Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Drug discovery wikipedia , lookup
Drug design wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacognosy wikipedia , lookup
Neuropharmacology wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Drug interaction wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Urban legends about drugs wikipedia , lookup
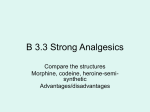
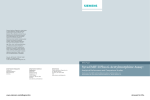
Journal of Analytical Toxicology, Vol. 21, October 1997 Case Report I Atypical Urinary Opiate Excretion Pattern* Leon R. Glass 1,2,~,Stephen T. IngaUsl, 3, Catherine L. Schilling 2, and Charles t. Hoppel 1,3 IResearch, 2pathology` and Laboratory Medicine Service, 113-B, Department of Veterans Affairs Medical Center, 10000 Brecksville Road, Brecksville, Ohio 44141 and 3Departments of Pharmacology and Medicine, Case Western Reserve University, Cleveland, Ohio 44106 [ Abstract I Heroin is rapidly metabolized in humans to 6-acetylmorphine (6-AM), which is further metabolized to morphine and morphine conjugates. Urinary 6-AM is the best diagnostic indicator of heroin abuse. This metabolite however, is usually present in urine at less than 3% of the concentration of urinary total morphine (MOR). We present two case studies of 43-year-old, apparently identical, male twins who displayed an atypical pattern of opiate metabolism. The subjects had a history of opiate abuse, and they are currently in a substance-abusetreatment program. Urine specimenssubmitted by these subjectsfor periodic clinical urine drug testing occasionally gave positive responsesfor opiates by enzyme immunoassay.These samples were then submitted for confirmation analysisusing a mixed-mode solid-phase extraction sample preparation, trimethylsilyl derivatization, and capillary gas chromatography--electron impact-massspectrometry confirmation analysis. These specimens contained as much as 2000 ng/mL of 6-AM with lessthan 350 ng/mL of MOR, which yielded 6-AM/MOR ratios as large as 1100%. Additional urine samples from these subjectsthat screened negative for opiates were also tested for the presence of 6-AM. Clinically significant concentrations of 6-AM were found in some of these samples. Introduction Illicit opiate use remains a major problem in North American society. Urine drug testing provides a tool for detecting users and for monitoring the compliance of subjects in recovery programs. The complex metabolic pathways of codeine, heroin (diacetylmorphine), and morphine complicate the interpretation of test results. Heroin is rapidly degraded to 6-acetylmorphine (6-AM) by both chemical and enzymatic processes. Heroin is labile in aqueous solutions, and deacylation is accelerated in biological fluids. In addition, there is extensive organ metabolism. The plasma half-life of heroin has been estimated at 2-8 rain (1-3). 6-AM is more stable than heroin; it undergoes conversion to * Data in this articlewere presentedin part at the annual meetingof the Societyof Forensic Toxicologistsin Denver,Colorado,October 1996. +Correspondenceshould be addressed to Leon R. Glass,Ph.D., PALMS113-B,VeteransAdministration MedicalCenter, 10000SrecksvilleRd., Brecksville,OH 44141, morphine by enzymatic and nonenzymatic deacylationwith an estimated plasma half-lifeof 10-40 rain (3,4). Morphine may be further metabolized by demethylation to normorphine, and both forms can be conjugated before excretion. Morphine and its metabolites are excreted as free and glucuronide or sulfate conjugates in bile, sweat, hair, and urine. Morphine glucuronide is normally the major urinary metabolite of heroin (5). Codeine is metabolized by demethylation to morphine or norcodeine and formation of conjugates. The rate of conversion of codeine to morphine varies widely among individuals. Subjects with an accelerated codeine metabolism pathway can produce urine specimens that are morphine positive with codeine concentrations below the cutoff after a codeine dose (6). Codeine is often present in the starting material for illicit heroin (7). Additionally,metabolic conversion of morphine to codeine has been reported (8). Thus, a user of heroin may produce a specimen that is positive for both codeine and morphine. Dietary sources of opiates, such as poppy seeds, further complicate the differentiation of hard-core drug abusers from the general population (1,9). These metabolic pathways are shown in Figure 1. Because of these complications, attention has lately been focused on morphine precursors. The extreme labilityof heroin limits its utility as a target analyte for routine abuse detection (5). 6-AM is considered the best marker for heroin use because there is no natural source, it is not a codeine metabolite, and it is comparativelystable relative to heroin (1,10,11). However, it is normally excreted in the first few hours following heroin use, is present in trace concentrations, and has limited chemical stability. The window of detection for 6-AMin urine is less than 8-h postdose (12). The concentration of 6-AMwas reported as approximately 1-3% of the concomitant total morphine (MOR) (13). The highest 6-AM/MORratio found in the literature was less than 8% (14). Experimental Materials Reagent-grade water was prepared by passage though a Millipore purification system. The primary standards, codeine, morphine, and 6-acetylmorphine, and the tri-deuterated Reproduction (photocopying) of editorial content of this journal is prohibited without publisher's permission. 509 Journal of Analytical Toxicology, Vol. 21, October 1997 analogues were obtained from Radian (Austin, TX). N,O-Bis(trimethylsilyl)trifluoroacetamide with 1% trimethylchlorosilane (BSTFA + TMCS) and derivatization-grade acetonitrile were purchased from Pierce Chemical (Rockford,IL). Oxycodone,oxymorphone, hydrocodone, hydromorphone, levorphanol, dextromethorphan, pentazocine, meperidine, normeperidine, dihydrocodeine, and 13-glucuronidase(Patella vulgata) were purchased from Sigma Chemical (St. Louis, MO). Mixed-modesolid-phase extraction (SPE) columns were obtained from United Chemical Technologies (Horsham, PA) and Radian. Sodium phosphate (dibasic), potassium phosphate (monobasic), sodium acetate, methanol, and acetonitrile were bought from J.T. Baker (Phillipsburg, NJ). All other solvents and reagents were of analytical grade. Standard solutions The working calibrator for the codeine/morphine quantitative assay was prepared by fortifying drug-free urine to 300 ng/mL for each drug. Positive quality control solution was prepared in a similar manner. Aliquots of these solutions were stored at-70~ until needed, thawed before use, and stored at 4~ until the supply was exhausted. Deuterated internal standard solution was prepared in reagent-grade water. Secondary standards for the 6-AM quantitative calibrator and quality control were prepared in acetonitrile at 1.0 and 1.25 mg/mL, respectively. Secondary standard aliquots were stored at -70~ until needed, thawed before use, and then stored at -20~ until consumed. Working calibrator and positive quality control were prepared on the day of assay by adding 100 p.L of the secondary standards to separate 5-mL aliquots of drugfree urine to yield concentrations of 20-ng/mL calibrator, and 25-ng/mL positive quality control. Mixtures of reference materials were prepared for use as qualitative scan standards. Mixture I contained meperidine, normeperidine, dextromethorphan, levorphanol, oxycodone, oxymorphone, and hydrocodone. Mixture II contained penta- Equipment The sample preparation system included a vacuum manifold (Supelco, Bellefonte, PA) for SPE and a Reacti-Vap III evaporator and heating block (Pierce) for eluant evaporation. The chromatographic system consisted of a model 5890 series II gas chromatograph (GC) equipped with a model 7673 autoinjector coupled to a model 5971A quadrupole mass selective detector, all of which were from Hewlett Packard (Avondale,PA). Extraction and derivatization procedure Opiate assay. Deuterated internal standards were added to all calibrator, quality control, and patient specimens. The scan standards were prepared by adding 100-~L aliquots of Mixture I and Mixture II to separate 4-mL aliquots of drug-free urine. Two milliliters of [3-glucuronidase (5000 U/mL) in 1M acetate buffer (pH 5) was added to each sample. Four milliliters of 300-ng/mL calibrator and 380-ng/mL positive quality control were added to the assigned tubes. Drug-free urine was used as the negative control. Four milliliters of patient urine, or an appropriate dilution in reagent-grade water, was added to the respective tubes. The samples were mixed and allowed to hydrolyze overnight at 60~ The samples were cooled, adjusted to pH 5.5-6.5 with 1N NaOH, centrifuged, and the supematant layers were carried forward to SPE. 6-AM. Samples for 6-AM determination were prepared in essentially the same manner as for opiate analysis but without hydrolysis. Deuterated internal standard in acetonitrile was added to all tubes and combined with 2 mL of 0.1M phosphate buffer (pH 6). Working calibrator and positive control samples were prepared at the time of assay by adding the secondary standards to separate 5-mL aliquots of drug-free urine. Five milliliters of patient urine, or a dilution of the urine with reagent-grade water, was used. The samples were mixed, adjusted to pH 5.5-6.5, centrifuged, and the supernatant layers were carried forward to SPE. F Cj 6-AM-I- MOR--- norMOR F Heroin zocine, dihydrocodeine, codeine, hydromorphone, morphine, and 6-monoacetylmorphine. Individualworking scan mixtures were prepared on the day of assay by spiking drug-free urine. Cj F Cj C!D V Cj norCOD F Cj Figure 1. Human heroin, morphine, and codeine metabolism. Abbreviations: F, free drug; Cj, glucuronide- or sulfate-conjugated drug; Cj*, 6-acetylmorphine conjugation is mentioned in reference 14; 6-AM, 6-acetylmorphine; MOR, morphine; norMOR, normorphine; COD, codeine; norCOD, norcodeine. 510 SPE SPE columns were conditioned by the sequential passage of 3 mL of methanol, 3 mL of reagent-grade water, and 1 mL of 0.1M phosphate buffer (pH 6.0). The supernatant layers from the samples were applied to the SPE columns. The columns were washed with 3 mL of reagent-grade water, 2 mL of 0.1M acetate buffer (pH 4.5), and 3 mL of methanol. The columns were dried by application of approximately 20-in. Hg vacuum for 10 min. The drugs were eluted with 3.0 mL of 4% concentrated ammonium hydroxide in ethyl acetate/isopropanol (84:12, v/v) and collected in 12 x 75-ram glass tubes. The solvent was removed under a stream of Journal of Analytical Toxicology, Vol, 21, October 1997 dry, oil-free air in a 40~ heating block. The residue was reconstituted with 400 IJL of ethyl acetate/MeOH (70:30, v/v), mixed, and transferred to an autosampler vial. The sample was dried as described previously, reconstituted with 100 I~Lof derivatization-grade acetonitrile, and capped. The trimethylsilyl derivatives were formed by reaction with 50 I~Lof BSTFAplus TMCS for 45 rain at 70~ in a heating block. The derivatized samples were transferred to autosampler microvials and recapped for gas chromatographic-mass spectrometric (GC-MS) analysis. GC-MS conditions and mass spectra obtained during same day analysis of scan standard Mixtures I and II. Results l~vo 43-year-old, apparently identical, twin males were participants in a methadone-maintenance substance abuse treatment program at this Department of Veterans Affairs Medical Center. These men had medical histories of opiate abuse. They provided urine specimens for clinical drug abuse screening twice each week as a condition of participation in the treatment program. In some specimens obtained from these men, an unusual pattern of heroin metabolites was noted. Initially, these isolated findings were viewed as artifacts, but several more instances of this metabolite pattern in their urine specimens impelled further study. A detailed examination of urine specimens obtained from these men during mid-1996 is described in this report. Figure 2 displays a section of a scan-mode total ion chromatogram obtained during opiate analysis of urine from one of the study subjects. The peak at retention time 13.26 rain corresponded with that of authentic 6-AMobtained from the scan standards analyzed the same day. The ion spectrum from the patient chromatograrn and spectrum of 6-AM-TMSare compared in Figure 3. Consequently a quantitative analytical method for 6-AMwas developed and validated. The recovery of 6-AM at 20 ng/mL was quantitative. The quantitative assay for 6-AM was linear (r2 = 0.999) over the concentration range 0.8--200 ng/mL with a slope of 0.95 and a # intercept of 1.42. However,some of the qualifying ions for the analyte and internal standard are common to both compounds. Concentrated samples in which the qualifying ratios were not within 20% were re-extracted using a greater dilution. The usual limit of quantitation and detection in our laboratory is The injection port temperature was maintained at 250~ The separations were accomplished on a 5% phenyl, 95% methyl silicon capillary column (25 m x 0.20-ram i.d., 0.33-11m film thickness, Hewlett-Packard) with a deactivated retention gap (5 m • 0.25-ram i.d., Restek). High-purity (99.999%) helium was used as the carrier gas. The head pressure was maintained at 150 kPa, which gave a flow rate of 0.5 mL/min at 250~ oven temperature. Splitless 1- or 2-1~Linjections were made. The instrument was tuned daily using perfluorotributylamine. The electron multiplier was set at autotune value for codeine and morphine analysis and 200 V above tune value for the 6-AMassay. A direct capillary connection to the ion source was used, and the interface was maintained at 310~ Ions used for quantitation are given in bold type. The maximum permissible variation of qualifier ion ratios was • 6-AM quantitation. The GC temperature program was as follows: initial temperature, 160~ held 1.00 rain; 25~ to 280~ 4~ to 300~ which was held for 2.2 rain; run time, 13 rain. The ions for selected ion monitoring (SIM) and integration were rn/z 402.2, 343.2, and 290.2 for 6-AM-d3and m/z 399.2, 340.2, and 287.2 for 6-AM. Codeine and morphine quantitation. The GC temperature program was as follows: initial temperature, 160~ held 1.00 rain; 20~ to 290~ 4~ to 305~ which was held for 1.25 rain; run time, 12.5 rain. The ions for SIM and integration were m/z 374.2, 346.2, and 237.2 for codeine-d3;m/z 371.2, 343.2, and 234.2 for codeine; m/z 432.2, 417.2, and 327.2 for morphine-d3 and; m/z 429.2, 414.2, and 324.2 for morphine. Qualitative scan mode for opiates. The .~ GC temperature program was as follows: < 2 initial temperature 140~ 10~ to 280~ 3.5~ to 300~ which was held for 1.79 rain; run time, 18 rain. The scan range was m/z 45-550. 10.50 11.00 11.s0 12.00 12.50 13.00 13.50 The prepared residues of the opiate assay were analyzed twice.The first injection used Time (min) 8IM mode for the quantitation of codeine Figure 2. Full spectrum total ion current chromatogram obtained from urine of one of the study and morphine. A second injection of the subjects. The specimen was prepared according to procedure given in the Experimental section same sample using scan acquisition was for opiate assay. Retention times correspond with TMS derivatives of codeine-d3 and codeine made for qualitative identification of any (peak 1), morphine-d3 and morphine (peak 2), and 6-acetylmorphine (peak 3). In this specimen, drug included in Mixtures I and II. Identificodeine and morphine concentrations were below the method limit of quantitation. cation was based on peak retention times 511 Journal of Analytical Toxicology, Vol. 21, October 1997 80,000 ng/mL. Although more specimens had detectable 6-AMconcentrations at higher morphine concentrations, there was no observable correlation between the ratio and the MOR concentration9 Forty-four urine specimens from the brothers were saved for analysis during a period of five months. The seven specimens which tested positive for opiates by enzyme immunoassay (EIA) were tested quantitatively for total morphine, total codeine, and 6-AM. The data in Table I show that the single sample in which 6-AMwas not detected was the only specimen that contained codeine. In the specimens containing 6-AM, all 6-AM/MORratios were greater than 100%. The 37 urines that tested negative for opiates by EIA were 399 A analyzed for 6-AM (Table II). Both subjects Scan 630 (13.255 min): 0801028.D (*) produced specimens with trace concentra340 tions of 6-AM in the absence of a positive opiate screen. The concentration range of 73 287 6-AM in the specimens in which it was de204 I tected was 1.2-10.3 ng/mL. 94 14.~ I 179 384 ] IlL .I. _,.I . ._9. . ,,..,,. . . ,LL .... ,.,,k.L, ,U,. 9 40% of the cutoff concentration9All qualifying ion ratios were within acceptable limits down to 6.3 ng/mL, which exceeded our normal criteria. For this study, the range was extended to the limit of detection, 0.8 ng/mL, by omitting ion m/z 287. Urines (n = 33) obtained from treatment programs that had MOR concentrations greater than 3500 ng/mL were assayed for 6-AM. The percentage ratio of 6-AM to MOR is plotted versus total morphine concentration in Figure 4. The average ratio was 09 which was consistent with reported values9 The highest 6-AM/MOR ratio from these typical specimens was 4.3%. Several specimens had negligible 6-AM concentrations with corresponding morphine concentrations greater than 50 100 150 200 250 300 350 399 B #58: 6-Acetylmorphine (TMS Derivative) (*) 340 73 287 9 4~. j :,., . ' . . - - . ' : .-'.-.'-_-:--. 2..~4 _..:_.:...~,. ,.282 / 59 L 94 124 146162179 ~ 229 253_ ,[ 50 100 150 200 250 [ .32L4 ' - ' - .'- . , ~ 356 384 300 350 Figure 3. A, mass spectrum obtained at the apex of peak 3 from Figure 2. Instrumental conditions were as described in the Experimental section (GC-MS conditions). B, mass spectrum obtained from TMS derivative of 6-acetylmorphine after derivatization and analysis of scan Mixture II. Instrumental conditions were as described in the Experimental section (GC-MS conditions). 5- o 4. v o o E o #__2 0 0 o ,< ,,a 0 o i o o o ---@:X]D. 0 o . ,o... 20000 o o 9 , .... 40000 , .... 60000 Q .... 80000 , 9 100000 .o. 9 , 120000 Total morphine (ng/mL) Figure 4. Plot of 6-acetylmorphine/total morphine (%) versustotal morphine concentration. These data obtained from 33 typical urine specimens which contained more than 3500 n~mL of total morphine. No ratio of 6-acetylmorphine/total morphine observed in this set of specimens was greater than 5%. 512 Discussion The specimens included in the study were received as clinical samples. As such, the donor identities were known, and analysis was not subject to the restraints of forensic protocol. Hospital policy precluded direct contact with the subjects, and specimen access was limited to the urine received for toxicology testing. When the pattern of elevated concentrations of 6-AMwith negligible total morphine was observed, five possibilities were considered: artifact, a drug other than heroin was involved, timing of the specimen donation relative to drug administration, route of administration, and impairment of the metabolic pathway. Artifact was initially considered a strong possibility. Environmental contamination of a specimen with heroin could account for the observed pattern in a given specimen. Conceivably, a subject who had not used opiates, but who had heroin-contaminated hands during sample collection, could introduce heroin into an otherwise drugfree specimen. Subsequent hydrolysis of heroin would produce substantial 6-AMwith minimal morphine concentrations within the first hours after contamination. Artifact became progressively less probable as subsequent samples that reproduced the unusual 6-AM/MORpattern were received. The route of administration affects the metabolism of drugs. There are various routes of opiate administration, including Journal of Analytical Toxicology, Vol. 21, October 1997 Table I. Urinary Distribution of Opiates from Study Subjects after Positive EIA* Screen Subject EW EW EW AW AW EW EW MOR (ng/mL) 6-AM (ng/mL) 6-AM/MOR (%) 309 118 313 363 183 209 175 642 379 326 n.d. 2152 1220 728 208 321 104 1176 584 416 COD (ng/mL) n.d. n.d. n.d. 151 n.d. intravenous, intramuscular, and subcutaneous injection; smoking; insufflation (snorting); and oral ingestion. Of these, intravenous injection and oral ingestion represent extremes of the drug administration spectrum. Other routes combine the metabolic consequences of intravenous or oral administration. Although oral heroin is more readily absorbed than morphine, there is a 100% first-pass effect (15). No orally n.d. n.d. * Abbreviations:EIA, enzyme immunoassay; MOR, total morphine; 6-AM, 6-acetylmorphine; COD,total codeine; n.d., not detected. Table II. Urinary 6-AM* from Study Subjects after Negative EIA Screen Month Subject 6-AM (ng/mL) 6 6 6 6 6 6 7 7 7 7 7 7 7 7 7 8 8 8 8 8 8 8 8 8 8 8 8 8 8 8 8 8 9 9 9 9 10 AW AW AW EW EW EW AW AW AW AW EW EW EW EW EW EW AW AW AW AW AW AW AW AW AW EW EW EW EW EW EW EW AW AW EW EW AW n.d. n.d. n.d. n.d. n.d. n.d. n.d. n.d. n.d. n.d. n.d. n.d. n.d. 3.6 1.6 1.9 n.d. n.d. n.d. n.d. n.d. n.d. n.d. n.d. 1.2 n.d. 3.8 n.d. n.d. n.d. 10.3 4.6 n.d. n.d. 3.9 2.5 n.d. * Abbreviations:EIA, enzyme immunoassay;6-AM, 6-acetylmorphine;n.d., not detected. ingested heroin or 6-AMreaches the systemic circulation. Intravenous administration provides 100% bioavailability, but carefully controlled studies have not demonstrated predominant 6-AM excretion in typical subjects (14). The timing of specimen collection relative to drug administration can have a dramatic effect on the relative concentrations of all urinary opiate metabolites. Studies with periodic timed urine collection after heroin administration gave a maximal 6-AM/MORratio of 8% (14). The appearance of a new "designer drug" yielding 6-AMas a primary metabolite would have produced many similar 6-AM/MOR patterns in our geographical area. However, this was not observed. Heroin can degrade to 6-AM before administration. 6-AMas a parent drug has not been studied, but the rapid metabolism of heroin to 6-AM metabolically would be similar to direct administration of 6-AM.The parent drug was probably heroin. The excretion pattern observed on multiple occasions in these closely related subjects suggests a defect in the heroin metabolic pathway. The observed concentrations of 6-AM in urine well above the proposed 10-ng/mL cutoffwithout greater than cutoff concentrations of MOR presents a general possibility of false-negative opiate use reports. The data presented in this paper suggest that if 6-AM is assayed only when total morphine is elevated, then some members of the heroin-using population may evade detection. There has been ongoing discussion in the forensic community concerning the guidelines for opiate testing. Testing for 6-AM without preliminary codeine and morphine determinations has been discussed as a possible approach. This design could distinguish heroin use from the prescription use of opiate narcotics and poppy seed consumption in the general population. References I. 2. 3. 4. M.A. ElSohlyand A.B. Jones. Morphine and codeine in biological fluids: approaches to source differentiation. Forensic Sci. Rev. 1: 14-21 (1989). E.J. Cone and W.D. Darwin. Rapid assayof cocaine, opiates and metabolites by gas chromatography-mass spectrometry. J. Chromatogr. 580:43-61 (1992). P.T.Smith, M. Hurst, and C.W. Gowdey. Spontaneous hydrolysis of heroin in buffered solution. Can. J. Physiol. Pharmacol. 56: 665-67 (1978). O. Lockridge, N. Mottershaw-Jackson, H.W. Eckerson, and B.N. La Du. Hydrolysis of diacetylmorphine (heroin) by human serum cholinesterase. J. Pharmacol. Exp. Then 215:1-8 (1980). 513 Journal of Analytical Toxicology,Vol. 2I, October 1997 5. 6. 7. 8. 9. 10. 514 B.A. Goldberger, W.D. Darwin, T.M. Grant, A.C. Allen, Y.H. Caplan, and E.J.Cone. Measurement of heroin and its metabolites by isotope-dilution electron-impact mass spectrometry. Clin. Chem. 39:670-75 (1993). E.J. Cone, P. Welch, B.D. Paul, and J.M. Mitchell. Forensic drug testing for opiates, I11. Urinary excretion rates of morphine and codeine following codeine administration. J. Anal. Toxicol. 15" 161-66 (1991 ). R. Dybowski and T.A. Gough. A study of transacetylation between 3,6-diacetylmorphine and morphine. J. Chromatogr. Sci. 22: 465-69 (1984). U. Boerner, R.L. Roe, and C.E. Becker. Detection, isolation and characterization of normorphine and norcodeine as morphine metabolites in man. J. Pharm. Pharmacol. 26" 393-98 (1974). G. Fritschi and W.R. Prescott, Jr. Morphine levels in urine subsequent to poppy seed consumption. Forensic Sci. Int. 27:111-17. (1985). B.D. Paul, J.M. Mitchell, and L.D. Mell, Jr. Gas chromatography/electron impact mass fragmentometric determination of urinary 6-acetylmorphine, a metabolite of heroin. J. AnaL ToxicoL 13' 2-7 (1989). 11. P. Kintz, A. Tracqui, B. Ludes, P. Mangin, A.A. Lugnier, and A.J. Chaumont. Identification of 6-monoacetylmorphine, as an indicator of heroin abuse. Acta Med. Leg. Soc. 39" 464-69 (1989). 12. E.J. Cone and P. Welch. Time course of detection of 6-acetylmorphine in urine after heroin administration. NIDA Research Monographs 95:449 (1989). 13. S.Y.Yeh, C.W. Gorodetzky, and R.L. McQuinn. Urinary excretion of heroin and its metabolites in man. ]. Pharmacol. Exp. Ther. 196" 249-56 (1975). 14. E.J.Cone, P. Welch, J.M. Mitchell, and B.D. Paul. Forensic drug testing for opiates: I. Detection of 6-acetylmorphine in urine as an indicator of recent heroin exposure; drug and assayconsiderations and detection times. J. Anal. Toxicol. 15:1-7 (1991 ). 15. C.E. Inturrisi, M.B. Max, K.M. Foley, M. Schultz, S.U. Shin, and R.W. Houde. The pharmacokinetics of heroin in patients with chronic pain. N. Eng. J. Mecl. 310:1213-17 (1984). Manuscript received March 26, 1997; revision accepted May 28, 1997.