Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cell growth wikipedia , lookup
Cell culture wikipedia , lookup
Cellular differentiation wikipedia , lookup
Extracellular matrix wikipedia , lookup
Signal transduction wikipedia , lookup
Cell encapsulation wikipedia , lookup
Cytokinesis wikipedia , lookup
Organ-on-a-chip wikipedia , lookup
Programmed cell death wikipedia , lookup
Cell membrane wikipedia , lookup
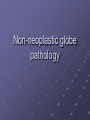
Non-neoplastic globe pathology Case 1 White mass in vitreous THIS MASS IN THE VITREOUS CAVITY IS COMPOSED OF WALL-TO-WALL NEUTROPHILS Gram + (dark blue) cocci. Endogenous bacterial endophthalmitis Endophthalmitis Inflammation of one or more coats of the eye and adjacent intraocular spaces. Infectious (exogenous or endogenous) and non-infectious (lens induced, foreign body) Infective endophthalmitis Causes after surgery: Gram + bacteria:Staphs, streps, corynebacterium, propionibacterium Gram- bacteria: pseudomonas, proteus, haemophilus, klebsiella, E-coli, enterobacter. Fungi: Aspergillus, candida, penicillium Causes of endogenous endophthalmitis Fungi: Candida and Aspergillus Bacteria: Neisseria meningitidis, streptococcus, staphs, bacillus cereus, nocardia Case 2 History Male adult Leukaemia On chemo. Brain abscess Dies Total body biopsy (Autopsy). Eyes examined by ophthalmic pathologist. Retina in reasonable good shape Full thickness necrosis of neural retina, featuring a homogeneous eosinophilic appearance with loss of cell details and ghost outlines of cells. Very little inflammation. Cysts containing bradyzoites (multiple black dots in pink cysts) TOXOPLASMOSIS Unicellular protozoal parasite. Definitive host is CAT Intermediate hosts: humans, rodents, fowl. Toxoplasmosis Parasite invades retinal cells directly Focal retinitis with an overlying vitritis In this case presented with ARN (well recognised). Toxoplasmosis Years later-reactivation can occur in areas of scars Congenital and acquired forms Congenital form-associated with encephalomyelitis, hepatosplenomegaly and retino-choroiditis Histology of Toxoplasmosis Protozoa in 3 forms Free trophozoite-lives in intracellular vacuole. Pseudocyst form-many protozoa enclosed by retinal cell membrane. Bradyzoite surrounded by self-made membrane-becomes cyst and can be extruded from retinal cells. Cyst forms when environment hostile. Cyst can remain latent. Case 3 Red eye Patient just arrived from SouthEast Asia Exudate in AC Thickened iris Granulomatous inflammation Pink, acid fast bacilli, stained with Ziehl-Neelsen stain. Other ways of detecting TB-Culture, PCR. TB UVEITIS TB AND THE EYE Direct innoculation, contiguous or bloodborne. Lids, conj, orbit, cornea, episclera and sclera, retina, optic nerve all involved. Cornea-immune mediated reaction (interstitial keratitis). Choroid vulnerable-rich blood supply NON-INFECTIVE INFLAMMTION 1 Non-caseating naked granulomas, in retina SARCOID AND EYE Idiopathic Afro-caribbeans 30 % ocular involvement Uvea, retina, lacrimal gland Anterior uveitis, pars planitis, retinal periphlebitis Nodules on lids, conj, band keratopathy Non-necrotising granulomatous inflammation + fibrosis later on. Naked granulomas. Can undergo necrosis Diagnosis of exclusion. 3 Iris expanded Higher power shows diffuse population of small lymphocytes Mostly T cells (CD 3+). UVEITIS EXOGENOUS-POST TRAUMA ENDOGENOUS-IDIOPATHIC and those with specific causes: Anterior (iritis), intermediate (cyclitis), posterior (choroiditis) Associations-juvenile RhA, ank spond (HLA B27) Reiter’s, uc, enteritis (salmonella, shigella, yersinnia), psoriatic, behcet’s Fuch’s uveitis syndrome, VKH. Causes-sarcoid, tb, leprosy, syphilis, parasites, fungi (candida, coccidio, histo, blasto), HSV, VZV, EBV, Complications of uveitis Cornea-endothelial cell loss-BK, band keratopathy AC-scar formation-iris obliteration Iris-atrophy, necrosis, loss of muscle, PAS, rubeosis, ectropion uveae, immobile pupil, iris bombe Lens-posterior cataract secondary to lens epithelial migration. Complications of uveitis Ciliary body-atrophy, cyclitic membrane Vitreous-vascularisation, condensation, PVD Choroid-atrophy, scarring, chorioretinal scar. Retina-perivasculitis, cmo, exudative detachment, rpe alterations. Glaucoma-clogging due to cells, PAS, pupil block, bombe, trabeculitis 4 Diffuse chronic inflammation of sclera-brawny type Chronic inflammatory cells Palisaded granulomatous Inflammation of sclera with collagen degeneration (necrobiosis). This is seen in nodular variant scleritis Often see this pattern of inflammation in connective tissue disorder assoc. scleritis Granulomatous inflammation again SCLERITIS Diffuse chronic inflammation in diffuse form, Or : granulomatous inflammation with collagen degeneration (necrobiosis) in nodular form. SCLERITIS Anterior-diffuse, nodular and necrotising with inflammation (brawny), necrotising without inflammation (scleromalacia perforans) Posterior-30% associated with systemic vasculitides, CTDs (rheumatoid, SLE, PAN, Wegener’s, relapsing polychondritis etc etc), lymphoma. Complications of scleritis Keratitis Cataract Uveitis Glaucoma Perforation of sclera Retinal detachment 5 Choriocapillaris intact Granulomatous (non-caseating) inflammation of uvea (choroid in this case), sparing the choriocapillaries Dalen-Fuch’s nodule-sub RPE granuloma (arrow). Reaction to uveal melanocytes….(current thinking) Histological differential: INFECTION, SARCOID,VKH DIFFERENTIAL INFECTION, SARCOID,VKH 6 DIABETES AND THE EYE Should be very familiar with this topic. Pathogenesis Irreversible non-enzymatic glycation of proteins occurs, for example: of matrix proteins (platelet activator inhibitor -1); this affects cell migration/activation of calcium channels in pericytes (responsiveness to endothelin-1-induced contractility) and thereby affecting function apoptosis has been linked to hyperglycemia and retinal pericyte death hyperglycemic states deplete intracellular glutathione (defense against peroxidation) hyperglycemic environments trigger upregulation of bax (apoptosis activator) and downregulation of bcl-2 (apoptosis inhibitor) eventually causing capillary pericyte and capillary endothelial cell death -glycosylated hemoglobin levels correspond to increased risk of retinopathy -growth factors that are considered to have a role in PDR include VEGF, Insulin likeGF I, Fibroblast GF; chemical mediators include IL-8 and interferon induced protein VEGF is associated with endothelial cell hypertrophy and capillary lumen obliteration -evidence of an intra-ocular rennin-angiotensin system with vitreous pro-rennin in diabetic patients; intra-ocular angiotensin-II synthesis is elevated and may have a role in NVI in DR -abnormal platelets, abnormal red cell deformability (micro-displacement), altered leucocyte deformability and altered blood viscosity contribute to retinal vessel occlusion and ischemia -plasma lipids are associated with hard exudates -growth hormone is thought to support development and progression of DR Lacey vacuolation of iris pigment epithelium-due to accumulation of glycogen-present in 40% of enucleated eyes from diabeticsDIABETIC IRIDOPATHY Pink glycogen deposits, with PAS stain Ectropion uveae, secondary to rubeosis New vessels on anterior stromal surface Normal pars plicata Grossly thickened basement membrane of pars plicata Normal retinal arteriole Arteriolosclerosis-note thick wall-called hyalinisation. Hyalinisation due to accumulation of lipid and fibrin, from leaky vessel, due to pericyte death Exudative maculopathy-pink exudate between RPE and fovea Hard exudates-protein rich eosinophilic material settles in outer plexiform layer because this is watershed zone between retina’s 2 blood supplies. Therefore cannot drain away easily. Hard exudates composed of lipid containing foamy macrophages Ovoid eosinophilic bodies of varying size in optic fibre layer Pink bodies in optic fibre layer-cotton wool spots or cytoid bodies. Indicate ischaemia and composed of swollen axons from disturbed axoplasmic flow-packed full of organelles. gliosis Chronic ischaemia of retina. Note loss of inner 2/3rd architecture (RGCs, INL, IPL), and replaced by gliosis-pink stuff. ONL remains with outer photoreceptor segments. Proliferative diabetic retinopathy Note new-vessels, surrounded Fibrous tissue on retinal surface. PRP SCAR Loss of choriocapillaris Bruch’s Loss of RPE Gliotic retina PRP SCAR-loss of RPE and choriocapillaris Retinochoroidal atrophy Retinal gliosis Gliotic retina in direct apposition to Bruch’s 7 Occluded branch venule. Note inflammation around vessel -attempts at organisation of thrombus Perl’s stain picks up haemosiderin Stains it intense blue. This indicates previous intra-retinal haemorrhage from BRVO CRVO/BRVO 8 Hard druse. Pink, homogeneous nodular material Lies between RPE basement membrane and inner collagenous part of Bruch’s. Note overlying RPE arophy Drusen Made up of: Alpha 1 antitrypsin Alzheiner amyloid beta protein Amyloid p protein Apolipoproteins B and E Cholesterol esters Clusterin Complement factors Complement receptor 1 Factor 10 Heparan sulfate proteoglycan HLA DR Immunoglubulins MHC class 2 antigens Peroxidized lipids Phospholipids TIMP-3 Transthyretin Ubiquitin vitronectin Thickened Bruch’s Fluffier, more diffuse, soft drusen Thick Bruch’s, hard drusen and complete loss of photoreceptors Haemorrhage of CNVM. CNVM lies between neural retina And RPE Eventual organisation of haemorrhage Will lead to disciform scar. RPE choroid RETINA CNVM RPE Vessel of CNVM CNVM choroid RPE ARMD dry and wet ARMD…. Commonest cause of legal blindness in developed world. Elderly Caucasian Hallmarks=drusen, RPE atrophy, CNV Pathogenesis ? Defects in RPE-Bruch’s-choriocapillaris complex Collection of heterogeneous disorders associated with multiple genetic and environmental factors ARMD pathogenesis ? Bruch’s accumulates lipids, non-collagenous proteins, extracellular matrix + collagen and elastin changes. This occurs with aging. Then…second phase…accumulation of basal linear deposit (between RPE cell and its basement membrane) and basal laminar deposit (between RPE basement membrane and inner collagen layer of Bruch’s membrane). Lipofuscin accumulates in RPE. Resultant increase in thickness of Bruch’s and impaired molecular transport through Bruch’s and RPE……photoreceptor cell death…..AMD. Drusen=sign of sick RPE. Thickening of Bruch’s thought to lead to metabolic changes and hypoxia. This is a stimulus for angiogenic factor release from RPE cells. Basal laminar deposits associated with neovascularisation. Choroidal neovascularisation leads to-exudative AMDhaemorrhage-disciform scarring Some AMD facts Wet and dry forms Risk factors: age (older), sex (women?), race (white caucasian),light exposure (controversial), cardiovascular (atheroma), diet (lipids, AREDS study-zinc and anti-oxidants), smoking+ Complement factor H gene strongly associated with AMD (up to 50% of cases). Single nucleotide polymorphism (Tyr402-His). Thought to lead to inappropriate inflammatory response of which drusen is a product. Leads to death of RPE and photoreceptors.