Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cushing reflex wikipedia , lookup
Circulatory system wikipedia , lookup
Intracranial pressure wikipedia , lookup
Cardiac output wikipedia , lookup
Haemodynamic response wikipedia , lookup
Biofluid dynamics wikipedia , lookup
Hemodynamics wikipedia , lookup
Blood pressure wikipedia , lookup
Blood pressure measurement wikipedia , lookup
Homeostasis wikipedia , lookup
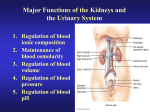
Physiology # 2 Renal Filtration & Tubular reabsorption Dr. Ahmad Dwari Qaisar A. Maaya'h Sheets 1 | P a g e Instruction! Let's start with this cool information: How coffee affects renal system (renal output)? Coffee increases the renal output, by increasing the Glomerular Filtration Rate (GFR), and by decreasing the reabsorption of Na+. Caffeine keeps us awake by acting on the CNS; by interfering with Adenosine receptors in the Brain. As we are doing any mental activity, adenosine will be accumulated (adenosine: inhibitory neurotransmitter), so, you will fall asleep; so Caffeine will interfere with adenosine receptors, by blocking them making you keep awake, and alert. Glomerular Filtration Rate (GFR) and Nephron Filtration Membrane (NFM) – forces affect them: We have a huge GFR (almost 180 L/day of plasma) through the glomeruli in both kidneys. So, we have some forces that are responsible for this filtration of plasma through this fenestrated membrane. We have 3 main forces that leads to this high GFR, they are: 1- The Glomerular Capillary Hydrostatic Pressure (GCHP): Once the blood reaches the glomerulus it will fill it, and this blood filling will create a hydrostatic pressure, in which results from the arterial pressure pushes the glomerulus. This pressure is higher than any other pressure in any other capillary system in the body; because two arterioles surrounds this capillary (high-resistance system). So, this will create a huge GCHP, which is about 60 mm Hg. This is the main driving force to push the plasma through the nephron filtration membrane. So, It is the major force that induces glomerular filtration. Depends contraction of the heart, and afferent/efferent arteriolar resistance. ** THIS FORCE PROMOTES FILTRATION. 2- The Plasma-Colloid Osmotic Pressure (PCOP): Once the plasma gets filtered, plasma proteins stay not filtered. So, plasma proteins will be concentrated in the glomerulus, this will create an osmotic/oncotic pressure (32 mm Hg), that moves water (by osmosis) from Bowman's capsule back to the glomerulus. So, it is due to the retention of plasma proteins in the blood of the glomerulus. Determined by: a. Arterial plasma colloid osmotic pressure b. Fraction of plasma filtered (filtration Fraction) ** THIS FORCE DECREASES FILTRATION. 2|Page 3- The Bowman's Capsule Hydrostatic Pressure (BCHP): Once the Bowman's capsule is filled with filtrated plasma, this filtrate will creates a hydrostatic pressure (18 mm Hg), that pushes the filtrate back through the NFM to the glomerulus. ** THIS FORCE DECREASES FILTRATION. - Bowman's capsule pressure & Glomerular oncotic pressure are LESS than the Glomerular hydrostatic pressure, so, we will end up with the sum of these 3 forces; (Net filtration pressure = 60 – 18 – 32 = 10 mm Hg). This 10 mm Hg will result in the filtration of plasma. All these 3 forces are physical forces (passive transport = depends on fluids dynamics & movement through blood vessels and membranes), there is no active transport (energy spent) here. - No active transport mechanisms or local energy expenditure are involved in in moving fluid across the glomerular membrane into Bowman’s capsule. Glomerular Filtration Rate (GFR) - Glomerular Filtration Rate (GFR): the total amount of filtrate formed per minute or per day, by the kidneys. (1.25 L/min OR 180 L/day). 3|Page - GFR regulation is mainly due to changes in the glomerular capillary blood pressure; a higher arterial blood pressure supplying the glomerulus can increase the GFR. So, we need this regulation to maintain proper kidney function. Factors that affect GFR 1- Decrease (↓) in the Glomerular capillary filtration coefficient (↓) GFR. (e.g.: chronic uncontrolled hypertension, DM, or chronic kidney disease). So, the filtration membranes are of no efficient filtration of the plasma. 2- Increase (↑) in the Bowman's capsule hydrostatic pressure (↓) GFR. (e.g.: stones; they will prevent the flow of the urine and filtrate, and this will increase the volume of filtrate in the Bowman's capsule and in the tubular system, so, this will increase the BCHP, reducing the GFR). 3- Increase (↑) in the Glomerular capillary colloid osmotic pressure (↓) GFR – it always constant, unless a pathology is present, Like pathologies leads to: (↑GFR, or ↓ renal plasma flow) 4- Increase (↑) in the Glomerular capillary hydrostatic pressure ↑ GFR : Important in physiological regulation of GFR. this pressure is determined by: 1. Arterial blood pressure 2. Afferent "enters the nephron" arteriolar resistance (controls the blood flow enters the nephron: so if we dilate this arteriole this will increase the flow, 4|Page increasing the GCHP, thus increase the GFR; while if we have vasoconstriction the opposite will happen.) 3. Efferent "exits the nephron" arteriolar resistance this has biphasic effect: At initial constriction, we are sequestering the blood in the glomerulus, so we will have more blood in the glomerulus, more blood pressure, more filtration. (Moderate ↑ resistance slight ↑ GFR) Severe constriction (the blood flow will fall below normal) ↓ GFR **Effect of change in afferent arteriolar resistance or efferent arteriolar resistance on glomerular filtration rate and renal blood flow.** FILTRATION CO-EFFICIENT - Glomerular Capillary Filtration Coefficient (Kf) This is a physical characteristic of the permeable membranes. It values in the GFR is: K= 12.5 ml/min/mmHg. And its formula is: Kf = Hydraulic Conductivity x Surface Area 5|Page - Normally it is not highly variable. - Disease that can reduce Kf and GFR: a- chronic hypertension b- obesity/diabetes mellitus c- glomerulonephritis Regulation of GFR and renal blood flow Under normal condition, the main driving force of filtration Is GCHP. While BCHP and GOP are most of time constant. So, under normal condition, the kidney tries to have constant GFR. So, no major variations are present in GFR due to any change in the BP. For example, when you are doing physical activity, you BP will increase, but your GFR will stay constant (If not constant = loss of fluid). So, all in all: Changes in the GFR primarily result from changes in glomerular capillary blood pressure. Changes in plasma colloid osmotic pressure and Bowman’s capsule 6|Page hydrostatic pressure are not subject to regulation and do not vary much under normal conditions. Uncontrolled shifts in the GFR can lead to fluid and electrolyte imbalances. So, We have 3 basic mechanisms to keep GFR constant, within limited range, despite the change in the blood pressure over the whole day: 1- Auto-regulation (regulates GFR and Renal Blood Flow): GFR remains constant if the Arterial pressure ranges from 75 to 160 mmHg. So … Normally filtration=180 /day, reabs. = 178.5 L/day urine =1.5 /day. Auto – regulation means automatic, something from the kidney itself. Even if you remove the kidney outside the body it will still have this property. This Property will keep the GFR and Blood flow within certain limits. If we don't have this Property, and we have 25% increase in the BP, the GFR will increase to 225 L/day, and if reabsorption is constant urine output = 46.5 L/day. (Very huge amount) • So, 30 folds increase in urine formation depletes the body. Renal Blood Flow (RBF): 1100 ml/min 22% of the C.O., and this large C.O. is important to remove the wastes from the blood. Also, to deliver enough O2 to the working tubules, that contains Na+ - K+ pumps, that needs huge amount of ATP (i.e., large fraction of O2 is consumed by the kidneys due to the high rate of active sodium reabsorption by the tubules). So, GFR & RBF are regulated by the Auto – regulation mechanism. 7|Page **Auto – regulation mechanism is primarily myogenic, so, it is under the control of smooth muscles in the arterioles of the kidneys. - If we have increasing in the arterial blood pressure (in the afferent arteriole), and we don’t have auto – regulation, we will have increase in the GFR, and increasing in the net filtration pressure. But, because of auto – regulation these myogenic mechanism in the afferent arteriole wall will constrict the arteriole, and decrease the blood flow to the glomeruli, decreasing the GFR and the NFP to the normal values. - If we have a fall in the arterial blood pressure (in the afferent arteriole), the input of blood to the glomeruli will decrease, so, the amount f the metabolic wastes will accumulate in the body. So, because of auto – regulation these myogenic mechanism in the afferent arteriole wall will dilate the arteriole, and increase the blood flow to the glomeruli, increasing the GFR and the NFP to the normal values. This figure to the left demonstrates the mechanism of Auto - regulation; which is a myogenic, thus altering the caliber of the afferent arterioles due to stretch. • If the GFR rises by increased arterial pressure, the afferent arterioles constrict. This lowers the GFR. • If the GFR decreases, the afferent arterioles dilate. This increases the GFR. 8|Page 2- ANS and Hormones regulations: The regulation of the GFR and RBF is done by the sympathetic nervous system (SNS) (we don’t have any parasympathetic regulation for the kidneys), and gets activated under stressful conditions (like: fight or flight, bleeding, diarrhea, and reduction in the blood pressure). So, the SNS will be activated to bring the BP to normal. By, decreasing the GFR; because we don’t want to lose the body's fluid and our solutes in the urine, we need to retain the fluids to stay in the body, to return the BP to normal. This action is done by vasoconstriction of the afferent a efferent arterioles. It also stimulates the release of Renin hormone. Renin hormone activates aldosterone release, that retains Na+ and eventually water, bringing the BP back to normal. At the same time there are some Hormones and autacoids, that regulates the GFR and RBF. We have 2 classes of them: 1st class: the ones that causes vasoconstriction (leads to deceasing the GFR and RBF): Norepinephrine , epinephrine, endothelin constrict renal blood vessels and decreases GFR. Angiotensin II constricts efferent arterioles ↑GFR - ↑ Na, H2O reabsorption. 2nd class: the ones that causes vasodilation (leads to increasing of the GFR and RBF): Endothelial - Derived Nitric oxide, decreases resistance, and ↑ GFR Prostaglandins, bradykinin cause vasodilatation. 3- Tubuloglomerular feedback mechanism Macula densa cells that found in space b/w the afferent and afferent arterioles. They sense the NaCl concentration in the fluid moving into the distal convoluted tubule. So, this sensation is very important in the regulation of the GFR and RBF by constricting or dilating the blood vessels. - So, If GFR increases, then NaCl movement also increases, then Macula densa cells send a paracrine message causing the afferent arteriole to contract, decreasing GFR and NaCl movement - While, If GFR deceases, then NaCl movement also decreases, then Macula densa cells send a paracrine message causing the afferent arteriole to dilation, increasing GFR and NaCl movement. By activation of RAAS. 9|Page NOTE: Auto - regulation and glomerulotubular balance try to maintain a constant GFR these processes are not 100% effective, so, ↑BP will always lead to ↑GFR (pr. Diuresis or pr. Natriuresis). Proteins, amino acids, glucose that are filtrated, they are going to be reabsorbed back, by second active transport. Baroreceptor reflex influence on the GFR in long-term regulation of arterial blood pressure, that will activate the SNS, that affects the GFR (reducing the filtration pressure), this means reduction in the GFR, to bring the BP back to normal. 10 | P a g e TUBULAR REABSORPTION We have huge amount of plasma gets filtered in the glomeruli (180 L/day). We don’t have this amount of plasma, this mean that our plasma is filtered 60 times a day. So, we need to reabsorb about 99% of the plasma back to the blood. This is what is called tubular reabsorption. Movements of water, solutes and other substances from the filtrate back to the blood. This process is highly selective, of a large amount (99% of filtered substances will back to blood). So…Tubular Reabsorption Is Selective and Quantitatively Large. • The rate at which each of these substances is filtered is calculated as: Filtration = Glomerular filtration rate \ Plasma concentration • A 10 per cent decrease in tubular reabsorption, from 178.5 to 160.7 L/day, would increase urine volume from 1.5 to 19.3 L/day (almost a 13-fold increase) if the glomerular filtration rate (GFR) remained constant. Filtered substances are transferred from the tubular lumen (through tubular cells) to the peritubular capillaries (blood). This process is highly selective and variable. - The return of substances to the blood is needed to maintain the composition of the ECF. Only excesses of materials are eliminated. - Reabsorption rates are high: 124 of 125 ml of filtered fluid per minute, 99% for water 100% for glucose 99.5% for salt. 11 | P a g e Tubules of the nephrons are made of a single layer of tubular cells. This allows an easy movement of fluids and solutes. Reabsorbed substance must cross: 1. Tubule wall. 2. interstitial fluid. 3. Wall of the peritubular capillaries, thus entering the blood. The single layer of epithelial cells of the nephron tubule has: i. Luminal membrane (facing tubule lumen). ii. Basolateral membrane (facing the interstitial spaces between the tubule and peritubular capillaries). * Many types of transport mechanisms occurs through the tubular membrane: 1- Active transport: consumes energy (ATP) to transport materials, against their electrochemical gradient. It is of 3 types: a- Primary Active: Na-K, Hydrogen, H-K, and Calcium pumps. 12 | P a g e Sodium: on basolateral sides, Na-K pump, creates negatives inside increases Na-influx. b- Secondary active : Co-transport, counter- transport . Na -Glcose , Na - a.a , Na - H+. The transport of Na leads to the transport of other molecule. c- Pinocytosis: Proteins . NOTE: Aldosterone is produced in the adrenal cortex. Reabsorption of Na: It is the main osmotic active substance in the ECF. If we have decrease in the Na – ECF concentration , reabsorption of Na will be done. Most Na filtered will be reabsorbed (Of the Na+ filtered, 99.5% is normally reabsorbed). This reabsorption of Na involves an active transport process. Na-K pump, pumps K to the inside of the cell, and Na to the outside of the cell. This pump is found in the basolateral side of the tubular cells. This movement of Na to the outside, making the tubular lumen more negative. This will produce an electrochemical gradient that leads Na to move through another channels that found at the luminal side. 13 | P a g e The reabsorption process differs according to the part of the nephron. Sodium is reabsorbed throughout the tubule with the exception of the descending limb of the loop of Henle. Of the Na+ reabsorbed, on average: A- (67%) in the proximal tubule (2/3 of Na+) (Plays an important role in the reabsorption of glucose, amino acids, water, chloride ions, and urea) – this is a not regulated amount of Na reabsorption. It has to happen. So reabsorption here is important to reabsorb 2/3 of Na, and other materials. B- (25%) in the loop of Henle (Plays a role in the production of varying concentrations and volumes of the urine) – loop of Henle is important in counter – current multiplication, it helps us to concentrate/dilute of urine. Also, this is a not regulated amount of Na reabsorption. By producing hyperosmolar medullary interstitial. C- (8%) in the distal and collecting tubules (depends on hormonal control, and plays an important role in regulating ECF volume) – this amount is regulated by hormones like: Aldosterone (stimulated via renin system) increases Na+ reabsorption - it increases BP / Blood volume. Atrial Natriuretic Peptide “ANP” (released from heart / atrium) decreases Na+ reabsorption – it decreases BP / Blood volume. Notes: The lecture includes 2 subjects, are (filtration + tubular reabsorption). Slides are included (Slides from: "1+2 file": 28 – 46, "2+3 file": 1 – 7). Listening to the Record is not preferable. Your Colleague: Qaisar Maaya'h GOOD LUCK AWN 14 | P a g e