Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
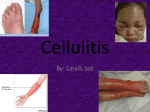
Derm April-NH/AH 06/04/2006 16:06 Page 1 Cellulitis and erysipelas – spot the difference Forum Dermatology If cellulitis is suspected, early diagnosis and intensive treatment are essential, writes Johnny Loughnane Figure 1: Cellulitis due to penetrating injury–plantar surface of foot Figure 2: Varicose ulcer with spreading cellulitis Table 1 CELLULITIS IS A NON-CONTAGIOUS INFECTION of the skin. It is common in general practice and a frequent cause of acute medical admission to hospital. A spreading bacterial infection of the lower dermis and subcutaneous tissues gives rise to tender inflammation. Erysipelas in contrast, is a more superficial infection involving the dermis and upper subcutaneous tissues. Being more superficial, erysipelas presents with a raised, distinct border. In contrast, the advancing border of cellulitis tends to be rather indistinct. In practice it is difficult to tell how deep the skin involvement is, and therefore to differentiate between cellulitis and erysipelas. It is probably best to consider erysipelas as a cellulitis with superficial spread. Streptococcus pyogens is the most frequent causative organism. Staphylococcus aureus may also cause it. Eighty per cent of cellulitis is due to strep. Most erysipelas is caused by strep. Cellulitis may sometimes be caused by a combination of staph and strep infection. The most common site of infection is the lower limb. Bacteria gain entry via a break in the skin surface (see Table 1). In the past, erysipelas was more common on the face but is now more frequent on the legs. Clinical features Leg ulcer, diabetes, lymphoedema, obesity and peripheral Ports of entry for bacteria in lower limb cellulitis • Varicose ulcers • Trauma • Fissuring in hyperkeratotic skin • Tinea pedis • Lower limb eczema • Intravenous drug abuse vascular disease are risk factors for developing cellulitis. In early infection, the patient complains of pain and of feeling generally unwell. Infection tends to progress rapidly with development of malaise, rigors, listlessness and confusion. Examination reveals swelling and redness that is tender and hot to touch. The advancing edge of cellulitis is not as well demarcated as that of erysipelas. Lymphangitis (tender, red swelling of the lymphatics) may be present and there may be tender regional lymphadenopathy. The diagnosis is essentially clinical. Because of the importance of early diagnosis and treatment, always closely inspect and feel the lower limbs of patients at risk, looking for the signs of inflammation outlined above. FORUM April 2006 61 Derm April-NH/AH 06/04/2006 16:06 Page 2 Forum Dermatology Table 2 Table 3 Indications for admission Initial antibiotic treatment • Severe or rapidly worsening infection • Flucloxacillin 1g QID • Patient systemically unwell or vomiting • Flucloxacillin 1g QID + amoxicillin 1g TID • Uncertainty regarding the diagnosis (need to outrule DVT) • Flucloxacillin 1g QID + phenoxymethylpenicillin 500mg QID • Orbital or periorbital cellulitis • Phenoxymethylpenicillin 1g QID, if erysipelas • Evidence of complications • Erythromycin 500mg-1gm QID if penicillin allergy • Immunocompromised patient • Diabetes mellitus – if unstable • Significant comorbidity (eg. heart failure, malignancy, respiratory failure, renal failure) • Children under one year of age • Frail elderly without good home support • Lack of response to home treatment at 48 hours Complications Septicaemia may complicate cellulitis, and a mortality rate of 5% has been reported in patients requiring hospital admission for cellulitis. Strep nephritis is rare. Cellulitis damages the lymphatic drainage system which may be subclinical or may cause symptomatic lymphoedema. It is estimated that up to 7% of people will develop chronic oedema after an episode of leg cellulitis. Once established, lymphoedema predisposes to further episodes of cellulitis. Twenty-five per cent of patients admitted to hospital with cellulitis will suffer recurrence in the future. Treatment A high index of suspicion, leading to prompt diagnosis and treatment, is vital. Appropriate antibiotics at adequate dosage and for a sufficient length of time should be given systemically. Patients who are not systemically unwell and do not have significant co-morbidities can be managed at home. Many will need admission to hospital for treatment (see Table 2). The patient should rest and elevate the affected limb. This reduces swelling and pain. Paracetamol 1g QID may be needed for pain. It is best to avoid NSAID use as there have been reports linking their use with the development or aggravation of necrotising fasciitis. We have little evidence to guide our choice of antibiotic in the treatment of cellulitis so treatment must be empirical. The chosen antibiotic should cover staph and strep infection. High dose flucloxacillin will cover both streptococci and penicillinase-resistant staphylococci. Flucloxacillin 1g QID, used alone, is recommended as initial treatment. Some recommend combining this with amoxycillin 1gm TID or phenoxymethylpenicillin 500mg QID. However, penetration of phenoxymethylpenicillin in tissue is poor. In patients allergic to penicillin use erythromycin 500mg1000mg QID. Remember that 20% of staph and strep are resistant to erythromycin. Therefore, if erythromycin is used, early follow-up is essential to ensure response. Clindamycin is an alternative for penicillin-allergic patients. As erysipelas is almost always due to strep infection, highdose phenoxymethylpenicillin (1g QID) used alone is advocated by some as a suitable initial treatment. Antibiotics should be continued for at least 10 days. Patients should then be reviewed and treatment continued if signs of infection persist. Be prepared to continue antibiotics for up to four weeks. Use potassium permanganate soaks (for 20 minutes) if there is any exuding area, eg. infected varicose ulcer. The patient should be followed up after 48 hours and advised to call earlier if there is any significant deterioration. Follow up As stated, there is a significant risk of recurrence. To reduce this risk: Treat underlying cause • Tinea pedis – antifungal therapy • Venous ulcer – compression bandaging, varicose vein surgery • Diabetes mellitus – optimise control • Leg oedema – support stockings, diuretic. • Trauma – advise on injury avoidance. Prophylactic antibiotics • Phenoxymethylpenicillin 500mg BD for one month, followed by 500mg daily • Erythromycin 500mg daily if allergic to penicillin • Prophylactic antibiotics should be considered for patients with high risk factors who have had two episodes of cellulitis. Cellulitis is a common problem in primary care. A high index of suspicion needs to be maintained to facilitate early diagnosis and intensive treatment. Consider admission in severe disease or if there is significant co-morbidity. Early follow-up should be arranged to check response to treatment. Johnny Loughnane is in practice in Co Limerick www.icgp.ie 62 FORUM April 2006