Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
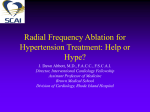
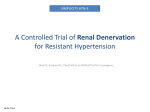
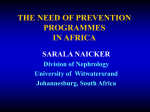
JACC: CARDIOVASCULAR INTERVENTIONS VOL. 5, NO. 3, 2012 © 2012 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION PUBLISHED BY ELSEVIER INC. ISSN 1936-8798/$36.00 DOI: 10.1016/j.jcin.2011.12.011 STATE-OF-THE-ART PAPER Renal Denervation for Hypertension Stefan C. Bertog, MD,*† Paul A. Sobotka, MD,‡§ Horst Sievert, MD* Frankfurt, Germany; Minneapolis, Minnesota; and Columbus, Ohio JACC: CARDIOVASCULAR INTERVENTIONS CME This article has been selected as this issue’s CME activity, available online at http://interventions.onlinejacc.org/ by selecting the CME tab on the top navigation bar. Accreditation and Designation Statement The American College of Cardiology Foundation (ACCF) is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. The ACCF designates this Journal-based CME activity for a maximum of 1 AMA PRA Category 1 Credit(s)™. Physicians should only claim credit commensurate with the extent of their participation in the activity. Method of Participation and Receipt of CME Certificate To obtain credit for this CME activity, you must: 1. Be an ACC member or JACC: Cardiovascular Interventions subscriber. 2. Carefully read the CME-designated article available online and in this issue of the journal. 3. Answer the post-test questions. At least 2 out of the 3 questions provided must be answered correctly to obtain CME credit. 4. Complete a brief evaluation. 5. Claim your CME credit and receive your certificate electronically by following the instructions given at the conclusion of the activity. CME Objective for This Article: After reading this article, the reader should understand the anatomy and physiology of the renal sympathetic nervous system and its role in blood pressure regulation, as well as the results of seminal experience with renal sympathetic denervation in animal models and humans. In addition, the reader will be up-to-date with recent experience using catheter-based renal denervation to treat essential hypertension and the potential use of this concept in conditions other than hypertension. CME Editor Disclosure: JACC: Cardiovascular Interventions CME Editor Habib Samady, MB, ChB, FACC, has research grants from the Wallace H. Coulter Foundation, Volcano Corp., St. Jude Medical, Forrest Pharmaceuticals Inc., and Pfizer Inc. Author Disclosure: Dr. Bertog has reported that he has no relationships relevant to the contents of this paper to disclose. Dr. Sobotka was chief medical officer of Ardian Inc. and is now an employee of Medtronic Inc. Prof. Sievert has received study honoraries, travel expenses, and consulting fees from Medtronic Inc. Medium of Participation: Print (article only); online (article and quiz). CME Term of Approval: Issue Date: March 2012 Expiration Date: February 28, 2013 From the *Cardiovascular Center Frankfurt, Frankfurt, Germany; †Department of Cardiology, Veterans Affairs Medical Center, Minneapolis, Minnesota; ‡Medtronic Inc., Minneapolis, Minnesota; and the §Ohio State University, Columbus, Ohio. Dr. Bertog has reported that he has no relationships relevant to the contents of this paper to disclose. Dr. Sobotka was chief medical officer of Ardian Inc. and is now an employee of Medtronic Inc. Prof. Sievert has received study honoraries, travel expenses, and consulting fees from Medtronic Inc. Manuscript received September 21, 2011; revised manuscript received November 28, 2011, accepted December 8, 2011. 250 Bertog et al. Renal Denervation for Hypertension JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 5, NO. 3, 2012 MARCH 2012:249 –58 Renal Denervation for Hypertension Systemic hypertension is a major burden to the individual and society. Its association with major adverse cardiac and cerebral events and favorable effects of antihypertensive therapy are undisputed. However, despite multidrug therapy, blood pressures are frequently suboptimally controlled. Moreover, adverse drug effects often interfere with patients’ lifestyles and affect compliance. Therefore, alternative treatment strategies have been explored. Most recently, attention has been redirected to the sympathetic nervous system (SNS) in the pathogenesis of hypertension. In addition, interruption of the renal SNS in humans with resistant hypertension has been studied with promising results. The following review provides an overview of the anatomy and physiology of the renal SNS, the rational for manipulating the SNS, and the results of therapeutic renal sympathetic denervation. (J Am Coll Cardiol Intv 2012;5:249 –58) © 2012 by the American College of Cardiology Foundation The profound effect of systemic hypertension on the individual and society and beneficial effects of antihypertensive therapy are no longer questioned. However, frequently, despite treatment, blood pressures remain suboptimally controlled. This, in addition to unwanted side effects of antihypertensive medications, has stimulated exploration of alternative treatment modalities. Most recently, attention has been redirected to the renal sympathetic nervous system (SNS) in the pathogenesis of systemic hypertension and to its successful interruption with catheter-based radiofrequency application. The important role of the SNS in hypertension has been explored by measurement of its activity in hypertensive subjects as well as by examination of blood pressure changes after manipulation of sympathetic activity. Though not universal, higher levels of catecholamines are found in hypertensive individuals (1) and in those with borderline hypertension (2). Likewise, an increase in renal (3), cardiac (3–5) and skeletal muscle SNS activity (2,5) has been described in hypertensive patients. In patients with severe hypertension, a direct relationship between blood pressure and sympathetic activity has been reported (6). Perhaps the most striking evidence in support of a dominant role of the SNS in human blood pressure control is the effect of surgical sympathectomy (more or less extensive removal of sympathetic ganglia depending on the technique used). Though it has never been compared with no therapy or medical therapy in a controlled or randomized fashion, a profound improvement in blood pressure control was demonstrated in most studies (7,8). In addition, a reduction in cardiac size (8,9), improvement in renal function (8 –10) and lower incidences of headaches (10), precordial pain (10), and cerebrovascular (10) events were reported. Moreover, several studies suggested a reduction in mortality compared to an uncontrolled group of medically treated patients (11–13). These beneficial effects were counterbalanced by significant operative morbidity and mortality and unwanted side effects that, together with the advent of more effective antihypertensive medications, led to abandonment of this procedure in the early 1970s. Nonetheless, the experience lends undisputable support to the important role of the SNS in blood pressure control and confirms that a favorable blood pressure response can be achieved by a reduction in sympathetic tone. Focusing now on the more targeted disruption of the renal SNS, most experience stems from observations made in patients with renal insufficiency undergoing nephrectomy or renal transplantation and animal models of renal sympathectomy. The impact of the renal SNS on blood pressure control is well recognized in patients with kidney disease. Overactivity of the SNS has been demonstrated in patients with endstage renal disease requiring dialysis, with normalization after bilateral nephrectomy (14). Even if uremic toxins are removed after kidney transplantation, sympathetic overactivity persists in patients whose native diseased kidneys are not removed (15), lending support to the notion that the diseased kidneys account for the increased sympathetic activity. Removal of a diseased kidney (e.g., for pyelonephritis or congenital hypoplasia) in patients with hypertension can lead to blood pressure normalization (16 –18). Likewise, bilateral nephrectomy of native kidneys in patients with end-stage renal disease and kidney transplants has been shown to improve or normalize blood pressures (19,20). Though renin levels in patients with end-stage renal disease are frequently elevated and thus overactivity of the renin-angiotensin system may contribute to hypertension, there is ample evidence that overactivity of the afferent sympathetic nervous signals is at least as important as renin release is in the genesis and maintenance of hypertension, as well as in the improvement after nephrectomy. For example, it has been shown that beta-blocker therapy in kidney transplant patients is only effective in patients whose native kidneys have not been removed (21). Further, inhibition of JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 5, NO. 3, 2012 MARCH 2012:249 –58 the renin-angiotensin system has a modest effect on muscle sympathetic nervous activity and blood pressure control in patients with end-stage kidney disease, yet, administration of the central sympatholytic agent, clonidine, has a substantial blood pressure–lowering effect (22). It is not clear what triggers the increased activity of renal afferent sympathetic nerves. However, renal ischemia may be the cause or at least a contributor. To this effect, in patients with ischemia caused by renal artery stenosis, normalization of muscle sympathetic activity has been demonstrated after renal artery angioplasty (23). Similarly, blood pressure normalization after unilateral nephrectomy in patients with renal artery stenosis has been reported (24). A complete summary of animal data relevant to the topic of renal denervation surpasses the limits of this review. However, 3 animal experiments merit discussion. In spontaneously hypertensive rats whose renal sympathetic activity is increased, the development of hypertension is delayed and the severity is attenuated by prior bilateral renal sympathetic denervation (25). In animals undergoing bilateral nephrectomy and autoreimplantation of their kidneys, any sympathetic influences to and from the kidney are disrupted. This has been shown to result in significant diuresis (26). Though the mechanism and long-term effects have been disputed, a readjustment of the pressure natriuresis response is plausible. Lastly, in dogs, stimulation of renal sympathetic nerves causes hypertension (27). Of note, this does not appear to be related solely to a reduction in renal blood flow, as this parameter changes little with chronic renal sympathetic stimulation (27). In conclusion, human experience and animal experiments unequivocally support not only an important role of the SNS in blood pressure regulation, but also a beneficial blood pressure response to the interruption of the renal SNS. Anatomy and Physiology of the Renal SNS The renal SNS affects blood pressure by 2 pathways (Fig. 1). It supplies the kidneys by a rich network of efferent, exclusively noradrenergic, sympathetic fibers located in the adventitia of the renal arteries and returns signals to the central nervous system via afferent sympathetic fibers likewise located in the adventitia. Autonomic centers in the medulla oblongata and midbrain receive and integrate afferent signals from end organ sensors and baroreceptors as well as from the hypothalamus, cortex, and limbic system and transmit efferent signals to sympathetic pre-ganglionic neurons in the intermediolateral column of the spinal cord. Fibers from neurons in the intermediolateral column (T10 to T12, L1 to L2) extend via splanchnic nerves to post-ganglionic neurons located in pre-vertebral ganglia. Post-ganglionic neurons reach the kidney via the adventitia of the renal arteries. Efferent Bertog et al. Renal Denervation for Hypertension 251 sympathetic fibers supply every aspect of the kidney, including the renal tubular cells (28), juxtaglomerular apparatus (29), and vasculature (30,31). Stimulation of efferent fibers causes activation of the adluminal basolateral Na/K adenosine triphosphatases (32), thereby promoting sodium and water retention, renin secretion via the juxtaglomerular apparatus (33), and vasoconstriction of renal arterioles. Hence, the efferent renal SNS will raise the goal blood pressure by a direct effect on the kidney promoting salt and water retention. Further, renin release stimulates the production of angiotensin II and thereby mineralocorticoids, mediating vasoconstriction and sodium and water retention, respectively. There appears to be a graded response depending on the intensity of the sympathetic signal, such that with low frequency stimulation renin secretion is first affected, followed by tubular sodium reabsorption and renal vascular tone at higher frequencies (34). In addition, and often underappreciated, the kidney transmits signals via afferent sympathetic fibers, the cell bodies of which are located in the dorsal root ganglia, to neurons of the posterior gray column of the ipsilateral spinal cord (35,36), from where signals are further relayed to autonomic centers in the central nervous system as well as to the contralateral kidney. The afferent fiber endings are found in all parts of the kidney; Abbreviation the richest network, however, is and Acronym located in the renal pelvis. Signals are transmitted by 2 families SNS ⴝ sympathetic nervous system of receptors, the mechanosensitive receptors that relay information regarding hydrostatic renal pelvic pressure, as well as renal arterial and venous pressure, and chemosensitive receptors activated by renal ischemia and changes in the chemical milieu of the renal interstitium (37). Afferent sympathetic dorsal root neurons transmit signals to the central nervous system. By their communication with sympathetic centers in the central nervous system, afferent sympathetic signals assume a major role in the regulation of overall sympathetic tone. This is elegantly demonstrated in an animal model whose kidneys have been injured by phenol injection. Blood pressure rises after phenol injections are prevented by prior dorsal rhizotomy (selective afferent sympathetic fiber interruption by transection of the dorsal roots) (38). Similarly, in rats with renal insufficiency, hypertension can be prevented by dorsal rhizotomy (39). Thus, the SNS has a profound effect on the kidney’s ability to regulate the goal blood pressure, and, vice versa, the kidney has an important effect on the overall sympathetic tone. In addition, afferent fibers communicate with the contralateral kidney, thereby allowing maintenance of sodium and water balance despite unilateral disturbances of salt and water excretion (40). For example, a unilateral increase in hydrostatic pressure (e.g., because of ureteral 252 Bertog et al. Renal Denervation for Hypertension JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 5, NO. 3, 2012 MARCH 2012:249 –58 Figure 1. The Renal SNS NTS ⫽ solitary tract nucleus; PVN ⫽ paraventricular nucleus; RVLM ⫽ rostral ventrolateral medulla. obstruction and hydronephrosis), via an increase in afferent sympathetic activity transmitted to the efferent fibers of the contralateral kidney, reduces the efferent renal sympathetic activity and, thereby, results in diuresis and natriuresis in the contralateral kidney (renorenal reflex) (40). When examining the role of the SNS in the genesis of hypertension, it is important to recognize that it is not activated in an all-on or all-off fashion. Instead, the sympathetic activity to certain organs only (e.g., the kidney or heart) (41) can be increased and thus have an impact on blood pressure control in the absence of a substantial activation of sympathetic fibers to other organs. This, in addition to differences in catecholamine metabolism, may explain variability in blood catecholamine levels in hypertensive patients. Two methods have allowed a more refined assessment of the SNS activity in humans: microneurography (42) and norepinephrine spillover (43,44). Microneurography measures the SNS activity in skeletal muscles. It can be used as a surrogate for overall sympathetic drive. Norepinephrine spillover can be used to measure organ-specific as well as overall SNS activity. JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 5, NO. 3, 2012 MARCH 2012:249 –58 Results of Percutaneous Sympathetic Denervation in Humans Our better understanding of the interplay between the kidney and SNS elucidates the importance of the SNS in blood pressure control and the pathogenesis of hypertension. In addition, the desirable results of sympathetic denervation in animal models and in patients who have undergone nephrectomies, together with the recognition of the favorable location of the sympathetic fibers and their exquisite sensitivity to radiofrequency, have resulted in the development of catheter-based radiofrequency ablation of the renal sympathetic nervous fibers. In a human feasibility, safety, and efficacy trial (Symplicity-1 [Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study]), 45 patients with drug-resistant hypertension underwent bilateral application of radiofrequency to the renal arteries (45). After renal artery angiography, anticoagulation and administration of opioid analgesics for control of diffuse abdominal pain that invariably occurs during this procedure, via 8-F femoral artery access, an 8-F guide catheter was positioned in the renal arteries, allowing delivery of a radiofrequency catheter (Fig. 2) into the renal arteries and circumferential application of radiofrequency energy (Fig. 3). The catheter tip is steerable via a hand control and is connected to a console (Fig. 4). Delivery of radiofrequency energy was monitored with a temperature and impedance sensor at the tip of the catheter such that unwanted tissue injury related to overheating was avoided. Two procedure-related complications occurred: 1 renal artery dissection related to catheter manipulation, which was treated successfully with renal artery stenting; and 1 femoral artery pseudoaneurysm. A significant blood pressure reduction at 1-month follow-up of 14 and 10 mm Hg (systolic and diastolic, respectively) was followed by a Bertog et al. Renal Denervation for Hypertension 253 sustained response with a pronounced systolic and diastolic blood pressure reduction of 27 and 17 mm Hg, respectively, at 12 months. Antihypertensive medication was adjusted in 13 patients at follow-up with a reduction in the number of antihypertensive medications in 9 patients and an increase in 4. Importantly, a significant blood pressure reduction remained even after excluding those 4 patients from the analysis whose antihypertensive medications were intensified. In 13% of patients, no favorable blood pressure response occurred. In 10 patients who underwent renal norepinephrine spillover measurements, a significant reduction in renal norepinephrine spillover was shown, confirming the intended reduction in sympathetic drive to the kidney. In addition, total body norepinephrine spillover decreased significantly, lending support to the hypothesis that, by a reduction in afferent renal sympathetic signaling, the overall sympathetic tone can be reduced. In 1 patient, renal norepinephrine spillover, total body norepinephrine spillover, the plasma renin level, and muscle sympathetic activity decreased after renal denervation (46). In addition, the cardiac muscle mass assessed by cardiac magnetic resonance imaging decreased by 15 g. Registry data, including patients from Symplicity-1 who have completed 24months follow-up (n ⫽ 18), demonstrate a sustained blood pressure reduction (33/14 mm Hg) (47). More recently, in the Symplicity HTN-2 (Renal Sympathetic Denervation in Patients with Treatment-Resistant Hypertension) trial, 106 patients with resistant hypertension were randomized to catheter-based therapy in addition to conventional antihypertensive medications, versus antihypertensive medications only, in a 1-to-1 fashion (48). The transcatheter techniques were similar to the previously described study. The primary endpoint was systolic blood pressure at 6-month follow-up. There was a significant difference in blood pressure changes from baseline between Figure 2. Fluoroscopic Images of Catheter Positions in the Renal Artery (Left) Radiofrequency catheter positioned in the right renal artery. (Right) Contrast injection into the right renal artery. 254 Bertog et al. Renal Denervation for Hypertension JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 5, NO. 3, 2012 MARCH 2012:249 –58 Figure 3. Radiofrequency Catheter Positioning in the Renal Artery Radiofrequency catheter positioning in the renal artery aiming at circumferential application of radiofrequency spaced apart by approximately 5 mm. Reprinted, with permission, from Medtronic Ardian, Mountainview, California. patients treated with catheter-based renal sympathectomy (reductions of 32/12 ⫾ 23/11 mm Hg) and those treated medically (0/1 ⫾ 21/10 mm Hg), with a mean blood pressure difference of 33/11 mm Hg between the groups at 6 months. A systolic blood pressure improvement of at least 10 mm Hg was observed in 84% of patients in the interventional group and in 35% in the medically treated control group. On 24-h ambulatory blood pressure monitoring, a significant blood pressure reduction was seen in patients who underwent renal sympathectomy (11/7 ⫾ 15/11 mm Hg), whereas the blood pressure was unchanged in patients with medically managed hypertension only. Importantly, the blood pressure reduction measured by 24-h ambulatory monitoring was less pronounced than that reported during office visits. One patient developed a pseudoaneurysm at the femoral access site treated successfully with ultrasound-guided manual compression. Seven patients developed transient bradycardia requiring atropine administration. The renal function and urine-albumincreatinine ratios remained unchanged at follow-up in both groups. Limitations to Human Experience With Catheter-Based Renal Sympathetic Denervation Figure 4. Symplicity Catheter System The steerable radiofrequency catheter is shown and the console that provides feedback to the operator regarding impedance and radiofrequency energy delivery as well as duration of energy application. Reprinted, with permission, from Medtronic Ardian, Mountainview, California. The results of Symplicity-1 and Symplicity HTN-2 are very encouraging; however, several limitations deserve discussion. Symplicity-1 was a proof-of-principle study that did not include a control group and operators and investigators were unblinded. Therefore, though the blood pressure remained JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 5, NO. 3, 2012 MARCH 2012:249 –58 unchanged in 5 patients who were excluded from the study, a placebo effect and observer bias cannot be excluded. Second, patients with accessory renal arteries were excluded. Hence, it cannot be assumed that renal denervation in the main renal arteries will translate into a similar beneficial effect in patients who have accessory renal arteries. Third, screening for secondary hypertension was limited. Fourth, 13% of patients were nonresponders. The reason for the absence of a blood pressure response in these patients remains unclear, as renal or overall sympathetic activity was not consistently measured before or after renal denervation in these patients. In Symplicity HTN-2, though the design was a randomized controlled trial, the investigators who performed blood pressure measurements were not blinded to the treatment mode. In addition, sham procedures were not performed in the control group. Hence, once again, a placebo effect and observer bias cannot be entirely ruled out. Given well-described pulmonary vein stenoses after radiofrequency pulmonary vein isolation to treat atrial fibrillation, concerns have been raised regarding the possibility of renal artery stenosis caused by application of radiofrequency to the renal arteries. However, the intensity of radiofrequency energy is several magnitudes lower than that used for pulmonary vein isolation. In Symplicity-1, in 18 patients who underwent renal angiography 2 to 4 weeks after the procedure and in 14 patients who underwent renal artery magnetic resonance imaging, no renal artery stenosis was seen. Of note, in 1 registry patient, progression of a mild renal artery stenosis to a hemodynamically significant lesion remote from the site of radiofrequency application requiring renal artery stenting was reported (47). Similarly, in Symplicity HTN-2, in 43 of 49 patients who underwent renal sympathectomy, renal artery imaging at 6-month follow-up did not show any significant renal artery stenosis or aneurysmal deformation. Nevertheless, despite the absence of treatment-related renal artery stenoses in both studies, a risk of renal artery stenosis in longer-term follow-up cannot be excluded at this point. In both Symplicity trials, only patients with renal arteries with an anatomy favorable to catheter-based therapy (minimal length of 20 mm allowing an adequate landing zone and minimal diameter of 4 mm) were included. A higher procedural risk in patients with more unfavorable anatomy is possible. Patients with more than mild renal insufficiency were excluded even though sympathetic overactivity is typically pronounced in the setting of renal insufficiency. In these patients, though a favorable effect on blood pressure control is anticipated, definitive statements regarding the benefit and safety of renal denervation cannot be made. The office blood pressure response in Symplicity HTN-2 was more pronounced than the ambulatory blood pressure response. This may be related to a more pronounced Bertog et al. Renal Denervation for Hypertension 255 activation of the SNS with office blood pressure measurements than during ambulatory blood pressure monitoring and hence more marked effect after renal denervation. Finally, similar to sympathetic reinnervation described after heart transplantation (49), sympathetic reinnervation to the kidney is conceivable and may abolish or attenuate a long-term effect. However, regrowth of sympathetic nerve fibers to the kidneys has not been shown in humans (50). Moreover, given the absence of angina in patients with transplant vasculopathy after heart transplantation, afferent sympathetic reinnervation is less likely. In addition, in those patients enrolled in Symplicity-1 and additional patients who underwent renal sympathetic denervation, 2-year follow-up demonstrated a pronounced lasting blood pressure reduction (47). Future Perspectives The importance of the renal SNS activity in hypertension and its modulation are well established. Several aspects deserve further exploration. First, it has become apparent that this procedure does not cause universal blood pressure lowering. The reason for the response variability remains to be determined. One potential cause may be incomplete denervation. It is also possible that renal sympathetic activity has a subordinate role in the genesis and maintenance of hypertension in subsets of hypertensive patients with normal renal sympathetic tone. The renal sympathetic tone is not uniformly increased. Instead, there appears to be variability in renal efferent sympathetic nerve activity in hypertensive patients. For example, in patients older than 60 years, though skeletal muscle sympathetic activity is increased, renal norepinephrine spillover is frequently normal (3), whereas in patients with the metabolic syndrome, renal and overall sympathetic overactivity is frequently very pronounced (51,52). Thus, it would be very important to identify parameters that may predict the response to renal denervation and help in patient selection. Second, the SNS activity appears to be of most importance in the earlier stages of hypertension. Early modification of SNS activity in these patients may bring a curative treatment for essential hypertension within reach. Thus, trials, including patients with milder forms of hypertension are warranted. Exploration of the impact of renal denervation in patients with secondary forms of hypertension, such as primary hyperaldosteronism that cannot be treated with surgical intervention should also be considered. Third, obesity and insulin resistance are frequent companions of hypertension. Sympathetic overactivity has been observed with obesity, insulin resistance, and the metabolic syndrome, and improvements in glucose metabolism and insulin resistance have been reported after renal sympathetic denervation (53–55). A compromised skeletal muscle mi- 256 Bertog et al. Renal Denervation for Hypertension crocirculation has been suggested to be present in patients with hypertension (56). Sympathetic denervation may enhance skeletal muscle blood flow mediated by a reduction in adrenergic alpha-1 receptor stimulation, increased skeletal muscle-capillary density, and a change in muscle fiber types (57), thereby potentially improving glucose uptake in the skeletal muscle. In addition, a decrease in glucagon secretion and gluconeogenesis and reduced activity of the reninangiotensin system may contribute to the beneficial effects of renal denervation on glucose metabolism and insulin resistance. Although our current understanding of the preceding findings is far from complete, given the high incidence of cardiovascular events in patients with insulin resistance and impaired glucose metabolism and the favorable impact of reduced sympathetic drive, lower event rates after renal denervation are conceivable. Studies to this effect evaluating the impact of sympathetic denervation on diabetes control and cardiovascular events are ongoing. In addition, further exploration of the impact of renal sympathectomy on the development of diabetic nephropathy is warranted as increases in glomerular filtration of up to 25% to 50% have been described early in the course of (type 1) diabetes, perhaps contributing to the development of glomerulosclerosis and diabetic nephropathy (58,59), and prevention of glomerular hyperfiltration has been reported after renal sympathetic denervation in an animal model (60). Similarly, moxonidine, a central sympathetic inhibitor has been associated with a reduction in microalbuminuria in patients with (type 1) diabetes (61). Further supporting a potentially protective effect on renal function beyond that expected due to blood pressure reduction, the natural decline in estimated glomerular filtration rate expected depending on blood pressure at any given time was smaller than predicted at early follow-up, even after taking the blood pressure reduction into account, after renal denervation in 153 hypertensive patients (including those enrolled in Symplicity-1) (47). However, in a small number of patients who completed later (up to 24 months) follow-up, the reduction in estimated glomerular filtration rate was more pronounced than that observed in a study examining the effect of ramipril, telmisartan, or both on renal function (62). Given these findings, further studies of the long-term impact on renal hemodynamics and function, particularly comparing renal denervation in a controlled fashion to conventional medical therapy, are warranted before a final statement regarding either a protective, neutral, or harmful effect can be made. Fourth, the impact of renal denervation on the renorenal reflex particularly in conditions affecting only 1 kidney is not clear. For example, whether during urinary obstruction of 1 kidney a compensatory diuresis of the contralateral kidney can be expected in the same magnitude as would occur in the absence of renal denervation remains to be determined. JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 5, NO. 3, 2012 MARCH 2012:249 –58 Fifth, the autonomic nervous system affects nearly every part of the body. Given the myriad effects of an overactive SNS beyond blood pressure control, many of which are detrimental, renal denervation in some conditions associated with sympathetic overactivity require further investigation. For example, in light of increased SNS activity in patients with systolic heart failure (63), its association with increased mortality (64) and the well-established benefits of beta adrenoreceptor blockade (65) and modification of the renin-angiotensin system (66), the concept of renal denervation to reduce overall sympathetic drive in heart failure is intriguing. Along this line, a reduction in left ventricular filling pressures and improved left ventricular systolic function following renal denervation has been shown in animal models of heart failure (67). Similarly, a potential benefit in patients with hepatorenal syndrome characterized by SNS overactivity (68) is possible. Lastly, an increased sympathetic drive has been described in patients with sleep apnea, together with a favorable impact on the apnea-hypopnea index after catheter-based renal sympathetic denervation (53). Hypothetically, this may be related to a reduction in fluid shifts to the neck with recumbent positioning after renal denervation based on the observation that a greater fluid shift from the lower extremities to the neck occurs in patients with uncontrolled versus well-controlled hypertension (69). The reported improvements in sleep apnea with aldosterone antagonists further supports a potential deleterious effect of excessive nocturnal rostral fluid shifts (70). Studies examining the mechanism and impact of sympathetic denervation in patients with sleep apnea are ongoing. Finally, it should be mentioned that catheter-based renal denervation is not the only device-based therapy available aiming to reduce the sympathetic nervous tone. Similar to renal sympathetic denervation, baroreceptor stimulation reduces the overall SNS activity and has been shown to lower blood pressure in a safety and feasibility trial (71). Recently, the results of a phase III trial comparing baroreceptor stimulation to conventional medical therapy in patients with resistant hypertension were published demonstrating a significant blood pressure reduction (72). However, it failed to meet 1 of the 2 primary efficacy endpoints (blood pressure responder rate at 6 months) likely related to an underestimation of blood pressure improvements in the control group. Importantly, as expected with the implantation of any foreign body, some adverse events occurred (4.8% nerve injury with residual deficit and 2.6% wound complications). Further studies will determine this concept’s role in hypertension treatment. Conclusions We have entered an exciting era with the ability to modulate the SNS and achieve an improvement in blood pressure JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 5, NO. 3, 2012 MARCH 2012:249 –58 control with percutaneous renal denervation and potentially beneficial effects on a plethora of other conditions associated with sympathetic overactivity. Renal denervation has become routine in some countries. Nevertheless, we should maintain our quest to further improve our understanding of the SNS in the pathogenesis of hypertension and some other disorders. Lastly, the SNS and mechanisms governing blood pressure control are complex and, though the procedure has demonstrated a good safety record, some longterm consequences may not be foreseeable. Therefore, systematic follow-up of patients who underwent renal sympathetic denervation is warranted. Only carefully planned trials further elucidating the physiology and examining the clinical effects of renal denervation on multiple levels will allow safe adoption of a promising concept and technology for patients with a variety of conditions other than hypertension. Reprint requests and correspondence: Dr. Horst Sievert, Cardiovascular Center Frankfurt, Seckbacher Landstrasse 65, 60389 Frankfurt, Germany. E-mail: [email protected]. REFERENCES 1. Goldstein DS. Plasma catecholamines and essential hypertension: an analytical review. Hypertension 1983;5:86 –99. 2. Anderson EA, Sinkey CA, Lawton WJ, Mark AL. Elevated sympathetic nerve activity in borderline hypertensive humans: evidence from direct intraneural recordings. Hypertension 1989;14:177– 83. 3. Esler M, Lambert G, Jennings G. Regional norepinephrine turnover in human hypertension. Clin Exp Hypertens A 1989;11 Suppl 1:75– 89. 4. Sakata K, Shirotani M, Yoshida H, Kurata C. Comparison of effects of enalapril and nitrendipine on cardiac sympathetic nervous system in essential hypertension. J Am Coll Cardiol 1998;32:438 – 43. 5. Schlaich MP, Lambert E, Kaye DM, et al. Sympathetic augmentation in hypertension: role of nerve firing, norepinephrine reuptake, and angiotensin neuromodulation. Hypertension 2004;43:169 –75. 6. Smith PA, Graham LN, Mackintosh AF, Stoker JB, Mary DA. Relationship between central sympathetic activity and stages of human hypertension. Am J Hypertens 2004;17:217–22. 7. Grimson KS. Total thoracic and partial to total lumbar sympathectomy and celiac ganglionectomy in the treatment of hypertension. Ann Surg 1941;114:753–75. 8. Peet M, Woods W, Braden S. The surgical treatment of hypertension: results in 350 consecutive cases treated by bilateral supradiaphragmatic splanchnicectomy and lower dorsal sympathetic gangliectomy. Clinical lecture at New York session. JAMA 1940;115:1875– 85. 9. Smithwick RH. Surgery in hypertension. Lancet 1948;2:65. 10. Grimson KS, Orgain ES, Anderson B, Broome RA, Longino FH. Results of treatment of patients with hypertension by total thoracic and partial to total lumbar sympathectomy, splanchnicectomy and celiac ganglionectomy. Ann Surg 1949;129:850 –71. 11. Evelyn KA, Alexander F, Cooper SR. Effect of sympathectomy on blood pressure in hypertension: a review of 13 years’ experience of the Massachusetts General Hospital. JAMA 1949;140:592– 602. 12. Hinton JW. End results of thoracolumbar sympathectomy for advanced essential hypertension. Bull N Y Acad Med 1948;24:239 –52. 13. Hammarstrom S, Bechgaard P. Prognosis in arterial hypertension: comparison between 251 patients after sympathectomy and selected series of 435 non-operated patients. Am J Med 1950;8:53– 6. 14. Converse RL Jr., Jacobsen TN, Toto RD, et al. Sympathetic overactivity in patients with chronic renal failure. N Engl J Med 1992;327: 1912– 8. 15. Hausberg M, Kosch M, Harmelink P, et al. Sympathetic nerve activity in end-stage renal disease. Circulation 2002;106:1974 –9. Bertog et al. Renal Denervation for Hypertension 257 16. Ask-Upmark. Ueber juvenile maligne Nephrosclerose und ihr Verhaeltnis zu Stoerungen in der Nierenentwicklung [Juvenille malignant nephrosclerosis and its role in disorders in kidney development]. Acta Pathol Microbiol Scand 1929;6:383– 442. 17. Butler AM. Chronic pyelonephritis and arterial hypertension. J Clin Invest 1937;16:889 –97. 18. Smith HW. Hypertension and urologic disease. Am J Med 1948;4: 724 – 43. 19. Cohen SL. Hypertension in renal transplant recipients: role of bilateral nephrectomy. Br Med J 1973;3:78 – 81. 20. McHugh MI, Tanboga H, Marcen R, Liano F, Robson V, Wilkinson R. Hypertension following renal transplantation: the role of the host’s kidney. Q J Med 1980;49:395– 403. 21. Huysmans FT, van Heusden FH, Wetzels JF, Hoitsma AJ, Koene RA. Antihypertensive effect of beta blockade in renal transplant recipients with or without host kidneys. Transplantation 1988;46:234 –7. 22. Ligtenberg G, Blankestijn PJ, Oey PL, et al. Reduction of sympathetic hyperactivity by enalapril in patients with chronic renal failure. N Engl J Med 1999;340:1321– 8. 23. Miyajima E, Yamada Y, Yoshida Y, et al. Muscle sympathetic nerve activity in renovascular hypertension and primary aldosteronism. Hypertension 1991;17:1057– 62. 24. Perry CB. Malignant hypertension cured by unilateral nephrectomy. Br Heart J 1945;7:139 – 42. 25. Abramczyk P, Zwoliñska A, Oficjalski P, Przybylski J. Kidney denervation combined with elimination of adrenal-renal portal circulation prevents the development of hypertension in spontaneously hypertensive rats. Clin Exp Pharmacol Physiol 1999;26:32– 4. 26. Quinby WC. The function of the kidney when deprived of its nerves. J Exp Med 1916;23:535– 48. 27. Kottke FJ, Kubicek WG, Visscher MB. The production of arterial hypertension by chronic renal artery-nerve stimulation. Am J Physiol 1945;145:38 – 47. 28. Müller J, Barajas L. Electron microscopic and histochemical evidence for a tubular innervation in the renal cortex of the monkey. J Ultrastruct Res 1972;41:533– 49. 29. Barajas L. The innervation of the juxtaglomerular apparatus: an electron microscopic study of the innervation of the glomerular arterioles. Lab Invest 1964;13:916 –29. 30. Ljungqvist A, Wågermark J. The adrenergic innervation of intrarenal glomerular and extra-glomerular circulatory routes. Nephron 1970;7: 218 –29. 31. Barajas L, Wang P. Localization of tritiated norepinephrine in the renal arteriolar nerves. Anat Rec 1979;195:525–34. 32. Aperia A, Ibarra F, Svensson LB, Klee C, Greengard P. Calcineurin mediates alpha-adrenergic stimulation of Na⫹,K(⫹)-ATPase activity in renal tubule cells. Proc Natl Acad Sci U S A 1992;89:7394 –7. 33. Skøtt O, Jensen BL. Cellular and intrarenal control of renin secretion. Clin Sci (Lond) 1993;84:1–10. 34. Koepke JP, DiBona GF. Functions of the renal nerves. Physiologist 1985;28:47–52. 35. Ciriello J, Calaresu FR. Central projections of afferent renal fibers in the rat: an anterograde transport study of horseradish peroxidase. J Auton Nerv Syst 1983;8:273– 85. 36. Rosas-Arellano MP, Solano-Flores LP, Ciriello J. c-Fos induction in spinal cord neurons after renal arterial or venous occlusion. Am J Physiol 1999;276:R120 –7. 37. Ciriello J, de Oliveira CV. Renal afferents and hypertension. Curr Hypertens Rep 2002;4:136 – 42. 38. Ye S, Zhong H, Yanamadala V, Campese VM. Renal injury caused by intrarenal injection of phenol increases afferent and efferent renal sympathetic nerve activity. Am J Hypertens 2002;15:717–24. 39. Campese VM, Kogosov E. Renal afferent denervation prevents hypertension in rats with chronic renal failure. Hypertension 1995;25:878 – 82. 40. Kopp UC, Smith LA, DiBona GF. Renorenal reflexes: neural components of ipsilateral and contralateral renal responses. Am J Physiol 1985;249:F507–17. 41. Esler M, Jennings G, Lambert G, Meredith I, Horne M, Eisenhofer G. Overflow of catecholamine neurotransmitters to the circulation: source, fate, and functions. Physiol Rev 1990;70:963– 85. 258 Bertog et al. Renal Denervation for Hypertension JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 5, NO. 3, 2012 MARCH 2012:249 –58 42. Vallbo AB, Hagbarth KE, Wallin BG. Microneurography: how the technique developed and its role in the investigation of the sympathetic nervous system. J Appl Physiol 2004;96:1262–9. 43. Esler M, Jennings G, Korner P, Blombery P, Sacharias N, Leonard P. Measurement of total and organ-specific norepinephrine kinetics in humans. Am J Physiol 1984;247:E21– 8. 44. Esler M, Jennings G, Korner P, et al. Total, and organ-specific, noradrenaline plasma kinetics in essential hypertension. Clin Exp Hypertens A 1984;6:507–21. 45. Krum H, Schlaich M, Whitbourn R, et al. Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study. Lancet 2009;373:1275– 81. 46. Schlaich MP, Sobotka PA, Krum H, Lambert E, Esler MD. Renal sympathetic-nerve ablation for uncontrolled hypertension. N Engl J Med 2009;361:932– 4. 47. Symplicity HTN-1 Investigators. Catheter-based renal sympathetic denervation for resistant hypertension: durability of blood pressure reduction out to 24 months. Hypertension 2011;57:911–7. 48. Esler MD, Krum H, Sobotka PA, et al., for the Symplicity HTN-2 Investigators. Renal sympathetic denervation in patients with treatment-resistant hypertension (the Symplicity HTN-2 trial): a randomised controlled trial. Lancet 2010;376:1903–9. 49. Kaye DM, Esler M, Kingwell B, McPherson G, Esmore D, Jennings G. Functional and neurochemical evidence for partial cardiac sympathetic reinnervation after cardiac transplantation in humans. Circulation 1993;88:1110 – 8. 50. Hansen JM, Abildgaard U, Fogh-Andersen N, et al. The transplanted human kidney does not achieve functional reinnervation. Clin Sci (Lond) 1994;87:13–20. 51. Grassi G, Dell’Oro R, Quarti-Trevano F, et al. Neuroadrenergic and reflex abnormalities in patients with metabolic syndrome. Diabetologia 2005;48:1359 – 65. 52. Huggett RJ, Burns J, Mackintosh AF, Mary DA. Sympathetic neural activation in nondiabetic metabolic syndrome and its further augmentation by hypertension. Hypertension 2004;44:847–52. 53. Witkowski A, Prejbisz A, Florczak E, et al. Effects of renal sympathetic denervation on blood pressure, sleep apnea course, and glycemic control in patients with resistant hypertension and sleep apnea. Hypertension 2011;58:559 – 65. 54. Mahfoud F, Schlaich M, Kindermann I, et al. Effect of renal sympathetic denervation on glucose metabolism in patients with resistant hypertension: a pilot study. Circulation 2011;123:1940 – 6. 55. Schlaich MP, Straznicky N, Grima M, et al. Renal denervation: a potential new treatment modality for polycystic ovary syndrome? J Hypertens 2011;29:991– 6. 56. Julius S, Gudbrandsson T, Jamerson K, Tariq Shahab S, Andersson O. The hemodynamic link between insulin resistance and hypertension. J Hypertens 1991;9:983– 6. 57. Koistinen HA, Zierath JR. Regulation of glucose transport in human skeletal muscle. Ann Med 2002;34:410 – 8. 58. Mogensen CE. Glomerular filtration rate and renal plasma flow in normal and diabetic man during elevation of blood sugar levels. Scand J Clin Lab Invest 1971;28:177– 82. 59. Christiansen JS, Gammelgaard J, Tronier B, Svendsen PA, Parving HH. Kidney function and size in diabetics before and during initial insulin treatment. Kidney Int 1982;21:683– 8. 60. Luippold G, Beilharz M, Mühlbauer B. Chronic renal denervation prevents glomerular hyperfiltration in diabetic rats. Nephrol Dial Transplant 2004;19:342–7. 61. Strojek K, Grzeszczak W, Górska J, Leschinger MI, Ritz E. Lowering of microalbuminuria in diabetic patients by a sympathicoplegic agent: novel approach to prevent progression of diabetic nephropathy? J Am Soc Nephrol 2001;12:602–5. 62. Petidis K, Anyfanti P, Doumas M. Renal sympathetic denervation: renal function concerns. Hypertension 2011;58:e19, author reply e20. 63. Hasking GJ, Esler MD, Jennings GL, Burton D, Johns JA, Korner PI. Norepinephrine spillover to plasma in patients with congestive heart failure: evidence of increased overall and cardiorenal sympathetic nervous activity. Circulation 1986;73:615–21. 64. Cohn JN, Levine TB, Olivari MT, et al. Plasma norepinephrine as a guide to prognosis in patients with chronic congestive heart failure. N Engl J Med 1984;311:819 –23. 65. Packer M, Bristow MR, Cohn JN, et al., for the U.S. Carvedilol Heart Failure Study Group. The effect of carvedilol on morbidity and mortality in patients with chronic heart failure. N Engl J Med 1996;334:1349 –55. 66. The CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N Engl J Med 1987;316:1429 –35. 67. Nozawa T, Igawa A, Fujii N, et al. Effects of long-term renal sympathetic denervation on heart failure after myocardial infarction in rats. Heart Vessels 2002;16:51– 6. 68. Ring-Larsen H, Henriksen JH, Wilken C, Clausen J, Pals H, Christensen NJ. Diuretic treatment in decompensated cirrhosis and congestive heart failure: effect of posture. Br Med J 1986;292:1351–3. 69. Friedman O, Bradley TD, Chan CT, Parkes R, Logan AG. Relationship between overnight rostral fluid shift and obstructive sleep apnea in drug-resistant hypertension. Hypertension 2010;56:1077– 82. 70. Gaddam K, Pimenta E, Thomas SJ, et al. Spironolactone reduces severity of obstructive sleep apnoea in patients with resistant hypertension: a preliminary report. J Hum Hypertens 2010;24:532–7. 71. Scheffers IJ, Kroon AA, Schmidli J, et al. Novel baroreflex activation therapy in resistant hypertension: results of a European multi-center feasibility study. J Am Coll Cardiol 2010;56:1254 – 8. 72. Bisognano JD, Bakris G, Nadim MK, et al. Baroreflex activation therapy lowers blood pressure in patients with resistant hypertension: results from the double-blind, randomized, placebo-controlled Rheos Pivotal Trial. J Am Coll Cardiol 2011;58:765–73. Key Words: hypertension 䡲 renal denervation 䡲 sympathetic nervous system. To participate in this CME activity by taking the quiz and claiming your CME credit certificate, please go to http://interventions.onlinejacc.org/ and select the CME tab on the top navigation bar.