Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
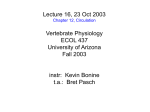
Am J Physiol Heart Circ Physiol 302: H2654–H2662, 2012. First published April 27, 2012; doi:10.1152/ajpheart.00072.2012. Atrial septostomy benefits severe pulmonary hypertension patients by increase of left ventricular preload reserve Yvette Koeken,1 Nico H. L. Kuijpers,1 Joost Lumens,2 Theo Arts,1 and Tammo Delhaas1 1 Department of Biomedical Engineering, Maastricht University, Maastricht, The Netherlands; and 2Unité de Rythmologie et Stimulation Cardiaque, Hôpital Cardiologique du Haut-Lévêque, Bordeaux, France Submitted 24 January 2012; accepted in final form 14 April 2012 computer modeling; exercise; blood pressure; circulation; oxygen delivery SHORTNESS OF BREATH, FATIGUE, dizziness, and syncope are symptoms related to severe pulmonary hypertension (PH). These symptoms probably originate from decreased capacity to increase right ventricular (RV) and, hence, left ventricular (LV) output during exercise (10). On the basis of clinical observations that PH patients with a patent foramen ovale, allowing blood flow from the right to the left atrium (LA), have better life expectancy (3, 18), severe PH patients without this opening often undergo atrial septostomy (AS) to artificially create an atrial septal defect (ASD) (Fig. 1). After this procedure, symptoms of severe PH diminish and survival is prolonged (10). The beneficial effects of AS for PH patients are ascribed to 1) volume unloading of the RV, 2) facilitated LV filling, 3) increased systemic output in rest and the possibility to further increase systemic output during exercise to maintain Address for reprint requests and other correspondence: Y. Koeken, Dept. of Biomedical Engineering, Maastricht Univ., P.O. Box 616, 6200 MD, Maastricht, The Netherlands (e-mail: [email protected]). H2654 cerebral blood pressure, and 4) increased oxygen delivery to the peripheral tissues (3, 8 –10, 19, 23). It should be noted, however, that the ASD causes mixing of oxygenated pulmonary venous blood with low saturated systemic venous blood in the LA. As a result, arterial oxygen saturation is reduced (8, 14, 17, 19, 22). In clinical trials it was found that the relative decrease in arterial oxygen saturation was less than the relative increase in systemic output. Hence, it was concluded that systemic oxygen delivery, defined as systemic flow multiplied by the arterial oxygen saturation, was increased (17, 19). It is believed that the improvement of the patient’s condition after AS is explained by this increase in systemic oxygen delivery (6, 10, 17, 19, 23). However, because venous oxygen saturation is not increased in PH patients after AS (4), improvement of the patient may not be the result of increased oxygen delivery. It has also been suggested that the improvement of the patient’s condition and the relief of syncope may be ascribed to conservation of systemic blood pressure during exercise. The additional filling of the LV through the ASD facilitates the mandatory increase in systemic flow to maintain cerebral blood pressure during exercise (4, 12). To the best of our knowledge, it is still unclear whether the benefits of AS in PH patients are explained by the increase of oxygen availability in the tissues, the possibility to maintain blood pressure during exercise, or a combination of these factors. In the present study, we evaluated effects of AS using a multiscale computational model of the cardiovascular system (1, 13). Variations of the degree of PH, amount of pulmonary flow, and ASD size were simulated to investigate whether their effects on hemodynamics and oxygen distribution may explain the beneficial effects of AS in severe PH. Additionally, hemodynamics were evaluated in severe PH patients during exercise before and after AS. METHODS We applied the multiscale CircAdapt model of the cardiovascular system to investigate the effects of AS on hemodynamics and oxygen distribution in severe PH. The CircAdapt model enables simulation of beat-to-beat dynamics of the four cardiac cavities and the systemic and pulmonary circulations (1, 13). It comprises myocardial walls, large blood vessels, peripheral resistances, and cardiac valves. Mechanical ventricular interaction is accounted for by relating global ventricular pump mechanics to local myofiber mechanics in the three ventricular walls, i.e., the LV free wall, the interventricular septum, and the RV free wall (13). In each wall, the myofiber stress-strain relation is determined by a three-element Hill model that describes active and passive cardiac myofiber mechanics (13), including the Frank-Starling relation. An important characteristic of the CircAdapt model is the reduced number of required input parameters, which is achieved by adaptation of cardiac and vascular wall size and mass to mechanical load (2). More specifically, parameters describing cardiac 0363-6135/12 Copyright © 2012 the American Physiological Society http://www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.2 on June 16, 2017 Koeken Y, Kuijpers NH, Lumens J, Arts T, Delhaas T. Atrial septostomy benefits severe pulmonary hypertension patients by increase of left ventricular preload reserve. Am J Physiol Heart Circ Physiol 302: H2654 –H2662, 2012. First published April 27, 2012; doi:10.1152/ajpheart.00072.2012.—At present, it is unknown why patients suffering from severe pulmonary hypertension (PH) benefit from atrial septostomy (AS). Suggested mechanisms include enhanced filling of the left ventricle, reduction of right ventricular preload, increased oxygen availability in the peripheral tissue, or a combination. A multiscale computational model of the cardiovascular system was used to assess the effects of AS in PH. Our model simulates beat-to-beat dynamics of the four cardiac chambers with valves and the systemic and pulmonary circulations, including an atrial septal defect (ASD). Oxygen saturation was computed for each model compartment. The acute effect of AS on systemic flow and oxygen delivery in PH was assessed by a series of simulations with combinations of different ASD diameters, pulmonary flows, and degrees of PH. In addition, blood pressures at rest and during exercise were compared between circulations with PH before and after AS. If PH did not result in a right atrial pressure exceeding the left one, AS caused a left-to-right shunt flow that resulted in decreased oxygenation and a further increase of right ventricular pump load. Only in the case of severe PH a right-to-left shunt flow occurred during exercise, which improved left ventricular preload reserve and maintained blood pressure but did not improve oxygenation. AS only improves symptoms of right heart failure in patients with severe PH if net right-to-left shunt flow occurs during exercise. This flow enhances left ventricular filling, allows blood pressure maintenance, but does not increase oxygen availability in the peripheral tissue. H2655 ATRIAL SEPTOSTOMY IN PULMONARY HYPERTENSION d关O2兴LA dt ⫽ 1 共max共0, QPV兲 · 共关O2兴PV ⫺ 关O2兴LA兲 VLA (2) ⫹ max共0, QSHUNT兲 · 共关O2兴RA ⫺ 关O2兴LA兲 ⫹ max共0, QMV兲 · 共关O2兴LV ⫺ 关O2兴LA兲兲 S O2 ⫽ Fig. 1. Schematic overview of the circulation with a right-to-left shunt. LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; QS, systemic blood flow; QP, pulmonary blood flow; QRL, right-to-left shunt blood flow through the atrial septal defect (ASD); V̇O2, total oxygen consumption by the body. In contrast with carbon dioxide removal and oxygen uptake and delivery that are determined by the effective pulmonary flow (location A), the delivery of nutrients (location B) and the removal of metabolic waste products (location C) are determined by systemic flow. Part of the venous return is redirected through the ASD directly to the left atrium, thereby bypassing the pulmonary circulation (dashed line). [Adapted with permission from Diller et al. (4).] and vessel mechanics are adapted to obtain physiological stresses and strains. More detailed theoretical descriptions of the CircAdapt and TriSeg model have been published previously (1, 2, 13). Specific input parameters used in this study are shown in Table 1. Oxygen distribution model. The hemodynamic pressure difference over the ASD determines the magnitude and direction of blood flow between the atria. Thus ASD flow in healthy persons will be from left to right. However, in severe PH, ASD flow reverses due to the high right atrial pressure. As a result, poorly saturated blood from the right atrium (RA) and highly saturated blood from the pulmonary veins are mixed in the LA. The dynamic behavior of the CircAdapt model allows blood to move in both directions through all cavities and vessels during the complete cardiac cycle. Mixing of flows with different oxygen concentrations in a cavity is described by: d关O2兴CAV dt ⫽ 1 VCAV n max共0, Qi兲共关O2兴i ⫺ 关O2兴CAV兲 兺i⫽1 关 O 2兴 K · 关Hb兴 · 100% Oxygen uptake in the lungs was assumed to render an oxygen saturation of 98% in the pulmonary veins (5, 7). The oxygen consumption in the systemic tissue was set equal to the oxygen consumption of an adult male (70 kg) in rest (300 ml/min; Refs. 4, 21). Simulation setup. In the normal circulation, stroke volume was set to 85 ml and heart rate to 70 beats/min, resulting in a cardiac output of 5.95 l/min. The pulmonary resistance (Rpulm) was 18 MPa s/m3 [2.3 Wood units (WU)]. To mimic chronic compensated PH, the vascular and cardiac wall masses and cardiac cavity volumes were adapted to a pulmonary resistance of 60 MPa s/m3 (7.6 WU). Further increase in pulmonary resistance in absence of structural adaptation will lead to decompensated PH, clinically characterized by decreased pulmonary flow. To simulate decompensated PH, pulmonary flow (Qp) was reduced to 2.8 l/min by limiting RV stroke volume to 40 ml, while the pressure difference between the pulmonary artery and LA was set at 14 kPa (105 mmHg). This resulted in further increase of the pulmonary resistance to 340 MPa s/m3 (46 WU; Ref. 11). To mimic AS, a connection with an adjustable diameter was created between the two atria. To assess the effect of AS on systemic flow (Qs) and oxygen delivery in PH, variations in ASD diameters (0 –16 mm), pulmonary flows (40, 50, 60 ml/s), and degrees of PH (Rpulm; 80 –340 MPa s/m3; 11– 46 WU) were simulated. Systemic flow was defined as the summation of flow through the ASD and predefined pulmonary flow. Arterial oxygen saturation was calculated from the oxygen concentrations in the systemic arteries. The systemic venous saturation was calculated from the oxygen concentration in the systemic veins. The set of differential equations describing pressure, volume, and oxygen Table 1. Input parameters Value (1) with Qi positive for inflow and negative for outflow, [O2]CAV the oxygen concentration in the cavity, [O2]i oxygen concentration of the inflow, and n the number of flows entering the cavity with volume VCAV. As defined by Eq. 1, the oxygen concentration in a cavity depends only on the inlet blood flow sizes and oxygen concentrations. When Eq. 1 is applied to the LA in a patient with right-to-left shunt flow it results in: (3) Parameter Mean systemic arterial blood pressure, mmHg Mean pulmonary arteriovenous pressure drop, mmHg Mean systemic blood flow, ml/s Cardiac cycle time, s Rest Compensated PH 92 92 11 85 0.85 37.5 85 0.85 PH, pulmonary hypertension. AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00072.2012 • www.ajpheart.org Decompensated PH 92 105 40 0.85 Downloaded from http://ajpheart.physiology.org/ by 10.220.33.2 on June 16, 2017 where [O2]LA is left atrial oxygen concentration and VLA the left atrial blood volume, QPV is blood flow entering the LA from the pulmonary veins with oxygen concentration [O2]PV, QSHUNT is blood flow entering the LA through the ASD with oxygen concentration [O2]RA, and QMV is blood leaving the LA through the mitral valve with oxygen concentration [O2]LA. In case of mitral regurgitation, QMV is negative and contains LV oxygen concentration [O2]LV. The oxygen distribution model is applied to the four cardiac cavities and the systemic and pulmonary arteries and veins. Oxygen saturation (SO2) in the blood is determined by the oxygen concentration ([O2]) and the capacity of blood to carry oxygen. Transport capacity of blood for oxygen depends on hemoglobin concentration ([Hb]), set to 9.4 mol Hb/m3 (15 g/l), and its capacity to carry oxygen (, 4 mol O2/mol Hb; Refs. 4, 20). The oxygen saturation in a cavity is calculated from the oxygen concentration as follows: H2656 ATRIAL SEPTOSTOMY IN PULMONARY HYPERTENSION RESULTS Pressure-volume relations (PV-loops) for both the LV and RV are shown in Fig. 2 under normal circumstances (A), compensated PH (B), decompensated PH (C), decompensated PH with decreased pulmonary flow (D), and decompensated PH with decreased pulmonary flow with an ASD of 14 mm in diameter (E). Figure 2A shows the LV and RV pressure-volume relations for the normal healthy circulation, with high pressures (125 mmHg) generated by the LV and lower pressures (25 mmHg) by the RV. Cardiac output and heart rate were set to normal values at a systemic flow of 5.95 l/min with 70 beats/min, respectively. In Fig. 2B, cardiac mechanics of compensated PH with a pulmonary resistance of 60 MPa s/m3 (7.6 WU) is shown. Compensated PH was associated with increase of RV systolic pressure (⫹105%) compared with the normal circulation (Fig. 2A) and with ⬃120% increase of RV wall volume. A shift of the RV pressure-volume relation to higher RV cavity volumes was observed. End-diastolic RV cavity volume increased from 120 up to 140 ml and end-systolic volume increased from 48 to 66 ml. The area enclosed by the RV pressure-volume relation, representing external stroke work generated by the RV, was increased compared with normal. Decompensated PH (Fig. 2C) showed further increase of endsystolic and end-diastolic RV cavity volumes to 163 and 248 ml, respectively, and an increase of RV peak pressure from 26 to 134 mmHg. Severely decompensated PH is shown in Fig. 2D, where pulmonary flow was limited to 2.8 l/min and Rpulm was 340 MPa s/m3 (46 WU). The reduction of pulmonary flow, hence RV stroke volume, resulted in a decrease of workload for the RV with 65% compared with the RV workload of the RV in decompensated PH (Fig. 2C). Ventricular pressurevolume relations after the creation of an ASD with a diameter of 14 mm in decompensated PH are shown in Fig. 2E. This simulation demonstrated that the ASD enables right-to-left shunting, causing increased mitral valve flow. As a result, LV end-diastolic volume was increased from 84 ml before AS to 91 ml after AS. Since end-systolic volume remained unchanged, LV stroke volume increased from 40 to 47 ml, thereby increasing systemic outflow from 2.8 to 3.3 l/min. Stroke work as generated by the LV was increased with 19% and RV peak pressure remained relatively unaffected by AS. Subsequently, systemic flow (Fig. 3, A–C) and arterial oxygen saturation (Fig. 3, D–F) were studied for combinations of different pulmonary resistances (Rpulm), pulmonary flows (Qp), and ASD diameters. Figure 3, A and D, shows the systemic flow and arterial oxygen saturation for a circulation with an ASD of 8 mm in diameter. A constant Qp in combination with an increase in Rpulm resulted in an increase of systemic flow (Fig. 3A) and a decrease of arterial saturation (Fig. 3D). The grey shaded area denotes simulations with right-to-left shunt flow. The lower border of this area indicates the critical resistance (Rcrit) at which Qs and Qp are equal, i.e., net shunt flow is zero. If Rpulm is smaller than Rcrit, the shunt flow across the ASD will be left-to-right, and, consequently, Qs will decrease. Rcrit was dependent on Qp; for Qp of 60, 50, and 40 ml/s, Rcrit was 180 MPa s/m3 (23 WU), 230 MPa s/m3 (29 WU), and 290 MPa s/m3 (37 WU), respectively. It should also be noted that Rcrit increased with increasing ASD size (Fig. 3, A–C). Figure 3D shows that for Qp of 40 ml/s, decrease of arterial oxygen saturation occurred at higher Rpulm compared with a Qp of 60 ml/s. Figure 3, D–F, shows arterial oxygen saturation in relation to Rpulm and pulmonary flow (Qp) for three different ASD diameters. With increasing ASD diameter, arterial oxygen saturation decreased in decompensated PH. Shunt direction. Figure 4 shows the systemic flow as well as the arterial and venous oxygen saturation as a function of ASD diameter for three different values of Qp in a circulation with a left-to-right shunt (Rpulm⬍ Rcrit; Fig. 4, A–C) and a right-to-left shunt (Rpulm ⬎ Rcrit; Fig. 4, D–F). Qp was kept constant at 60, 50, and 40 ml/s, respectively, while Qs was allowed to increase or decrease as a result of shunt flow. If the systemic flow decreased due to left-to-right shunt flow (Fig. 4A), arterial Fig. 2. Pressure volume relations (PV-loop) A: normal (Qp ⫽ 85 ml/s, Qs ⫽ 85 ml/s, and Rpulm ⫽ 18 MPa s/m3). B: compensated pulmonary hypertension (PH; Qp⫽ 85 ml/s, Qs ⫽ 85 ml/s, and Rpulm ⫽60 MPa s/m3). C: decompensated PH (Qp ⫽ 85 ml/s, Qs ⫽ 85 ml/s, and Rpulm ⫽ 165 MPa s/m3). D: severe decompensated PH with decreased cardiac output (Qp ⫽ 40 ml/s, Qs ⫽ 40 ml/s, and Rpulm ⫽ 340 MPa s/m3). E: same as D, with an ASD of 14 mm in diameter (Qp ⫽ 40 ml/s, Qs ⫽ 47 ml/s, and Rpulm ⫽ 340 MPa s/m3). AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00072.2012 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.2 on June 16, 2017 concentration was solved using the MATLAB ode113 solver (The Mathworks, Natick, MA). Oxygen saturations were averaged over time within one cardiac cycle. Hemodynamic steady state was achieved within 100 cardiac cycles. Simulating exercise. Exercise was simulated in a circulation with decompensated PH by incrementally reducing systemic peripheral resistance, down to 50% of its normal resting value, while keeping pulmonary resistance constant. Regulation of blood pressure by venoconstriction and renal retention are both included in the model. The total blood volume in a subject can be divided into two volume partitions, which are stressed and unstressed blood volume. Stressed blood volume is defined as the volume of blood that must be removed from the vasculature to decrease the transmural pressure of the vessels from the existing value to zero (16). Unstressed volume, i.e., the volume of blood in the vessels at zero transmural pressure, is disregarded in the model. Venoconstriction was modeled by lumping recruitment of unstressed volume into increase of stressed blood volume. Renal retention increases total circulating blood volume and, hence, also stressed blood volume. Heart rate was allowed to increase linearly up to 140 beats/min. Adaptation of the cardiac walls to the increased hemodynamic load was disregarded. Simulations with and without ASD of 16 mm were performed. ATRIAL SEPTOSTOMY IN PULMONARY HYPERTENSION H2657 oxygen saturation (Fig. 4B) also slightly decreased. Venous oxygen saturation (Fig. 4C) decreased with decreasing Qp and with increasing ASD size. In the presence of a right-to-left shunt, systemic output increased with shunt flow. The shunt flow increased proportionally with increase of ASD diameter and Qp (Fig. 4D). Arterial oxygen saturation decreased proportionally with increase of ASD diameter (Fig. 4E) due to mixing of oxygen poor and rich blood in the LA. Venous oxygen saturation showed to be proportionally related to Qp and to be independent of ASD size (Fig. 4F). Exercise. In Fig. 5, simulations in which systemic resistance incrementally decreased to 50% of Rsys in rest, are shown for circulations with and without ASD. The two most extreme situations are presented. Figure 5, B and E, shows the results of simulations with maintenance of mean systemic arterial pressure only by means of increased stressed volume and, hence, Fig. 4. Venous and arterial oxygen saturation for 3 different pulmonary flows (Qp; dotted: 40 ml/s; dashed: 50 ml/s; and solid: 60 ml/s) with a constant oxygen consumption for different ASD diameter with a left-to-right shunt flow (Rpulm ⬍ Rcrit; top) and a right-to-left shunt flow (Rpulm ⬎ Rcrit;, bottom). Pulmonary flow is kept constant resulting in decreased systemic flow in a left-to-right shunt flow and increased systemic flow with right-to-left shunt flow. Systemic flow decreases for larger ASDs in left-to-right shunting and increases with right-to-left shunting for increasing ASD diameter (A and D). Arterial oxygen saturation shows decrease in both cases as dynamic mixing of blood is allowed (B and E). Venous oxygen saturation appears to be related to ASD size for Rpulm ⬍ Rcrit, unrelated to ASD size for Rpulm ⬎ Rcrit, and related to Qp regardless of shunt flow direction (C and F). AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00072.2012 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.2 on June 16, 2017 Fig. 3. Systemic flow (A–C) and arterial oxygen saturation (D–F) in relation to pulmonary resistance (Rpulm) and pulmonary flow (Qp) for ASD diameter 8 mm (A and D), 12 mm (B and E), and 16 mm (C and F). Grey shadow area indicates occurrence of right-to-left shunt flow. H2658 ATRIAL SEPTOSTOMY IN PULMONARY HYPERTENSION Downloaded from http://ajpheart.physiology.org/ by 10.220.33.2 on June 16, 2017 Fig. 5. Aortic valve flow (QAO) and pressures in the aorta (pAO) and left ventricle (pLV) for patient without (A–C) and with an ASD (D–F) while systemic resistance was decreased to 95% (A and D) or 50% (B, C, E, and F) of its value at rest. Heart rate (HR)was kept constant at 70 beats/min (A, B, D, and E) and was increased to 140 (C and F). G: stressed blood volume increase in relation to the decrease in systemic resistance for simulations without and with ASD. Solid lines indicate simulations with a constant heart rate of 70 beats/min and dashed lines with an increasing heart rate (Table 2). Increase of left ventricular contractility resulted in a decrease of stressed volume. increased stroke volume. Figure 5, C and F, shows results of simulations with maintenance of mean systemic arterial pressure by increase of heart rate up to 140 beats/min. In the presence of an ASD, increase in stressed blood volume and, hence, of systemic venous pressure, was present, but not as abundant as in the simulations without an ASD (Fig. 5G and Table 2). Due to the increased RV preload, pulmonary flow in the simulations with ASD increased up to 130% if systemic resistance was reduced to 50% of its value at rest. The combination of increased systemic venous pressure and decreased AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00072.2012 • www.ajpheart.org H2659 ATRIAL SEPTOSTOMY IN PULMONARY HYPERTENSION Table 2. Simulated values for flows, pressures, and volumes in rest and during exercise No ASD Rest 100 50 50 0 70 1.00 109 80 2 92 98 193 115 2 2 300 98 49 298 98 50 Exercise 90.0 55 55 0 84 1.04 108 79 2 92 109 206 125 2 2 300 98 53 331 98 50 70 69 69 0 112 1.23 109 79 3 92 137 254 153 5 3 300 98 63 415 98 50 Rest 50 86 86 0 140 1.64 112 78 6 92 173 338 188 15 7 300 98 70 514 98 50 100.0 50 52 ⫺2 70 1.00 109 77 2 92 98 191 114 2 2 300 93 47 313 93 45 Exercise 90.0 53 58 ⫺5 84 1.01 109 78 2 92 104 196 119 2 2 300 93 51 347 92 44 70.0 59 74 ⫺15 112 1.08 110 78 2 92 116 210 125 3 3 300 93 60 444 90 42 50.0 66 98 ⫺32 140 1.25 114 76 4 92 134 239 148 5 5 300 90 65 589 82 34 ASD, atrial septal defect; Qp, pulmonary flow; Qs, systemic flow; QASD, shunt flow; HR, heart rate; V, normalized stressed blood volume; SBP, systemic blood pressure; DBP, diastolic blood pressure; CVP, central venous pressure; MAP, mean arterial pressure; pPA, pulmonary artery pressure; EDVRV, right ventricular end-diastolic volume right ventricle; pRV, systolic right ventricular pressure; pRA, right atrial pressure; pLA, mean left atrial pressure; V̇O2, oxygen consumption; Art. sat., mean arterial oxygen saturation; Ven. sat., mean venous oxygen saturation. systemic resistance led to an increase in right-to-left shunt flow across the ASD. The ASD flow was responsible for 70% of the almost twofold increase in systemic flow needed in simulations with 50% decreased systemic resistance. The exponential relation between stressed blood volume and systemic resistance is steeper for the simulations without ASD compared with the ones with ASD (Fig. 5G). In the absence of an ASD, decrease of Rsys and, hence, in mean systemic arterial pressure was mainly compensated for by an increase in stressed blood volume, leading to increased systemic venous pressure. On the one hand, this increased systemic venous pressure will lower the pressure difference across the peripheral circulation. Consequently, a smaller increase in systemic output is needed to maintain systemic arterial pressure in case of a decreased systemic resistance. On the other hand, the increased systemic venous pressure will lead to an increased RV preload and, hence, increased pulmonary flow. In a circulation without an ASD, increase of heart rate resulted in a large increase of stressed volume. However, the increase of stressed blood volume was less than in a simulation with constant heart rate (Fig. 5, C, F, and G, dotted line). In a circulation with an ASD, stressed blood volume did not differ between simulations with constant and increased heart rate. The effect of increased LV contractility on the reduction of stressed blood volume increase was limited. A twenty-five percent increase in active stress generation resulted in 1% reduction of the stressed volume increase in a circulation without ASD, while the reduction was 4% in a circulation with ASD. Although systemic arterial pressure could be maintained in simulations without an ASD, it can be appreciated, both from Table 2 and Fig. 5, that this process is accompanied by an increase of stressed blood volume of ⬎30%, which is above values mentioned in literature (15, 16). DISCUSSION The CircAdapt model of the human heart and circulation has been extended with an oxygen distribution model. The resulting model has been used to evaluate the effect of AS on both hemodynamics and oxygen transport in patients with severe PH. In our simulations, the direction of shunt flow was dependent on both pulmonary flow and resistance. Shunt flow direction reversed when pulmonary vascular resistance (Rpulm) exceeded a critical value, Rcrit. This critical resistance value had a distinct inverse proportional relation with pulmonary flow (Qp) and was not related to ASD size. Although arterial oxygen saturation was drastically decreased by right-to-left shunt flow, venous oxygen saturation did not change, suggesting similar oxygen delivery to the tissue. Simulations of exercise with severe PH in which pulmonary resistance exceeds Rcrit showed that these PH patients benefit from an ASD because right-toleft atrial shunt flow facilitates maintenance of systemic arterial pressure. Shunt direction. Most patients with severe PH suffer from syncope, fatigue, and right heart failure (10). The presence of right heart failure suggests that the RV is working at maximal capacity in these patients. We therefore assumed that pulmonary flow and pulmonary vascular resistance do not change after AS and retain their maximal value. In contrast, the systemic flow could change in our simulations, enabling investigation of the effect of AS on systemic flow. ASD flow direction is determined by the pressure difference between the RA and LA, whereas amount of flow is determined by ASD size and the pressure difference across the ASD. Normally, LA pressure exceeds RA pressure and an ASD will result in a left-to-right shunt flow and an increased pulmonary flow with respect to the systemic flow. In a PH AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00072.2012 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.2 on June 16, 2017 Exercise, %Rsys Qp, ml/s Qs, ml/s QASD, ml/s HR, beats/min V, ⫺ SBP, mmHg DBP, mmHg CVP, mmHg MAP, mmHg pPA, mmHg EDVRV, ml pRV, mmHg pRA, mmHg pLA, mmHg V̇O2 constant, ml/min Art. sat., % Ven. sat., % V̇O2 variable, ml/min Art. sat., % Ven. sat., % ASD 16 mm H2660 ATRIAL SEPTOSTOMY IN PULMONARY HYPERTENSION Fig. 6. Oxygen transport in a circulation with a constant pulmonary flow of 2.5 l/min, constant oxygen consumption (V̇O2; 0.2 mmol/s), and right-to-left shunt flow through the ASD. Systemic oxygen transport (SOT) increases with increasing systemic flow (line B, corresponding with location B in Fig. 1), but also more oxygen is returned to the heart through the venae cavae (venous return; line C, corresponding with location C in Fig. 1). The amount of oxygen that can be used by the systemic tissue, the effective systemic oxygen transport (SOTeff), is unchanged (line A, corresponding with location A in Fig. 1). will be the sum of Qs and the left-to-right shunt flow. In the presence of a right-to-left shunt, desaturated blood will bypass the pulmonary vascular bed and Qs will be the sum of Qp and the right-to-left shunt flow. Therefore, using Qs as a representative of the amount of blood passing through the lungs that can be oxygenated, is incorrect. We should look for the quantity of systemic venous blood that is directed to the pulmonary circulation and oxygenated, the so-called effective pulmonary flow (Qep). Consequently, the effective systemic oxygen transport capacity (SOTeff) should be defined as the product of Qep and pulmonary venous saturation. SOTeff can be applied to both normal circulations and those with shunts. Reduction of RV preload, which will occur during right-to-left shunt flow, will not result in an increase in Qep. Although SOT will increase in this situation, SOTeff will definitely not increase (Fig. 6). Relieve of symptoms and the increase in exercise capacity in PH patients after AS can therefore not be explained by changes in oxygen distribution. Nutrients and metabolic waste products transport. In contrast with oxygen uptake and delivery that are determined by the effective pulmonary flow, the delivery of nutrients (Fig. 1, location B) and the removal of metabolic waste products (Fig. 1, location C) are determined by systemic flow. Therefore, an increase in systemic flow, induced by a right-to-left shunt flow through the ASD, may ameliorate the condition in the patient by improved delivery of nutrients and increased removal of accumulated waste products. However, removal of carbon dioxide still remains dependent on effective pulmonary flow (Fig. 1, location A). Exercise. Systemic arterial blood pressure is maintained during exercise, because the decrease in systemic vascular resistance will be compensated for by an increase in systemic blood flow. In severe PH, however, increase of systemic output is restricted due to the incapability of the RV to further increase pressure and, hence, pulmonary flow through the highly resistant pulmonary vasculature. In these patients, resting heart rate and finally stressed blood volume are increased to enlarge venous return to the heart to maintain systemic arterial blood pressure. Increase in stressed blood volume by venoconstriction and by renal retention are both included in the model. In the absence of an ASD, a larger increase in stressed blood volume is needed to compensate for the decrease in systemic resistance and subsequent arterial pressure drop. The increase in stressed blood volume is, however, not infinite. Considering a healthy person with a total blood volume of 80 ml/kg, ⬃30% (25 ml/kg) of this total volume is stressed volume (16). Venoconstriction can mobilize 7.5 ml/kg blood from the unstressed blood volume and increase stressed volume to maintain blood pressure (15). Therefore, an increase of stressed volume up to 30% is supposed to be reasonable. In a circulation without an ASD, maximal recruitment of blood volume will occur at lower exercise levels than in a circulation with an ASD (Fig. 5). Once PH patients without ASD start to exercise, they reach either the limit of their capacity to increase their stressed blood volume acutely, or the RV will be pushed towards its limits with respect to cavity volume or pressure generation (Table 2). Consequently, blood pressure will drop and the patient will suffer from dizziness or fainting. After AS, the PH patient will be able to increase systemic output without the need of maximal blood volume recruitment. Systolic blood pressure will increase during exercise because LV stroke volume is in- AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00072.2012 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.2 on June 16, 2017 patient, an ASD will only result in right-to-left shunt flow, when the PH is severe enough (6), so that RA pressure exceeds LA pressure (Figs. 3 and 4). Due to right-to-left shunt flow, systemic blood flow will increase, albeit that systemic arterial blood oxygen content is reduced due to mixing of oxygen rich and poor blood in the atria (Fig. 4E). Although zero net shunt flow is hemodynamically unimportant because Qs and Qp remain unchanged, it can reduce systemic arterial oxygen saturation (Fig. 3, D–F). Dynamic movement of blood from left-to-right and vice versa allows oxygen rich and oxygen poor blood to mix in the atria. This mixing will increase oxygen saturation in the RA, but it will also reduce LA saturation and, hence, arterial oxygen saturation (Fig. 3D). Conceivably, arterial oxygen saturation cannot be used to quantify right-to-left shunt flow, as is common clinical practice. To estimate net shunt flow and direction in the clinical setting, we therefore recommend to use additional measurements, for example of LV end-diastolic volume or pressure, as done by Sandoval et al. (19). Oxygen availability. Systemic oxygen transport (SOT) is defined as systemic flow multiplied by the systemic arterial oxygen saturation (Fig. 6). SOT defined as such will increase in the presence of a right-to-left shunt after AS in severe PH patients, because the decrease in arterial oxygen saturation is overcompensated for by the increase in systemic flow (6, 10, 14, 17, 19, 23). However, the systemic venous blood that passes through the shunt will travel round the circulation and arrive back at the RA with the same oxygen content and, therefore, will not add to the capacity to transport oxygen into the tissue (12). In a normal circulation, the pulmonary and systemic circulations are connected in series and, hence, Qp and Qs are equal and interchangeable. In the presence of a left-to-right shunt, oxygenated blood will bypass the systemic vascular bed and Qp H2661 ATRIAL SEPTOSTOMY IN PULMONARY HYPERTENSION Table 3. Simulations results compared with clinical data from literature No ASD Present Simulation Kerstein et al. (10) Simulation Kurzyna et al. (11) Kerstein et al. (10) Means Means SD Means SD Means Means SD Means SD 3.0 3.0 0 70 109 80 2 92 98 115 2 2 300 98 49 15 2.5 2.5 0 — — — — — 62.1 — 15.2 4.0 — 93 42 14.8 0.8 0.8 0 — — — — — 17.5 — 7.0 3.5 — 3 5 2.9 — — 0 — — — — 91.9 68.8 — 11.2 4.8 — 97.4 — 15.3 — — 0 — — — — 14.2 22.1 — 7.1 2.6 — 1.7 — 1.6 3.0 3.1 0.1 70 109 77 2 92 98 114 2 2 300 93 47 15 2.4 3.0 0.6 — — — — — 66.2 — 14.4 4.3 — 84.0 — — 0.9 1.1 0.3 — — — — — 17.9 — 5.9 4.1 — 3.8 — — — — — — — — — 90.2 71.9 — 10.0 7.3 — 89.0 — 14.8 — — — — — — — 16.1 23.7 — 4.3 2.8 — 7.1 — 2.5 Hb, hemoglobin concentration. creased. The increase in systemic flow is facilitated by the blood flow through the ASD, which abolishes the preload restriction of the LV (Fig. 5). PH patients with Rpulm close to Rcrit in rest may benefit by AS during exercise, because shunt direction may reverse due to decrease of systemic resistance. As discussed above, blood passing right-to-left through the ASD has low oxygen saturation and therefore will not contribute to additional oxygen delivery to the tissue. Over the long term, however, the decreased arterial oxygen saturation might induce hemoglobin production (10, 12). Although the resultant increased hemoglobin levels will increase the capacity of blood to carry oxygen, it will also increase blood viscosity, resulting in higher workload for the ventricles and increased risk of thrombosis. Clinical relevance of model simulations. As compared with a previous modeling study in this field (4), the present study uses a multiscale model of cardiovascular system dynamics that relates global pulmonary and systemic hemodynamics to pump mechanics of the cardiac chambers and to local mechanics of the constituting myocardial tissue being responsible for the pumping action of the heart. It allows for increase of stressed volume by venoconstriction during exercise. The characteristics of the systemic and pulmonary circulation could be adjusted to simulate various degrees of pulmonary hypertension and exercise. Moreover, the CircAdapt model gives insight in volumes and pressures which are mostly inaccessible in patients. Table 3 shows the results of the simulations and clinical data from literature (10, 11). Overall, simulated pressures and volumes are in agreement with clinical data. However, it should be mentioned that simulated mean RA pressure is low and mean pulmonary artery pressure is high compared with corresponding clinical data. Since atrial pressure is directly related to diastolic ventricular pressure, low RA pressure implies low diastolic RV pressure. This suggests that the RV is more compliant in the model than in severe PH patients. High pulmonary artery pressure suggests a strong RV that is able to produce high pressures. Despite these quantitative differences, the qualitative effects of AS on cardiovascular function in our simulations are in agreement with clinical findings. Simulating a less compliant and weaker ventricle would not change these qualitative effects but only amplify effects quantitatively. Several clinical investigators evaluated atrial septostomy in severe PH patients (9 –11, 19). Modeling studies are less commonly used, although they can provide valuable mechanistic insights in cardiovascular function dynamics before and after atrial septostomy both in rest and in exercise. Our study shows that AS might only be beneficial to patients with severe PH and that this benefit originates from an increase of LV preload and not from an increase in oxygen delivery to the tissue, as stated in previous studies (6, 10, 17, 19, 23). These simulation results may lead to improved success rate of the procedure by improving patient selection and, hence, withholding the procedure to likely nonresponders. Ultimately, an inverse modeling approach, in which the model is personalized by fitting simulated hemodynamics to a set of patient-specific data, might facilitate patient selection for AS and prediction of outcome by simulation of the intended intervention. Conclusion. Our multiscale model of the cardiovascular system enables the exploration of the effects of AS in severe PH patients on oxygen distribution and cardiovascular mechanics. Atrial septostomy in PH patients results in a right-to-left shunt flow if pulmonary vascular resistance exceeds a critical value. This critical resistance value is inversely proportional with pulmonary flow and is hardly influenced by ASD size. Although right-to-left shunt flow does not lead to increased oxygen availability, the condition of a PH patient may improve because maintenance of systemic arterial pressure is facilitated during exercise. GRANTS This work was supported by the Dutch Heart Foundation Grant 2007B203. DISCLOSURES No conflicts of interest, financial or otherwise, are declared by the author(s). AUTHOR CONTRIBUTIONS Author contributions: Y.K., T.A., and T.D. conception and design of research; Y.K. performed experiments; Y.K., N.H.K., T.A., and T.D. analyzed AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00072.2012 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.2 on June 16, 2017 QP, l/min QS, l/min QASD, l/min HR, beats/min SBP, mmHg DBP, mmHg CVP, mmHg MAP, mmHg pPA, mmHg pRV, mmHg pRA, mmHg pLA, mmHg V̇O2, ml/min Art. sat., % Ven. sat., % Hb, g/dl Kurzyna et al. (11) ASD Present H2662 ATRIAL SEPTOSTOMY IN PULMONARY HYPERTENSION data; Y.K., N.H.K., J.L., T.A., and T.D. interpreted results of experiments; Y.K. and T.D. prepared figures; Y.K. and T.D. drafted manuscript; Y.K., N.H.K., J.L., T.A., and T.D. edited and revised manuscript; Y.K., N.H.K., J.L., T.A., and T.D. approved final version of manuscript. REFERENCES AJP-Heart Circ Physiol • doi:10.1152/ajpheart.00072.2012 • www.ajpheart.org Downloaded from http://ajpheart.physiology.org/ by 10.220.33.2 on June 16, 2017 1. Arts T, Delhaas T, Bovendeerd P, Verbeek X, Prinzen FW. Adaptation to mechanical load determines shape and properties of heart and circulation: the CircAdapt model. Am J Physiol Heart Circ Physiol 288: H1943– H1954, 2005. 2. Arts T, Lumens J, Kroon W, Delhaas T. Control of whole heart geometry by intramyocardial mechano-feedback: a model study. PLoS Comput Biol 8: e1002369, 2012. 3. Austen WG, Morrow AG, Berry WB. Experimental studies of the surgical treatment of primary pulmonary hypertension. J Thorac Cardiovasc Surg 48: 448 –455, 1964. 4. Diller GP, Lammers AE, Haworth SG, Dimopoulos K, Derrick G, Bonhoeffer P, Gatzoulis MA, Francis DP. A modelling study of atrial septostomy for pulmonary arterial hypertension, and its effect on the state of tissue oxygenation and systemic blood flow. Cardiol Young 20: 25–32, 2010. 5. Diller GP, Uebing A, Willson K, Davies LC, Dimopoulos K, Thorne SA. Analytical identification of ideal pulmonary-systemic flow balance in patients with bidirectional cavopulmonary shunt and univentricular circulation: oxygen delivery or tissue oxygenation? Circulation 114: 1243– 1250, 2006. 6. Galie N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA. Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J 30: 2493– 2537, 2009. 7. Guyton AC, Hall JE. Textbook of Medical Physiology (12th ed.). Philadelphia, PA: W. B. Saunders, 2011. 8. Hausknecht MJ, Sims RE, Nihill MR, Cashion WR. Successful palliation of primary pulmonary hypertension by atrial septostomy. Am J Cardiol 65: 1045–1046, 1990. 9. Keogh AM, Mayer E, Benza RL, Corris P, Dartevelle PG, Frost AE. Interventional and surgical modalities of treatment in pulmonary hypertension. J Am Coll Cardiol 54: S67–S77, 2009. 10. Kerstein D, Levy PS, Hsu DT, Hordof AJ, Gersony WM, Barst RJ. Blade balloon atrial septostomy in patients with severe primary pulmonary hypertension. Circulation 91: 2028 –2035, 1995. 11. Kurzyna M, Dabrowski M, Bielecki D, Fijalkowska A, Pruszczyk P, Opolski G. Atrial septostomy in treatment of end-stage right heart failure in patients with pulmonary hypertension. Chest 131: 977–983, 2007. 12. Lammers AE, Haworth SG, Diller GP. Atrial septostomy in patients with pulmonary hypertension: should it be recommended? Expert Rev Respir Med 5: 363–376, 2011. 13. Lumens J, Delhaas T, Kirn B, Arts T. Three-wall segment (TriSeg) model describing mechanics and hemodynamics of ventricular interaction. Ann Biomed Eng 37: 2234 –2255, 2009. 14. Micheletti A, Hislop AA, Lammers A, Bonhoeffer P, Derrick G, Rees P. Role of atrial septostomy in the treatment of children with pulmonary arterial hypertension. Heart 92: 969 –972, 2006. 15. Rothe CF. Point-counterpoint: active venoconstriction is/is not important in maintaining or raining end-diastolic volume and stroke volume during exercise and orthostasis. J Appl Physiol 101: 1262–1264, 2006. 16. Rothe CF. Reflex control of veins and vascular capacitance. Physiol Rev 63: 1281–1342, 1983. 17. Rothman A, Sklansky MS, Lucas VW, Kashani IA, Shaughnessy RD, Channick RN, Auger WR, Fedullo PF, Smith CM, Kriett JM, Jamieson SW. Atrial septostomy as a bridge to lung transplantation in patients with severe pulmonary hypertension. Am J Cardiol 84: 682–686, 1999. 18. Rozkovec A, Montanes P, Oakley CM. Factors that influence the outcome of primary pulmonary hypertension. Br Heart J 55: 449 –458, 1986. 19. Sandoval J, Gaspar J, Pulido T, Bautista E, Martinez-Guerra ML, Zeballos M. Graded balloon dilation atrial septostomy in severe primary pulmonary hypertension. A therapeutic alternative for patients nonresponsive to vasodilator treatment. J Am Coll Cardiol 32: 297–304, 1998. 20. Santamore WP, Barnea O, Riordan CJ, Ross MP, Austin EH. Theoretical optimization of pulmonary-to-systemic flow ratio after a bidirectional cavopulmonary anastomosis. Am J Physiol Heart Circ Physiol 274: H694 –H700, 1998. 21. Sherwood L. Human Physiology (6th ed.). Belmont, CA: Thomson Brooks/Cole, 2007. 22. Thanopoulos BD, Georgakopoulos D, Tsaousis GS, Simeunovic S. Percutaneous balloon dilatation of the atrial septum: immediate and midterm results. Heart 76: 502–506, 1996. 23. Zierer A, Melby SJ, Voeller RK, Moon MR. Interatrial shunt for chronic pulmonary hypertension: differential impact of low-flow vs. high-flow shunting. Am J Physiol Heart Circ Physiol 296: H639 –H644, 2009.