Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
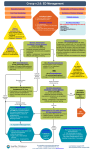
Ms Julia Bowey Head of Medicines Management Issue 126 Antidote Urgent treatment of Croup -consider oral corticosteroid treatment for all children, and a practice stock of soluble prednisolone for more severe cases. See local Map of Medicine for Croup (October 2012) for assistance in diagnosing and classifying the severity of croup on presentation (www.mapofmedicine.com). October 2012 “Tip of the Month” Mild Croup Consider a single dose of oral dexamethasone in children with mild croup -this reduces the proportion who re-present with croup in the following 7-10 days, compared with placebo. Dexamethasone dose for a child; 150 micrograms/kg body weight orally as a single dose: A 'typical' one-year-old weighing 10kg will require a dose of 1.5mg, which can be prescribed and administered as 3 x 500 microgram tablets Dexamethasone is also available as 2mg tablets for heavier children Dexamethasone tablets can be dispersed in water prior to administration (see the BNF for Children) Avoid prescribing the oral solution which is unlicensed and therefore not routinely stocked in community pharmacies (If parents/carers provide a good history of croup in the preceding 24 hrs but the child is now well, a dose of corticosteroid could be prescribed in case the child deteriorates again). Moderate or Severe Croup (see local Map of Medicine Croup pathway for clinical definitions) Give oral corticosteroid treatment (single dose) for all children with a diagnosis of moderate croup. If no corticosteroids are available, refer to the Emergency Department (ED). Severe croup requires urgent carriage to secondary care services. Consider soluble prednisolone. Dose for a child; 1-2mg/kg body weight orally as a single dose. Soluble prednisolone is available as 5mg tablets, which should meet all needs. Practices may wish to consider keeping a pot of these in stock to administer in moderate to severe cases, either instead of, or before, urgent transfer to hospital. For all groups, consider giving a second dose if residual symptoms are still present the following day. Drug Safety Update (MHRA) http://www.mhra.gov.uk//Safetyinformation/DrugSafetyUpdate/CON185627 Volume 6, Issue 2 (September 2012) Drug safety advice of particular relevance to primary care: Oseltamivir (Tamiflu): changed concentration and dosing dispenser of oral suspension from October 2012 From early October 2012, the strength of oseltamivir (Tamiflu) oral suspension will be 6 mg/mL. A new dosing dispenser, calibrated in mL, will be introduced at the same time. Dipeptidylpeptidase-4 inhibitors (‘gliptins’): risk of acute pancreatitis There have been reports of acute pancreatitis associated with drugs in the dipeptidylpeptidase-4 (DPP-4) inhibitor class of antidiabetic agents (‘gliptins’). Patients should be informed of the characteristic symptoms of acute pancreatitis – persistent, severe abdominal pain (sometimes radiating to the back) – and encouraged to tell their healthcare provider if they have such symptoms. Levofloxacin: some indications restricted Levofloxacin (a fluoroquinolone antibiotic) may only be considered in the treatment of acute bacterial sinusitis, acute exacerbation of chronic bronchitis, community acquired pneumonia or complicated skin and soft tissue infections when other medicines cannot be prescribed, or have been ineffective. Long Term Proton Pump Inhibitors (PPIs) and rare reports of hypomagnesaemia or risk of fracture http://www.mhra.gov.uk/Safetyinformation/DrugSafetyUpdate/CON149774 Further to the April edition of Antidote where we included the MHRA warnings on this, further local advice has been agreed as follows: Hypomagnesaemia Where possible use PPIs for no longer than one year continuously (e.g. use intermittently for symptom control at the lowest possible dose). Problems seem to be associated with long term use (>1 year). Over the counter PPIs should not be used for more than 4 weeks without medical advice. In anyone taking a long term PPI with a loop diuretic, thiazide or metalozone, in particular with digoxin, be extra vigilant of early warning signs of severe hypomagnesaemia and warn patients of possible insidious symptoms (e.g. fatigue, dizziness, loss of appetite, vomiting, muscle twitches or tremors) Measure magnesium if problems are suspected and seek advice from the CCG medicines management team with respect to correction with magnesium supplements if levels are very low. Discontinue the PPI if possible. Magnesium supplements are ‘special order’ products and as such should not be prescribed without the latest product advice from your CCG pharmacist. Fracture Risk Local Osteoporosis Guidelines have been updated to reflect MHRA guidance. PPI’s have been added to the list of medications associated with a (modest) risk of osteoporosis when used at high doses for longer than one year. Elderly patients may be particularly susceptible. Where possible use PPIs for no longer than one year continuously (e.g. use intermittently for symptom control at the lowest possible dose). Problems seem to be associated with long term use (>1 year) at high doses. Over the counter PPIs should not be used for more than 4 weeks without medical advice. Avoid PPIs where possible in patients with osteoporosis or with multiple risk factors, and ensure adequate calcium and vitamin D intake. Give advice on other lifestyle factors to reduce the risk of osteoporosis and/or fracture. The Map of Medicine now has over 100 local clinical pathways. Visit www.mapofmedicine.com to browse what is available locally (Southampton / South West Hampshire view). An NHS Athens password is required. The maps may be helpful both between and during consultations (as they contain patient information links), and for CPD, appraisals and revalidation purposes