Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
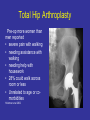
Osteoarthritis: Impact of Sex and Gender Kim Templeton, MD AMWA Annual Meeting March 2016 CONFLICT OF INTEREST I hereby certify that, to the best of my knowledge, no aspect of my current personal or professional situation might reasonably be expected to affect significantly my views on the subject on which I am presenting. Institute of Medicine Report 2001 • Every cell has a sex • Sex=genetic (gonadal) complement • Gender=social interactions, available resources Sex and Gender-Based Differences • Anatomy • Physiology (especially immune system) • Effect of sex hormones local systemic • Environmental influences • Impact on incidence, presentation, response to treatment, prevention Musculoskeletal System • • • • • • • • • Polymyositis Myasthenia gravis Duchenne muscular dystrophy Becker muscular dystrophy TMJ (syndrome) Adhesive capsulitis Shoulder instability/subluxation Hallux valgus Hip dysplasia Musculoskeletal System • • • • • • Scoliosis (de Quervain) tenosynovitis Carpal tunnel syndrome Rheumatoid arthritis Systemic lupus erythematosus Psoriatic arthritis Musculoskeletal System • • • • • • Adolescent scoliosis Anterior knee pain (syndrome) Hallux valgus Female athlete triad Stress fracture Osteoporosis (primary and secondary) • Cervical spondyolosis Musculoskeletal System • • • • • • • • Trochanteric bursitis Iliotibial band syndrome Morton neuroma Breast carcinoma metastatic to bone Fibromyalgia Ehlers Danlos syndrome ACL injury Osteoarthritis (especially knee and 1st CMC) Osteoarthritis Incidence • Depends on definition • About 14% of people over 25 y/o (CDC) • 34% over the age of 65 • 25% lifetime risk (about 30% for women, 20% for men) • Primary cause of disability Sex/Gender Differences Female/male OA per 100 • • Radiographic hand 9.5/4.8 feet 2.7/1.5 knee 1.2/0.4 hip 1.4/1.4 Symptomatic OA hand 8.9/6.7 feet 3.6/1.6 knee 13.6/10.0 CDC data Sex/Gender-Specific Osteoarthritis Risk Factors • Acquired injury patterns of overuse • Inherent impact of estrogen muscle strength anatomy Joint Injury • Significantly higher risk of OA in younger people after knee injury-even with reconstruction • Earlier among women than men with ACL injuries Roos Current Opinion in Rheumatology 2005 Shoe Wear • Heel height leads to greater knee flexion, anterior pelvic tilt, trunk extension, slower walking speeds • As heel height increased, increased internal knee abduction (external adduction) moments • Increases inherent adduction moment • Increased peak joint forces • Impact on medial compartment of knee? Barkema et al 2011 Thumb CMC Arthritis • Overall prevalence noted incidentally on radiographs • No significant correlation with physical workload history • Effects of decreased estrogen and increased laxity? • Significant impact on function and independence Sohda et al JBJS 2005 Effects of Estrogen • Estrogen receptors on chondrocytes, bone, synoviocytes • Promotes chondrocyte proliferation, differentiation, matrix formation • Inhibits production of MMPs • Differences in response to estrogen of male and female chondrocytes Estrogen and OA • OVX rats noted to have surface cartilage erosions at 9 weeks • Lower incidence of erosion in rats treated with estrogen or SERM • 50% decrease in urinary excretion of type II collagen degradation products at 12 months in postmenopausal women treated with SERM Christgau et al 2004 Effects of Estrogen • Ovariectomized mice with model of induced OA • Increased cartilage injury • Due to loss of bone or direct effect on cartilage? Sniekers et al 2010 Femoroacetabular Impingement • Acetabular dysplasia higher in women • Cam vs pincer • Pincer more common in women • Acetabular retroversion and/or overcoverage • Repetitive impaction of acetabular rim and femoral head/neck PFP-Risk Factors • • • • • • • • • • • • • • Large Q-angle Foot pronation Increased femoral anteversion Genu valgum External tibial torsion Tibia vara Patellar ligamentous hypermobility Insufficient VMO vs v. lateralis Generalized ligamentous laxity Tight lateral patellar retinaculum Tight IT band Patella alta Shallower femoral notch Narrower patella Muscle Strength • Quads strength in women with higher in those without OA or fewer radiographic changes • Only ½ had OArelated pain • Impact of strength on development of OA? Palmieri-Smith et al 2010 Sex-Based Differences in Osteoarthritis? 508 patients with hip OA Women more likely to have • polyarticular disease • superolateral migration of femoral head • more severe symptoms • more rapid loss of joint space Maillefert et al 2003 Treatment Non-surgical • • • • • • • • • • • Activity modification Weight loss Exercise Muscle strengthening/exercise NSAIDs Glucosamine/chondroitin sulfate Narcotics Topical rubs (NSAIDs, capsaicin) Injections No sex-based differences in response No objective indication for TJA Gender Influences on Total Joint Arthroplasty • Performed more often in women • Estimated three-fold underuse in women compared to men (Ontario) • Equivalent willingness to undergo the procedure • Women less likely to have spoken to physician regarding surgery (most important predictor of having surgery) Hawker et al 2000 Patient Concerns • Men reported willingness TJA when no longer able to perform vigorous outdoor activity • Women reported willingness for TJA when limited in indoor ambulation Karlson et al 1997 Total Joint Arthroplasty • Men more likely to be referred for TJA by their primary care provider (HR 1.25 overall) after adjusting for medical factors, even in age group 20-39 • Impact of SES more significant for men • Bias regarding social expectations, anticipated results of TJA? Rahman et al 2010 Pre-operative Function • Patients with end-stage OA and waiting for TKA/THA • Women with significantly poorer health-related QOL scores, self-efficacy (confidence in management of pain, fatigue, etc), and function Ackerman et al 2005 Total Hip Arthroplasty Pre-op more women than men reported • severe pain with walking • needing assistance with walking • needing help with housework • 28% could walk across room or less • Unrelated to age or comorbidities Holtzman et al 2002 Results of THA • Women with worse WOMAC scores (function, pain, stiff) and SF-36 physical function, pain , social function preoperatively • Both genders improved post-operatively • No significant difference in post-operative scores, but women with worse scores at all time points Lavernia et al 2011 THA Outcome • Total joint replacement registry • 35,140 primary, elective, unilateral • Women 57.5% of sample • 29% higher risk of aseptic implant failure • Hazard ratio 1.97 for metal-on-metal • Partly explained by smaller head size (instability) Nepple et al JAMA 2013 Metal-on-metal THA Outcome • Increased risk of failure due to aseptic loosening and pseudotumors • Not related to implant size or orientation (latter significant for men) • Enhanced inflammatory response? Pre-op sensitization due to jewelry wear? • Not recommended for use in women Latteier et al 2011 TKA-Results • Results of TKA rely on sizes of implants? • Implants more closely match the average male bone size • Soft tissue impingement? Hitt et al 2003 Future Directions • Injury prevention • Early identification • Encouraging/empowering pts to seek care earlier (e.g., OAAA) • Ask pts earlier about pain and function • Identify best practices (e.g., COAMI) • Continued exploration/discussion of impact of sex and gender Thank You!