitment of considerable case-control or familial datasets for adequately powered analysis. Our expression data for all cells and for T cells of different phenotypes are consistent with the observation that T−318 frequency is lower among MS patients than controls: MS patients are less often carriers of an allele functionally associated with higher expression of a T cell down-regulatory protein. It would be difficult, however, to assess whether the T−318-associated increase of CTLA4 expression in certain T-cell subsets is sufficient to suppress an autoimmune process. The functional importance of the CTLA-4 gene has recently been evaluated. Ligation of CTLA-4 inhibits production of IL-2,33 while blockade of CTLA-4 increases production of IL-2, IFN-␥, IL-3 and TNF-␣ in Th1 cell clones, and of IL-3, IL-4, IL-5 and IL-10 in Th2 cell clones.28 Also, it has been shown that signaling via CTLA-4 can modulate production of TGF-34 and suppress production of TNF-␣ and IL-1;18 yet, CTLA-4knockout T cells can produce TGF- and IL-10.35 These findings support the notion of an inhibitory role for CTLA-4 and at the same time indicate that alternative down-regulatory immune pathways may exist. We did not find any significant associations between dinucleotide-repeat alleles and intracellular or cellsurface protein expression. Previous reports have suggested that autoimmune diseases are associated with longer CTLA-4 exon 4 microsatellite alleles and have cited, as an explanation for this, the observation that the length of AT repeats in the 3′ UTRs of transiently expressed genes may be inversely related to mRNA stability. However, this observed association between autoimmune diseases and longer microsatellite alleles can be better explained as a coincidence resulting from linkage disequilibrium between specific microsatellite, exon 1 and promoter alleles. Our data show similar levels of responsiveness to identical mitogen concentrations in PBMCs from MS patients and controls. Thus, there appears to be no defective expression of the CTLA-4 molecule in MS. CTLA-4 is a T cell activation marker and has inhibitory function on T cells; increased expression of CTLA-4 on PBMCs might contribute to the clinical improvement of MS by mediating anergy or apoptosis of T cells.36 Our results provide evidence that cell-surface and intracellular CTLA-4 expression levels are tightly regulated; that CD4+ and CD8+ cells may have different roles in down-regulation of ongoing immune response in MS; that the transcription rate of CTLA-4 gene and expression levels of the CTLA-4 protein are conditioned by specific genotypes, one of which, by increasing CTLA-4 expression, may decrease the risk of MS. 149 Materials and methods Patients and controls For flow cytometry analysis, 38 patients were diagnosed according to the recommendations of Poser et al37 as having clinical definite MS. At the time of blood sampling, 23 patients were receiving various immunosuppressive drug treatments. Thirty-four control specimens were obtained either from healthy medical students and hospital employees (n = 10) or from healthy blood donors (n = 24); control subjects were of the same ethnic background as patients. To support observations made by flow cytometry, we analyzed mRNA expression by competitive RT-PCR using cDNA specimens, collected for previous studies, from 60 MS patients,38 29 MG patients and 26 healthy controls,39 all different from the individuals studied for flow cytometry. At the time of blood sampling 11 MS patients and 13 MG patients were receiving immunosuppressive drug treatment. Control specimens were obtained from laboratory employees of the same ethnic background as patients. Non-overlapping groups of patients and controls were analyzed for protein and mRNA levels. MG patients were included particularly for mRNA analysis. PCR-SSP for detection of CTLA-4 promoter and exon 1 polymorphisms Genomic DNA was extracted from 5–10 ml venous blood by a modified salting-out protocol.40 The CTLA4 promoter and exon 1 polymorphisms were genotyped by PCR amplification with sequence-specific primers (PCRSSP); as the dimorphisms are separated by a mere 365 bases, it was possible to determine cis-located allele combinations by way of four haplotype-specific PCR amplifications for each subject. Primers were designed according to the published human CTLA-4 complementary DNA sequence (Genebank accession number M74363). Primer pair 5′ AGT CTC CAC TTA GTT ATC CAG ATC CTC and 3′ CAG GGC CAG GTC CTG GT amplified the C−318 – A49 haplotype. Primer pair 5′ AGT CTC CAC TTA GTT ATC CAG ATC CTC and 3′ CAG GGC CAG GTC CTG GC amplified the C−318 – G49 haplotype. Primer pair 5′ AGT CTC CAC TTA GTT ATC CAG ATC CTT and 3′ CAG GGC CAG GTC CTG GT amplified the T−318 – A49 haplotype. Primer pair 5′ AGT CTC CAC TTA GTT ATC CAG ATC CTT and 3′ CAG GGC CAG GTC CTG GC amplified the T−318 – G49 haplotype. Optimal PCR conditions consisted of an initial denaturation at 94°C for 2 min; followed by 10 cycles of denaturation at 94°C for 10 s and annealing at 65°C for 1 min; followed by 20 cycles of denaturation at 94°C for 10 s, annealing at 61°C for 50 s and elongation at 72°C for 30 s. After PCR thermal cycling (GeneAmp PCR System 9600; Perkin–Elmer, Norwalk, CT, USA), PCR reaction mixtures were loaded in 3 mm-wide slots in 2% (w/w) ME agarose gels prestained with ethidium bromide (0.5 g/ml gel) and were run for 25–30 min at 7–8 V/cm in 0.5 × TBE buffer (89 mM Tris base/89 mM boric acid/2 mM EDTA, ph 8.0) and gels were examined under UV illumination. Genes and Immunity CTLA4 polymorphisms and gene expression A Ligers et al 150 Microsatellite genotyping Individuals whose cells were to be analyzed by flow cytometry were genotyped for the microsatellite marker located in exon 4 (CTLA-4; http://cedar.genetics.soton. ac.uk/pub). Primers were synthesized by Scandinavian Gene Synthesis (Köping, Sweden), and the forward primer pair was labeled with 5′-HEX phosphoramidites. Primer pair sequences from 5′ to 3′ were HEX-GT GAT GCT AAA GGT TGT ATT GC and AAA ACA TAC GTG GCT CTA TGC AC. Optimal PCR conditions consisted of 35 cycles of denaturation at 95°C for 1 min, annealing at 55°C for 40 s and elongation at 72°C for 1 min. Genotyping was carried out on an Applied Biosystems 377 DNA automated sequencer using the semiautomated GeneScan/Genotyper software.41 For each sample, 1.5 l of diluted PCR product was combined with 0.5 l of internal size standard (GeneScan-350, PE Biosystems). The accuracy and reproducibility of automated sizing of fragments were confirmed by analysis in duplicate of randomly chosen samples. Competitive RT-PCR mRNA levels of CTLA-4 were quantified by a sensitive competitive RT-PCR method described by Huang et al38 The main principles for the method are the following: by combining varying amounts of target cDNA with a fixed amount of internal standard (double-stranded DNA for the same target gene), a linear standard curve is obtained; test samples are then co-amplified with the same amount of internal standard, and their amounts after amplification are calculated based on the quotient of the area- under-the-curve for target cDNA divided by that for the internal standard using the linear regression formula from the standard curve. To compensate for relative differences between samples, for the variable integrity of the individual RNA samples and for variations in reverse transcription, -actin cDNA was amplified and quantified for every test sample. PCR products were detected using an Applied Biosystems 377 DNA sequencer equipped with the GeneScan 2.02 software, and the results were analyzed using the Genotyper 1.1 software (PE Biosystems). Immunostaining and flow cytometry PBMCs were obtained from heparinized blood by a standard Ficoll-hypaque separation method. Cells were stimulated with Con-A (5 mg/ml) for 72 hrs. Fifty l of cell suspension (2 × 105 cells) was labeled with monoclonal antibodies (mAbs) conjugated with fluorescein isothiocyanate (FITC, green fluorescence), phycoerythrin (PE, orange fluorescence) or peridinin chlorophyll protein (PerCP, red fluorescence). All mAbs were titrated in preliminary experiments. Samples were incubated with mAb for 30 min at 4°C in the dark. The cells were washed twice with phosphate-buffered saline (PBS) containing 1% bovine serum albumin (BSA; Sigma, St Louis, MO, USA) and centrifuged at 2200 g for 10 min. To detect intracellular CTLA-4, cells were fixed with 4% paraformaldehyde, permeabilized with 0.1% saponin and stained with anti-CTLA-4 mAb intracellularly. Cells were washed twice with PBS containing 0.1% saponin, Figure 3 Fixed and permeabilised cells were preincubated with purified anti-CTLA-4 mAb (5 /106 for 30 min at 4°C). After incubation an anti-CTLA-4 FITC-labelled mAb was added to the cell suspension. Left part of the figures shows the percentages of CD3+ cells expressing CTLA-4 at the cell surface and CD3+ cells expressing CTLA-4 intracellularly. Right part of the figure shows the result of blocking experiment. Genes and Immunity CTLA4 polymorphisms and gene expression A Ligers et al resuspended in 250 l of 1% BSA/PBS and analyzed in a Becton Dickinson FACScan flow cytometer. Data analysis Flow cytometry data were processed using CellQuest software (Becton Dickinson). Combinations of anti-CD3, anti-CD4, anti-CD8 and anti-CTLA-4 mAbs were used to discriminate CTLA-4 positive T cells. Ten thousand events with light-scatter characteristics of mononuclear cells were saved for flow cytometry analysis with five parameters (forward scatter, reflecting cell size; side scatter, reflecting granularity; and intensity of FITC, PE and PerCP fluorescence). To define the precise gate, background staining (ie, the number of cells with fluorescence intensity over the defined level when stained with irrelevant mouse immunoglobulin G) was subtracted from each specific staining. A blocking experiment with unconjugated anti-CTLA-4 mAb was preformed to confirm staining specificity (Figure 3). Percent values presented are the fractions of the cell populations that stained for CTLA-4, eg, number of CD3+CTLA-4+ cells divided by the total number of CD3+ cells. Statistical analysis The Mann–Whitney U test was used to compare percentages of CTLA-4+ PBMC and CTLA-4 mRNA levels. Oneand two-way ANOVA and pair-wise mean differences were calculated from square-root values. The group carrying G49/G49 in exon 1 was excluded from two-way ANOVA analysis due to the absence in that group of subjects carrying C−318/T−318 or 84/84 in exon 4. Statistical calculations were performed using the Systat 9 program (SPSS Science, SPSS Inc, Chicago, IL, USA). Acknowledgments We thank Dr D Svensson and Dr J Krikis for statistical advice. References 1 Martino G, Hartung HP. Immunopathogenesis of multiple sclerosis: the role of T cells. Curr Opin Neurol 1999; 12: 309–321. 2 Karandikar NJ, Vanderlugt CL, Walunas TL, Miller SD, Bluestone JA. CTLA-4: a negative regulator of autoimmune disease. J Exp Med 1996; 184: 783–788. 3 Tivol EA, Borriello F, Schweitzer AN, Lynch WP, Bluestone AJ, Sharpe AH. Los of CTLA-4 leads to massive lymphoproliferation and fatal multiorgan tissue destruction, revealing a critical negative regulatory role of CTLA-4. Immunity 1995; 3: 541–547. 4 Carreno BM, Bennett F, Chau TA et al. CTLA-4 (CD152) can inhibit T cell activation by two different mechanisms depending on its level of cell surface expression. J Immunol 2000; 165: 1352–1356. 5 Brunet JF, Denizot F, Luciani MF, Roux-Dosseto M, Suzan M, Mattei MG. A new member of the immunoglobulin superfamily – CTLA-4. Nature 1987; 328: 267–270. 6 Harper K, Balzano C, Rouvier E, Mattei MG, Luciani MF, Golstein P. CTLA-4 and CD28 activated lymphocyte molecules are closely related in both mouse and human as to sequence, message expression, gene structure, and chromosomal location. J Immunol 1991; 147: 1037–1044. 7 Linsley PS, Greene JL, Tan P et al. Coexpression and functional cooperation of CTLA-4 and CD28 on activated T lymphocytes. J Exp Med 1992; 176: 1595–1604. 8 Kuiper HM, Brouwer M, Linsley PS, van Lier RA. Activated T cells can induce high levels of CTLA-4 expression on B cells. J Immunol 1995; 155: 1776–1783. 9 Donner H, Rau H, Walfish PG et al. CTLA-4 alanine-17 confers genetic susceptibility to Graves’ disease and to type 1 diabetes mellitus. J Clin Endocrinol Metab 1997; 82: 143–146. 10 Marron MP, Raffel LJ, Garchon HJ et al. Insulin-dependent diabetes mellitus (IDDM) is associated with CTLA4 polymorphisms in multiple ethnic groups. Hum Mol Genet 1997; 6: 1275–1282. 11 Yanagawa T, Hidaka Y, Guimaraes V, Soliman M, DeGroot LJ. CTLA-4 gene polymorphism associated with Graves’ disease in a Caucasian population. J Clin Endocrinol Metab 1995; 80: 41–45. 12 Ligers A, Xu C, Saarinen S, Hillert J, Olerup O. The CTLA-4 gene is associated with multiple sclerosis. J Neuroimmunol 1999; 97: 182–190. 13 Harbo HF, Celius EG, Vartdal F, Spurkland A. CTLA-4 promoter and exon 1 dimorphisms in multiple sclerosis. Tissue Antigens 1999; 53: 106–110. 14 Heward JM, Allahabadia A, Carr-Smith J et al. No evidence for allelic association of a human CTLA-4 promoter polymorphism with autoimmune thyroid disease in either population-based case-control or family-based studies. Clin Endocrinol 1998; 49: 331–334. 15 Seidl C, Donner H, Fischer B et al. CTLA4 codon 17 dimorphism in patients with rheumatoid arthritis. Tissue Antigens 1998; 51: 62–66. 16 Vandenborre K, Delabie J, Boogaerts MA et al. Human CTLA4 is expressed in situ on T lymhocytes in germinal centres, in cutaneous graft-versus host disease, and in Hodgkins disease. Am J Pathol 1998; 152: 963–973. 17 Liu MF, Liu HS, Wang CR, Lei HY. Expression of CTLA-4 molecule in peripheral blood T lymphocytes from patients with systemic lupus erythematosus. J Clin Immunol 1998; 18: 392–398. 18 Liu MF, Yang CY, Li JS, Lai KA, Chao SC, Lei HY. Increased expression of down-regulatory CTLA-4 molecule on T lymphocytes from rheumatoid synovial compartment. Scand J Immunol 1999; 50: 68–72. 19 Mena E, Rohowsky-Kochan C. Expression of costimulatory molecules on peripheral blood mononuclear cells in multiple sclerosis. Acta Neurol Scand 1999; 100: 92–96. 20 Magistrelli G, Jeannin P, Herbault N et al. A soluble form of CTLA-4 generated by alternative splicing is expressed by non stimulated human T cells. Eur J Immunol 1999; 29: 3596–3602. 21 Oaks MK, Hallett KM, Penwell RT, Stauber EC, Warren SJ, Tector AJ. A native soluble form of CTLA-4. Cell Immunol 2000; 201: 144–153. 22 Perkins D, Wang Z, Donovan C et al. Regulation of CTLA-4 expression during T cell activation. J Immunol 1996; 156: 4154– 4159. 23 Kouki T, Sawai Y, Gardine CA, Fisfalen ME, Alegre ML, DeGroot LJ. CTLA-4 gene polymorphism at position 49 in exon 1 reduces the inhibitory function of CTLA-4 and contributes to the pathogenesis of Graves’ disease. J Immunol 2000; 165: 6606–6611. 24 Takahashi T, Tagami T, Yamazaki S et al. Immunologic selftolerance maintained by CD25(+)CD4(+) regulatory T cells constitutively expressing cytotoxic T lymphocyte-associated antigen 4. J Exp Med 2000; 192: 303–310. 25 Read S, Malmstrom V, Powrie F. Cytotoxic T lymphocyteassociated antigen 4 plays an essential role in the function of CD25(+)CD4(+) regulatory cells that control intestinal inflammation. J Exp Med 2000; 192: 295–302. 26 Leung HT, Bradshaw J, Cleaveland JS, Linsley PS. Cytotoxic T lymphocyte-associated molecule-4, a high avidity receptor for CD80 and CD86, contains an intracellular localization motif in its cytoplasmic tail. J Biol Chem 1995; 270: 25107–25114. 27 Schneider H, Martin M, Agarraberes FA et al. Cytolytic T lymphocyte-associated antigen-4 and the TCR/CD3 complex, but not CD28, interact with clathrin adaptor complexes AP-1 and AP-2. J Immunol 1999; 163: 1868–1879. 28 Alegre ML, Shiels H, Thompson CB, Gajeuski TF. Expression and function of CTLA-4 in Th1 and Th2 cells. J Immunol 1998; 161: 3347–3356. 151 Genes and Immunity CTLA4 polymorphisms and gene expression A Ligers et al 152 29 Chambers CA, Kuhns MS, Allison JP. Cytotoxic T lymphocyte antigen-4 (CTLA-4) regulates primary and secondary peptidespecific CD4+ T cell responses. Proc Natl Acad Sci USA 1999; 96: 8603–8608. 30 Sun D, Ben-Nun A, Wekerle H. Regulatory circuits in autoimmunity: recruitment of counter-regulatory CD8+ T cells by encephalitogenic CD4+ T line cells. Eur J Immunol 1988; 18: 1993–1999. 31 Braun J, Donner H, Siegmund T, Walfish PG, Usadel KH, Badenhoop K. CTLA-4 promoter variants in patients with Graves’ disease and Hashimoto’s thyroiditis. Tissue Antigens 1998; 51: 563–566. 32 Park YJ, Chung HK, Park DJ et al. Polymorphism in the promoter and exon 1 of the cytotoxic T lymphocyte antigen-4 gene associated with autoimmune thyroid disease in Koreans. Thyroid 2000; 10: 453–459. 33 Krummel MF, Allison PJ. CTLA-4 engagement inhibits IL-2 accumulation and cell cycle progression upon activation of resting T cells. J Exp Med 1996; 183: 2533–2540. 34 Chen W, Jin W, Wahl SM. Engagement of cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) induces transforming growth factor- (TGF-) production by murine CD4(+) T cells. J Exp Med 1998; 188: 1849–1857. Genes and Immunity 35 Bachmann MF, Köhler G, Ecabert B, Mak TW, Kopf M. Cutting edge: lymphoproliferative disease in the absence of CTLA-4 is not T cell autonomous. J Immunol 1999; 163: 1128–1131. 36 Gribben JG, Freeman GJ, Boussiotis VA et al. CTLA4 mediates antigen-specific apoptosis of human T cells. Proc Natl Acad Sci USA 1995; 92: 811–815. 37 Poser CM, Paty DW, Scheinberg L et al. New diagnostic criteria for multiple sclerosis: guidelines for research protocols. Ann of Neurol 1983; 13: 227–231. 38 Huang W-X, Huang P, Link H, Hillert J. Cytokine analysis in multiple clerosis by competitive RT-PCR: A decreased expression of IL-10 and an increased expression of TNF-␣ in chronic progression. Mult Scler 1999; 5: 342–348. 39 Huang W-X, Huang P, Fredrikson S, Pirskanen R, Hillert J. Decreased mRNA expression of TNF-␣ and IL-10 in nonstimulated peripheral blood mononuclear cells in myasthenia gravis. Eur J Neurol 2000; 7: 195–202. 40 Olerup O, Aldener A, Fogdell A. HLA-DQB1 and -DQA1 typing by PCR amplification with sequence-specific primers (PCR-SSP) in 2 hours. Tissue Antigens 1993; 41: 119–134. 41 Reed PW, Davies JL, Copeman JB et al. Chromosome-specific microsatellite sets for fluorescence-based, semi-automatic genome mapping. Nat Genet 1994; 7: 390–395.