Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Herd immunity wikipedia , lookup
Common cold wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Vaccination wikipedia , lookup
Neonatal infection wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Infection control wikipedia , lookup
Immune system wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Immunocontraception wikipedia , lookup
Adaptive immune system wikipedia , lookup
Molecular mimicry wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Innate immune system wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
DNA vaccination wikipedia , lookup
Human papillomavirus infection wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Hepatitis B wikipedia , lookup
Review Article
Indian J Med Res 130, September 2009, pp 266-276
Immune responses to human papilloma viruses
M.A. Stanley
Department of Pathology, University of Cambridge, Cambridge, UK
Received February 16, 2009
HPV infection in the genital tract is common in young sexually active individuals, the majority of whom
clear the infection without overt clinical disease. However most of those who develop benign lesions
eventually mount an effective cell mediated immune response and the lesions regress. Regression of
ano-genital warts is accompanied histologically by a CD4+ T cell dominated Th1 response; animal
models support this and provide evidence that the response is modulated by CD4+ T cell dependent
mechanisms. Failure to develop effective CMI to clear or control infection results in persistent infection
and, in the case of the oncogenic HPVs, an increased probability of progression to CIN3 and invasive
carcinoma. The central importance of the CD4+ T cell population in the control of HPV infection is
shown by the increased prevalence of HPV infections and HGSIL in individuals immunosuppressed as
a consequence of HIV infection. The prolonged duration of infection associated with HPV seems to be
associated with effective evasion of innate immunity as reflected in the absence of inflammation during
virus replication, assembly and release, and down regulation of interferon secretion and response thus
delaying the activation of adaptive immunity. Serum neutralising antibody to the major capsid protein
L1 usually develops after the induction of successful cell mediated immunity and these antibody and cell
mediated responses are protective against subsequent viral challenge in natural infections in animals.
Prophylactic vaccines consisting of HPV L1 VLPs generate high anti L1 serum neutralizing antibody
concentrations and in clinical trials have shown greater than 95 per cent efficacy against both benign and
neoplastic genital HPV associated disease. These vaccines are delivered intramuscularly and therefore
circumvent the immune evasion strategies of the virus.
Key words Antibody - cell mediated immunity - human papillomavirus - prophylactic vaccine - VLPs
Introduction
the host. Host defence is a partnership between innate
immunity (phagocytes, soluble proteins e.g., cytokines,
complement and epithelial barriers) together with
adaptive immunity (antibody, cytotoxic effector cells).
In simple terms, the innate immune system detects the
pathogen and acts as first line defence clearing (it is
estimated) up to 90 per cent of microbial assaults alone1.
Innate immunity has no specific memory but crucially
activates the appropriate adaptive immune response
From the standpoint of the evolutionary
microbiologist, papillomaviruses are very successful
infectious agents. They induce chronic infections that
have no apparent systemic sequellae and rarely kill the
host, but periodically shed large amounts of infectious
virus for transmission to naïve individuals. To achieve
this successful lifestyle, HPVs must either avoid or
negotiate the powerful immune defence systems of
266
STANLEY: IMMUNE RESPONSE TO HUMAN PAPILLOMA VIRUS
that generates both lethal effector responses of exquisite
specificity for, and long lived-cells with, memory for
the insult. Thus, the adaptive responses of antibody
mediated humoral immunity clear free virus particles
from body fluids and can prevent re-infection by virus,
those of cell mediated immune (CMI) responses are
essential for the clearance of virus infected cells. Innate
immunity is alerted by cell injury and stress or cell death,
phenomena that activate the innate sensors such as Toll
like receptors and the inflammasome and manifested
by inflammation (the local vascular response to injury).
In the inflammatory process soluble and cellular innate
immune effectors are recruited and local parenchymal
cells and phagocytes (both recruited and local) are
activated to secrete inflammatory cytokines and other
defence molecules that in turn recruit more cytotoxic
effectors to the inflammatory focus. Crucially dendritic
cells in the periphery are activated to kick start the
adaptive immune response by presenting antigen to
naïve T cells in the draining lymph node. How this
marvelous defence system is recruited to respond to
HPV infections and how the virus ducks and weaves to
avoid it is the subject of this brief review.
HPVs are exclusively intra-epithelial
The exclusively intra-epithelial life cycle of HPVs
is central to understanding the host response. Virus
infects basal keratinocytes probably via micro-abrasions
of the epithelial surface that leave the basal lamina
intact2. All subsequent events in the viral life cycle are
tightly linked to the differentiation programme of the
keratinocyte as it progresses up through the epithelium3.
The terminal events that result in genome encapsidation,
viral assembly and maturation of infectious virus occur
in the most superficial differentiated cells of squamous
epithelium. This intra-epithelial life cycle has some key
features that impact on the recognition and response of
the host immune system to papillomaviruses. Firstly
no inflammation accompanies viral infection and thus
there is no danger signal to alert the innate immune
sensors. HPVs are not lytic viruses the life cycle is
played out in the keratinocyte a cell destined for death
from natural causes and high level viral replication
and viral assembly occur in terminally differentiated
keratinocytes, cells that have already undergone a
regulated death programme. Secondly, although HPVs
appear to be able to bind to and enter cells other than
keratinocytes, viral gene expression and viral protein
synthesis are confined to keratinocytes. There is no
synthesis of viral protein in antigen presenting cells.
Finally there is either no or very little viraemia. Virus
267
infects via microabrasions that leave the basal lamina
intact and is shed from mucosal or cutaneous surfaces
far from vascular channels. Thus, there is poor access
to the draining lymph nodes where adaptive immune
responses are initiated.
Immune responses to HPV
Regressing genital warts
In view of these impediments, one might well
ask whether there is an immune response to HPV but
evidence from a range of sources shows that there is.
Spontaneous regression is a feature of both cutaneous
and ano-genital warts and immunohistological analysis
of this phenomenon is informative. Non-regressing
genital warts are characterised by a lack of immune
cells, the few intra-epithelial lymphocytes present are
CD8 T cells and mononuclear cells are present mainly
in the stroma. Histological examination of regressing
genital warts reveals a large infiltrate into the wart
stroma and epithelium of T cells (both CD4+ and
CD8+) and macrophages4. The infiltrating lymphocytes
express activation markers, the cytokine milieu is
dominated by pro-inflammatory cytokines such as
IL-12, TNF-α and IFN-γ5 and there is upregulation
of the adhesion molecules required for lymphocyte
trafficking on the endothelium of the wart capillaries6.
These appearances are characteristic of a cell mediated
Th1 biased immune response.
Natural animal infections
Cross sectional clinical studies provide only a
snapshot of what is a dynamic process and ethical and
practical considerations inhibit longitudinal studies
in humans. However, in animal models of mucosal
papillomavirus infection such as the canine oral
papillomavirus (COPV) the immunological events of
the entire wart cycle from infection to regression can
be followed. In COPV infections wart regression is
accompanied by a cellular infiltrate similar to that seen
in regressing cutaneous and genital warts7. Systemic
T cell responses directed to E2 and E6 peptides can be
detected at low frequency at distinct time points during
the infectious cycle8. These responses occur in narrow
time windows that coincide with periods of viral DNA
amplification and are maximal at the time of wart
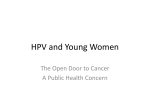
regression thereafter declining quite rapidly. Serum
neutralising antibody to the major capsid protein L1
can be detected at or just after wart regression (Fig. 1)
with peak titres 2-3 wk post wart clearance9. Serum
antibody concentrations even at peak are modest and
268
INDIAN J MED RES, September 2009
Fig. 1. The immune response to COPV infection. Panel 1 shows wart progression and regression in experimental infection in the mouth with
COPV in 2 beagle dogs. Warts became visible 5 wk after infection and grew rapidly to reach their greatest diameter at 8 wk. Regression was rapid
and lesions disappeared by 10 wk post infection. Panel 2 shows that anti-COPV L1 serum IgG was just detectable at week 8 but by week 11-12
peak antibody concentrations were achieved. Regression is preceded at week 7-8 post infection by migration into the stroma and wart infected
epithelium of CD4+ T cells, principally a T cells followed by a smaller subset of CD8+ T cells (Panel 2 and 3).
Source: Ref. 9.
slowly decline in the following weeks and months but
animals remain resistant to challenge with large doses
of infectious virus even in the absence of detectable
serum antibody.
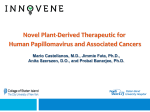
Epidemiological and natural history studies
Epidemiological and natural history studies10
strongly suggest that the course of events in HPV
infections follow a similar pattern11 (Fig. 2). Virtually
all natural history studies show that genital HPV
infection (as determined by detection of HPV DNA
in cervico-vaginal lavages) is extremely common
in young sexually active women with a cumulative
prevalence of 60-80 per cent12. Most of these HPV
infections “clear” i.e., DNA for that specific HPV type
can no longer be detected. The time taken to clearance
for the hrHPVs particularly HPV 16 seems on average
to be 8-16 months, considerably longer than the 4-8
months reported for the low risk HPVs13. However
if the immune response fails to clear or control the
infection then a persistent infection, often with focally
high levels of hrHPV DNA is established and it is this
cohort of individuals that have an increased probability
of progression to high grade cervical intra-epithelial
neoplasia (CIN 2/3) and invasive carcinoma10,14,15.
Cell mediated immunity to HPV
The increased incidence and progression of HPV
infections in immunosuppressed individuals illustrates
the critical importance of the CD4 T cell regulated
cell mediated immune response in the resolution and
control of HPV infections16,17. HIV infected patients
show multiple recurrences of cervical HPV infections18
and an increased incidence of both of cutaneous and
genital warts19 that appears to reflect an increased risk
of progression from sub clinical to clinical disease.
Prospective studies show prolonged persistence of
hrHPV DNA in HIV infected 13-18 yr old girls who
are otherwise healthy20 and a high incidence of CIN2/3
in this group21. Importantly the risk for incident CIN in
these HIV infected girls appeared to be due primarily to
the persistence of low grade squamous intra-epithelial
neoplasia (LSIL), rather than the persistence of hrHPV
DNA without a detectable lesion, implying that florid
STANLEY: IMMUNE RESPONSE TO HUMAN PAPILLOMA VIRUS
269
in these responses30. In a longitudinal study of women
with PCR determined cervical HPV 16 infection
lack of CTL response to E6 but not E7 correlated
with persistent HPV infection suggesting that a CTL
response to HPV 16 E6 is important for viral clearance
and, by implication, neoplastic progression31.
Fig. 2. The natural course of genital infection. Source: Ref. 11.
viral gene expression in a persistent active infectious
cycle is important in progression22.
CD4 T cell responses
There is increasing evidence that, as in COPV, CD4
T cell responses to E2 and, probably E6 are important at
least in hrHPV infections. A non intervention follow up
study of women with cytological evidence of low grade
CIN, showed that HPV16 E2-specific T cell responses,
as measured by specific IL-2 release in vitro, occurred
frequently at the time of lesion clearance23. Good Th1
type immunity against the E2 and E6 protein has been
detected in healthy individuals with no clinical signs
of HPV16 infection24. Importantly, these Th1 type
responses were found only occasionally in high-grade
CIN patients and were impaired in cervical cancer
patients25. In a longitudinal study extending over 12
months of women with histologically diagnosed CIN 1
systemic CD4+ responses to E2 were detected in HPV
16+ histological regressors but were absent in HPV
16+ histologcal progressors. No E2 specific responses
were found in patients with high grade CIN2/3 at the
time of recruitment (Woo, van der Burg and Stanley,
unpublished observations). These data suggest that
a hall mark of effective immune control of HPV 16
infection in the cervix is the generation of CD4+ cells
specific for E2.
Cytotoxic effectors
Cell mediated cytotoxicity is the most important
effector mechanism for the control and clearance of
viral infections and is implemented by a range of cells
both antigen specific cytotoxic T cells (CTL) and the
so called “innate lymphocytes” a heterogeneous group
that includes natural killer (NK) cells, γδ T cells and
invariant natural killer T cells (iNKT). HPV specific
CTL can be detected in patients with previous26 or
ongoing HPV infection27-29. Both CD4+ and CD8+
cytotoxic effectors have been shown to be involved
NK cells are key components of the innate immune
response to viral infections. They are a sub-set of
lymphocytes that kill virally infected or tumour cells
lacking surface expression of MHC Class I molecules
and there is evidence that they are important in HPV
infections. Abnormal NK cell function correlated
with more frequent recurrence of disease in children
with RRP32. A subset of patients with severe combined
immunodeficiency followed up over the long term
post haemopoietic stem cell transplantation33 exhibited
severe cutaneous papillomatosis associated with either
common γc receptor cytokine subunit or Janus kinase-3
(JAK-3) deficiency. A common consequence of such
signalling defects is natural killer cell deficiency and
indeed NK cell counts were lower in these patients.
PBMC from patients with active HPV 16 neoplastic
disease display a reduced NK cell activity against HPV
16 infected keratinocytes34,35. Large numbers of γδ T
cells migrate into regressing papillomas induced by
BPV36 but there are no published data showing that
these cells form a significant infiltrate in regressing
HPV induced lesions37.
Humoral immune responses
Numerous serological studies using HPV virus
like particles (VLPs) have shown that infection with a
genital HPV is followed eventually by sero-conversion
and type specific antibody to the major viral coat protein
L1; antibody to the minor viral coat protein L2 is not
detectable in natural infections in animals or humans38.
Sero-conversion most frequently occurs between 6
and 18 months after the first detection of HPV DNA
in subjects with persistent HPV infection i.e. detection
of HPV DNA of the same type on two occasions at
least 6 months apart39-41 and rarely in subjects with
incident HPV infections i.e., detection of HPV DNA on
only one occasion42. However, as in animal infections,
antibody concentrations are low even at the time of
sero-conversion. Furthermore not all HPV infected
subjects sero-convert and 20-50 per cent of women
with HPV DNA do not have detectable type specific
anti- HPV antibodies although this statement must be
qualified by the fact that the current serological assays
are relatively insensitive41,43. The modest humoral
response is not surprising since there is no blood born
270
INDIAN J MED RES, September 2009
phase of infection and free virus particles are shed
from the surface of squamous epithelia with poor
access to vascular and lymphatic channels and hence
to lymph nodes where immune responses are initiated.
Anti-HPV L1 antibodies however persist for many
years and 10 years post the first detection of HPV
DNA approximately 20-25 per cent of women remain
antibody positive. A controversial issue is whether
these low levels of anti-L1 antibody protect against reinfection with the same HPV type44. This question is not
easy to address. There is increasing evidence that HPV
is not cleared when lesions regress but as in COPV45,
CRPV46 and BPV47 infection remains in a latent state
in a few basal keratinocytes48-50. The detection of HPV
DNA of the same type in a sero-positive individual
may therefore reflect reactivation of latent virus rather
than re-infection. Only if the “new” HPV DNA can be
shown to be distinct in sequence from the HPV DNA
originally detected can re-infection be proven.
HPV avoids host defences
Why HPV infection remains ignored or undetected
by the immune system for so long is a central question.
HPV infections are exclusively intra-epithelial and,
theoretically, HPV attack should be detected by
the professional APC of squamous epithelia, the
Langerhans cell (LC). The activated LC should then
migrate to the draining lymph node, processing HPV
antigens en route, present antigen to naïve T cells in
the node that then differentiate into armed effector
cells, migrate back to the infected site and destroy the
infected keratinocytes.
This cycle of events is deflected in a number of
ways. The infectious cycle of HPV is in itself an
immune evasion mechanism inhibiting host detection of
virus. HPV replication and release does not cause cell
death since the differentiating keratinocyte is already
programmed to die and this “death by natural causes”
does not act as a danger signal in the infected site. Thus,
for most of the duration of the HPV infectious cycle
there is little or no release into the local milieu of proinflammatory cytokines important for DC activation
and migration and the central signals to kick start the
immune response in squamous epithelia are absent51.
There is no blood borne phase of the HPV life cycle
and only minimal amounts of replicating virus are
exposed to immune defences and, in effect, the virus
is practically invisible to the host - a viral strategy
that results in persistent, chronic infections as the host
remains ignorant of the pathogen for long periods.
Virus capsid entry is usually an activating signal
for dendritic cells but there is evidence that Langerhans
cells are not activated by the uptake of HPV capsids.
Langerhans cells, when incubated with L1 virus like
particles (VLPs) of HPV16 do not initiate epitope
specific immune responses against L1 derived antigens52.
In contrast, stromal dendritic cells are activated by VLP
and stimulate HPV specific T cells53-55. Studies in TLR
4 (Toll like receptor) deficient mice suggests that TLR4
contributes to the recognition of HPV 16 VLP by stromal
DC56,57.
Interference with Interferon
For most of the duration of the HPV infectious
cycle there is little or no release into the local milieu
of pro-inflammatory cytokines important for dendritic
cell activation and migration and the essential signals
to kick start the immune response in squamous
epithelia are absent11. However, even in the absence
of viral induced cytolysis and cell death, HPV infected
keratinocytes should be activated to induce type 1
interferon responses - a powerful, generic, anti-viral,
defence system. The type 1 interferons, IFN-α and
IFN-β, have antiviral, antiproliferative anti-angiogenic
and immunostimulatory properties acting as a bridge
between innate and adaptive immunity activating
immature DC58. Most DNA viruses have mechanisms
for inhibiting interferon synthesis and signalling and
the papillomaviruses are no exception.
High risk HPV infection downregulates IFN-α
inducible gene expression and the HPV16, E6 and
E7 oncoproteins directly interact with components
of the interferon signalling pathways (see 59). Thus,
E7 inhibits IFN-α mediated signal transduction by a
binding to P48/IRF-9 preventing translocation to the
nucleus, thereby inhibiting the formation of the ISGF3 transcription complex that binds ISRE (interferon
specific response element) in the nucleus60. E7
interferes with intermediate IFN mediated signals also
by physically associating with IRF-1 inhibiting IRF1 mediated activation of the interferon-β promoter
recruiting histone deacetylase to the promoter, thereby
preventing transcription61. In vivo expression of HPV18
E7 results in reduced expression of IRF-1 target gene
such as TAP1, IFN-β and MCP-1 by inhibition of the
transactivating function of IRF-162. The E6 protein
of HPV also targets the interferon pathway. E6 binds
to IRF-3 and inhibits its transcript activation function
thereby preventing transcription of IFN-α messenger
RNA63. E6 binds to TYK2 preventing binding to the
STANLEY: IMMUNE RESPONSE TO HUMAN PAPILLOMA VIRUS
cytoplasmic portion of the IFN receptor inhibiting
phosphorylation of TYK2, STAT1, STAT2 impairing
JAK STAT activation and therefore inhibiting
specifically IFN-α mediated signalling64. DNA
microarray analysis of gene expression shows that
HPV16 alters expression of 3 groups of genes,
interferon response genes, NF-κB stimulated genes
and cell cycle regulation genes65-67. E6 decreases
expression of IFN-α and β, downregulates nuclear
STAT-1 protein and decreases binding of STAT1 to the
ISRE. E6 and E7 therefore directly alter expression
of genes that enable host resistance to infection and
immune function.
One can conclude that HPV efficiently evades the
innate immune response and delays the activation of the
adaptive immune response but eventually the defences
are activated the infection is controlled and immune
memory to that specific HPV type is established.
There are risks to the host of such a strategy since the
host DC’s are exposed to low levels of viral proteins
in a non-inflammatory milieu for a protracted time
period and local immune non-responsiveness may be
established in the infected mucosa. In this milieu that
is operationally HPV antigen tolerant, host defences
could become irrevocably compromised, HPV antigen
specific effector cells may either not be recruited to the
infected focus or their activity could be down regulated
or both. Thus, if during a persistent high risk HPV
(hrHPV) infection there is deregulation of hrHPV E6
and E7 with increased protein expression this might not
result in an armed effector CMI response but rather the
dominance of T regulatory cells68,69. In consequence,
progression to high grade CIN and invasive carcinoma
would not be impeded.
Prophylactic HPV vaccines
It might well have been thought that since the
antibody response in natural infections was so modest
that vaccines that generate serum neutralizing antibodies
would not be effective. However, some of the earliest
experimental work in rabbits using CRPV, showed very
clearly that neutralizing antibodies were protective70. In
these experiments, if rabbits were infected systemically
with CRPV by direct injection of virus into the muscle
or bloodstream, papillomas did not arise on the skin of
the challenged animals, but neutralizing antibodies were
generated and the animals were completely resistant
to viral challenge by abrasion of the epithelium. This
and other data suggested very strongly that generating
neutralizing antibodies to virus capsid proteins would
be an effective prophylactic vaccine strategy and this
has proved to be so. Two HPV L1 VLP vaccines have
271
been developed ; Cervarix®, a bivalent HPV 16, 18
VLP vaccine from GlaxoSmithKline and Gardasil®
also known as Silgard, a quadrivalent HPV 16/18/6/11
vaccine from Merck Vaccines. These products are to
be delivered in a 3 shot immunisation schedule and
induce, at their peak after the third immunisation at 6
months, high concentrations of neutralizing antibodies
to L1 and virtually all subjects in the vaccine trials
have seroconverted71,72. These vaccines are delivered
intramuscularly, resulting in rapid access of antigen
to the local lymph nodes, thus circumventing the
immune avoidance strategies of the viral intraepithelial
infectious cycle. Furthermore, HPV L1 VLPs are highly
immunogenic, inducing potent antibody responses in
the absence of adjuvant73 due to their ability to activate
both innate and adaptive immune responses. VLPs are
rapidly bound by myeloid DCs and B lymphocytes,
and signal via the toll-like receptor dependent pathway
MYD74,75 which is essential for B cell activation and
antibody generation in mice and probably also in
humans.
The currently available vaccines have been shown
to be highly efficacious in the various Phase II and
Phase III randomized control trials (RCTs) achieving
over a 5 year period 100 per cent protection against
HPV 16/18 caused high grade cervical intra-epithelial
disease (CIN2/3) in 15-26 year old women naïve for
HPV 16 and/or 18 at trial entry50,76,77. Currently, the
best assumption is that the mechanism of protection
elicited by VLPs is serum antibodies. The most
unequivocal evidence for this notion comes from
experiments in rabbits and dogs78-80 in which it was
shown that naïve animals passively immunized with
purified serum IgG from either VLP immunized or
naturally infected animals were completely protected
against high viral challenge. The mechanism by which
neutralizing antibodies to HPV prevent viral entry is at
present speculative. However, new data on virus entry
to cells suggest different stages at which neutralizing
antibodies could be effective. Recent studies have
shown that HPV infection requires a micro abrasion
of the squamous epithelium that results in epithelial
denudation but retention of the epithelial basement
membrane2. HPV initially binds by a primary receptor
to this exposed basement membrane before entering
the keratinocyte, presumably as the keratinocyte
migrates along the basement membrane to repair the
small wound. This is a protracted process extending
over 24 to 48 h, during which it is speculated the virus
capsid undergoes conformational changes that expose
the secondary receptor by which the virus binds to and
272
INDIAN J MED RES, September 2009
enters the keratinocyte81. Virus neutralizing antibodies
could act therefore, by binding to the receptors or by
binding to the capsid and preventing the conformational
distortion essential for successful viral entry. Probably
both types of antibodies are generated after VLP
immunization, but in general, higher concentrations
of blocking antibodies (anti-receptors) are needed
for neutralization compared with those preventing
conformational changes. This is of interest since it
implies that relatively low concentrations of the latter
would be needed for protection and is consistent with
observations from animal papillomavirus studies. For
example, in the dog and rabbit79,82 low concentrations
of anti L1 antibodies provide long-term protection
against high doses of challenge virus. Detectable anti
L1 antibody persists in vaccinated subjects at least
over 5 years in most vaccinees but HPV 18 antibody
concentrations fall to background levels in about 20
per cent of subjects immunised with the quadrivalent
vaccine71. However, efficacy against HPV 18
associated CIN2/3, AIS and VIN/VaIN3 remains at 100
per cent over a 4 year period irrespective of antibody
level and attack rates of HPV 18`in the placebo group
remain constant over this time (Ault 2007, personal
communication).
Mathematical modelling of the kinetics of antibody
decay indicates that antibody (at least for yeast derived
HPV 16 VLPs) could persist for 30 years83 and crucially
there is good evidence that robust immune memory is
generated by these vaccines. The quadrivalent vaccine
has shown an impressive recall response to antigen
challenge, the functional read out for memory, 5
years post immunisation84 and circulating B memory
cells can be detected 1 month after the third and final
immunisation with the bivalent vaccine85. Furthermore,
the persistence of antibody levels in excess of that found
in natural infection strongly suggests robust B and T
memory induction. Immune memory is fundamental
to successful immunisation and the observations of
persistence of antibody and robust recall from the
VLPs in the trials leads to optimism that the duration
of protection might be measured in decades as for
example has been shown for in hepatitis B sub unit
vaccines86.
Cross protection
In natural HPV infections, the detectable
neutralizing antibody responses are type specific, but
HPV L1 VLP vaccines generate not only type specific
but cross-reactive and cross-neutralizing antibodies87.
Both commercial prophylactic vaccines have now
shown evidence of cross-protection, or protection
against non-vaccine HPV types. The high antibody
concentrations generated by the vaccines probably
explain this phenomenon. In general, the population of
antibodies produced in response to a particular antigenic
stimulus such as a VLP, is heterogeneous. Most antigens
are structurally complex, containing many different
epitopes or antigenic determinants. The immune system
responds to the antigen by producing antibodies to
most of the accessible epitopes. Thus, in any response
to a specific protein there will be several populations of
antibodies; the overall antibody response is polyclonal
or heterogeneous and it comprises the output of all the
individuals’ stimulated B cells. Epitopes recognized
by B cells are usually a confirmation and these B cell
epitopes are only displayed by proteins in the native or
tertiary structure. Complex proteins such as L1 contain
multiple overlapping epitopes, some of which are
immunodominant, that is, they induce a more profound
and stronger response in the host than other epitopes
and therefore dominate the polyclonal response. This
can be seen quite clearly in the antibody response to
HPV L1 VLPs. The immunodominant antibodies are
type-specific antibodies but there are, subpopulations
of other antibodies, some of which will be to epitopes
shared by other HPV types. In natural infections, the
antibody concentrations generated are low so that
only the immunodominant species is detected, but in
VLP immunized individuals, antibody concentrations
are high and the subpopulations of cross-reactive and
cross-neutralizing can therefore be detected in sero
assays37. These subpopulations are present at antibody
concentrations one to two logs lower than the dominant
type-specific neutralizing antibodies87. Not every
individual will generate cross-neutralizing antibodies
since immunodominance is complex.
Summary
HPV infection in the genital tract is common
in young sexually active individuals, the majority
of whom clear the infection without overt clinical
disease. However most of those who develop benign
lesions eventually mount an effective CMI response
and the lesions regress. Regression of ano-genital
warts is accompanied histologically by a CD 4+ T cell
dominated Th1 response, animal models support this
and provide evidence that the response is modulated
by CD4+ T cell dependent mechanisms. Failure to
develop effective CMI to clear or control infection
results in persistent infection and, in the case of the
STANLEY: IMMUNE RESPONSE TO HUMAN PAPILLOMA VIRUS
hrHPVs, an increased probability of progression to
CIN3 and invasive carcinoma. The central importance
of the CD4+ T cell population in the control of HPV
infection is shown by the increased prevalence of HPV
infections and HGSIL in individuals immunosuppressed
as a consequence of HIV infection. The prolonged
duration of infection associated with HPV seems to be
associated with effective evasion of innate immunity
as reflected in the absence of inflammation during virus
replication, assembly and release, and down regulation
of interferon secretion and response thus delaying the
activation of adaptive immunity.
273
canine oral papillomavirus infection: host immunity, virus
characterization, and experimental infection. Virology 1999;
265 : 365-74.
10. Moscicki AB, Schiffman M, Kjaer S, Villa LL. Chapter 5:
Updating the natural history of HPV and anogenital cancer.
Vaccine 2006; 24 (Suppl 3): S42-51.
11. Stanley M. Immune responses to human papillomavirus.
Vaccine 2006; 24 (Suppl 1): S16-22.
12. Schiffman M, Kjaer SK. Chapter 2: Natural history of
anogenital human papillomavirus infection and neoplasia.
J Natl Cancer Inst Monogr 2003; (31) : 14-9.
13. Trottier H, Franco EL. The epidemiology of genital human
papillomavirus infection. Vaccine 2006; 24 Suppl 1 : S1-15.
Serum neutralising antibody to the major capsid
protein L1 usually develops after the induction of
successful cell mediated immunity and these antibody
and cell mediated responses are protective against
subsequent viral challenge in natural infections in
animals. Prophylactic vaccines consisting of HPV
L1 VLPs generate high anti L1 serum neutralizing
antibody concentrations and in clinical trials have
shown greater than 95 per cent efficacy against both
benign and neoplastic genital HPV associated disease.
These vaccines are delivered intramuscularly and
therefore circumvent the immune evasion strategies of
the virus.
14. Ho GY, Bierman R, Beardsley L, Chang, CJ, Burk RD. Natural
history of cervicovaginal papillomavirus infection in young
women. N Engl J Med 1998; 338 : 423-8.
References
18. Fruchter RG, Maiman M, Sedlis A, Bartley L, Arrastia CD.
Multiple recurrence of cervical intraepithelial neoplasia in
women with the human immunodeficiency virus. Obstet
Gynecol 1996; 87 : 338-44.
1. Medzhitov R, Janeway CAJ. Innate immunity: the virtues of
a non-clonal system of recognition. Cell 1997; 91 : 295-8.
2. Roberts JN, Buck CB, Thompson CD, Kines R, Bernardo
M, Choyke PL, et al. Genital transmission of HPV in a
mouse model is potentiated by nonoxynol-9 and inhibited by
carrageenan. Nat Med 2007; 13 : 857-61.
3. Doorbar J. The papillomavirus life cycle. J Clin Virol 2005; 32
(Suppl 1): S7-15.
4. Coleman N, Birley HD, Renton AM, Hanna NF, Ryait BK,
Byrne M, et al. Immunological events in regressing genital
warts. Am J Clin Pathol 1994; 102 : 768-74.
5. Stanley MA, Scarpini C, Coleman N. Cell mediated immunity
and lower genital tract neoplasia. RCOG monograph; 2003.
6. Coleman N, Stanley MA. Characterization and functional
analysis of the expression of vascular adhesion molecules in
human papillomavirus-related disease of the cervix. Cancer
1994; 74 : 884-92.
7. Nicholls PK, Moore PF, Anderson DM, Moore RA, Parry NR,
Gough GW, et al. Regression of canine oral papillomas is
associated with infiltration of CD4+ and CD8+ lymphocytes.
Virology 2001; 283 : 31-9.
8. Jain S, Moore RA, Anderson DM, Gough GW, Stanley MA.
Cell-mediated immune responses to COPV early proteins.
Virology 2006; 356 : 23-34.
9. Nicholls PK, Klaunberg BA, Moore RA, Santos EB, Parry
NR, Gough GW, et al. Naturally occurring, nonregressing
15. Liaw KL, Hildesheim A, Burk RD, Gravitt P, Wacholder S,
Manos MM, et al. A prospective study of human papillomavirus
(HPV) type 16 DNA detection by polymerase chain reaction
and its association with acquisition and persistence of other
HPV types. J Infect Dis 2001; 183 : 8-15.
16. Benton, EC, Arends, MJ. Human papillomavirus in the
immunosuppressed. In. Lacey C, editor. Papillomavirus
reviews: Current research on papillomaviruses. Leeds: Leeds
University Press; 1996. p. 271-9.
17. Palefsky JM, Gillison ML, Strickler HD. Chapter 16: HPV
vaccines in immunocompromised women and men. Vaccine
2006; 24 (Suppl 3) : S140-6.
19. Fennema JSA, Van Ameijden EJC, Coutinho RA, Van den Hock
AJAR. HIV, sexually transmitted diseases and gynaecologic
disorders in women: Increased risk for genital herpes and
warts among HIV-infected prostitutes in Amsterdam. AIDS
1995; 9 : 1071-8.
20. Moscicki AB, Ellenberg JH, Farhat S, Xu J. Persistence
of human papillomavirus infection in HIV-infected and
-uninfected adolescent girls: risk factors and differences, by
phylogenetic type. J Infect Dis 2004; 190 : 37-45.
21. Moscicki AB, Ellenberg JH, Crowley-Nowick P, Darragh TM,
Xu J, Fahrat S. Risk of high-grade squamous intraepithelial
lesion in HIV-infected adolescents. J Infect Dis 2004; 190 :
1413-21.
22. Moscicki AB, Ellenberg JH, Farhat S, Xu J. Persistence
of human papillomavirus infection in HIV-infected and
-uninfected adolescent girls: risk factors and differences, by
phylogenetic type. J Infect Dis 2004; 190 : 37-45.
23. de Jong A, van der Burg SH, Kwappenberg KM, van der Hulst
JM, Franken KL, Geluk A, et al. Frequent detection of human
papillomavirus 16 E2-specific T-helper immunity in healthy
subjects. Cancer Res 2002; 62 : 472-9.
24. Welters MJ, de Jong A, van den Eeden SJ, van der Hulst JM,
Kwappenberg KM, Hassane S, et al. Frequent display of
human papillomavirus type 16 E6-specific memory t-Helper
cells in the healthy population as witness of previous viral
encounter. Cancer Res 2003; 63 : 636-41.
274
INDIAN J MED RES, September 2009
25. Welters MJP, van der Logt P, van den Eeden SJF, Kwappenberg
KMC, Drijfhout JW, Fleuren GJ, et al. Detection of human
papillomavirus type 18 E6 and E7-specific CD4+ T-helper 1
immunity in relation to health versus disease. Int J Cancer
2006; 118 : 950-6.
39. Wideroff L, Schiffman MH, Nonnenmacher B, Hubbert N,
Kirnbauer R, Greer CE, et al. Evaluation of seroreactivity
to human papillomavirus type 16 virus-like particles in an
incident case-control study of cervical neoplasia. J Infect Dis
1995; 172 : 1425-30.
26. Nakagawa M, Stites DP, Farhat S, Sisler JR, Moss B, Kong F,
et al. Cytotoxic T lymphocyte responses to E6 and E7 proteins
of human papillomavirus type 16: relationship to cervical
intraepithelial neoplasia. J Infect Dis 1997; 175 : 927-31.
40. Carter JJ, Wipf GC, Hagensee ME, McKnight B, Habel LA,
Lee SK, et al. Use of human papillomavirus type 6 capsids
to detect antibodies in people with genital warts. J Infect Dis
1995; 172 : 11-8.
27. Evans CA, Bauer S, Grubert T, Brucker C, Baur S, Heeg K,
et al. HLA-A2-restricted peripheral blood cytolytic T
lymphocyte response to HPV type 16 proteins E6 and E7 from
patients with neoplastic cervical lesions. Cancer Immuno
Immunther 1996; 42 : 151-60.
41. Carter JJ, Koutsky LA, Wipf GC, Christensen ND, Lee SK,
Kuypers J, et al. The natural history of human papillomavirus
type 16 capsid antibodies among a cohort of university women.
J Infect Dis 1996; 174 : 927-36.
28. Alexander M, Salgaller ML, Celis E, Sette A, Barnes WA,
Rosenberg SA, et al. Generation of tumor-specific cytolytic T
lymphocytes from peripheral blood of cervical cancer patients
by in vitro stimulation with a synthetic human papillomavirus
type 16 E7 epitope. Am J Obstet Gynecol 1996; 175 : 158693.
29. Evans EM, Man S, Evans AS, Borysiewicz LK. Infiltration
of cervical cancer tissue with human papillomavirus- specific
cytotoxic T-lymphocytes. Cancer Res 1997; 57 : 2943-50.
42. Carter JJ, Koutsky LA, Hughes JP, Lee SK, Kuypers J, Kiviat
N, et al. Comparison of human papillomavirus types 16, 18,
and 6 capsid antibody responses following incident infection.
J Infect Dis 2000; 181 : 1911-9.
43. Kirnbauer R, Hubbert NL, Wheeler CM, Becker TM,
Lowy DR, Schiller JT. A virus-like particle enzyme-linked
immunosorbent assay detects serum antibodies in a majority
of women infected with human papillomavirus type 16. J Natl
Cancer Inst 1994; 86 : 494-9.
30. Nakagawa M, Stites DP, Palefsky JM, Kneass Z, Moscicki
AB. CD4-positive and CD8-positive cytotoxic T lymphocytes
contribute to human papillomavirus type 16 E6 and E7
responses. Clin Diagn Lab Immunol 1999; 6 : 494-8.
44. Viscidi RP, Schiffman M, Hildesheim A, Herrero R, Castle
PE, Bratti MC, et al. Seroreactivity to human papillomavirus
(HPV) types 16, 18, or 31 and risk of subsequent HPV
infection: results from a population-based study in Costa Rica.
Cancer Epidemiol Biomarkers Prev 2004; 13 : 324-7.
31. Nakagawa M, Stites DP, Patel S, Farhat S, Scott M, Hills NK,
et al. Persistence of human papillomavirus type 16 infection
is associated with lack of cytotoxic T lymphocyte response to
the E6 antigens. J Infect Dis 2000; 182 : 595-8.
45. Moore RA, Nicholls PK, Santos EB, Gough GW, Stanley
MA. Absence of canine oral papillomavirus DNA following
prophylactic L1 particle-mediated immunotherapeutic
delivery vaccination. J Gen Virol 2002; 83 : 2299-301.
32. Stern Y, Felipovich A, Cotton RT, Segal K. Immunocompetency
in children with recurrent respiratory papillomatosis:
prospective study. Ann Otol Rhinol Laryngol 2007; 116 : 16971.
46. Amella CA, Lofgren LA, Ronn AM, Nouri M, Shikowitz MJ,
Steinberg BM. Latent infection induced with cottontail rabbit
papillomavirus. A model for human papillomavirus latency.
Am J Pathol 1994; 144 : 1167-71.
33. Laffort C, Le Deist F, Favre M, Caillat-Zucman S, RadfordWeiss I, Debre M, et al. Severe cutaneous papillomavirus
disease after haemopoietic stem-cell transplantation in patients
with severe combined immune deficiency caused by common
gammac cytokine receptor subunit or JAK-3 deficiency.
Lancet 2004; 363 : 2051-4.
47. Campo MS, Jarrett WF, O’Neil W, Barron RJ. Latent
papillomavirus infection in cattle. Res Vet Sci 1994; 56 : 151-7.
34. Cho YS, Kang JW, Cho M, Cho CW, Lee S, Choe YK,
et al. Down modulation of IL-18 expression by human
papillomavirus type 16 E6 oncogene via binding to IL-18.
FEBS Lett 2001; 501 : 139-45.
49. Abramson AL, Nouri M, Mullooly V, Fisch G, Steinberg BM.
Latent human papillomavirus infection is comparable in the
larynx and trachea. J Med Virol 2004; 72 : 473-7.
48. Maran A, Amella CA, Di Lorenzo TP, Auborn KJ, Taichman
LB, Steinberg BM. Human papillomavirus type 11 transcripts
are present at low abundance in latently infected respiratory
tissues. Virology 1995; 212 : 285-94.
35. Lee SJ, Cho YS, Cho MC, Shim JH, Lee KA, Ko KK, et
al. Both E6 and E7 oncoproteins of human papillomavirus
16 inhibit IL-18-induced IFN-gamma production in human
peripheral blood mononuclear and NK cells. J Immunol 2001;
167 : 497-504.
50. Paavonen J, Jenkins D, Bosch FX, Naud P, Salmeron J,
Wheeler CM, et al. Efficacy of a prophylactic adjuvanted
bivalent L1 virus-like-particle vaccine against infection with
human papillomavirus types 16 and 18 in young women:
an interim analysis of a phase III double-blind, randomised
controlled trial. Lancet 2007; 369 : 2161-70.
36. Knowles G, O’Neil BW, Campo MS. Phenotypical
characterization of lymphocytes infiltrating regressing
papillomas. J Virol 1996; 70 : 8451-8.
51. Tindle RW. Immune evasion in human papillomavirusassociated cervical cancer. Nat Rev Cancer 2002; 2 : 59-65.
37. Hong K, Greer CE, Ketter N, Van Nest G, Paliard X. Isolation
and characterization of human papillomavirus type 6-specific
T cells infiltrating genital warts. J Virol 1997; 71 : 6427-32.
52. Fausch SC, Da Silva DM, Rudolf MP, Kast WM. Human
papillomavirus virus-like particles do not activate Langerhans
cells: a possible immune escape mechanism used by human
papillomaviruses. J Immunol 2002; 169 : 3242-9.
38. Dillner J. The serological response to papillomaviruses. Semin
Cancer Biol 1999; 9 : 423-30.
53. Da Silva DM, Fausch SC, Verbeek JS, Kast WM. Uptake of
human papillomavirus virus-like particles by dendritic cells
STANLEY: IMMUNE RESPONSE TO HUMAN PAPILLOMA VIRUS
275
is mediated by Fc{gamma} receptors and contributes to
acquisition of T cell immunity. J Immunol 2007; 178 : 758797.
and upregulate proliferation-associated and NF-kappaBresponsive genes in cervical keratinocytes. J Virol 2001; 75 :
4283-96.
54. Lenz P, Lowy DR, Schiller JT. Papillomavirus virus-like
particles induce cytokines characteristic of innate immune
responses in plasmacytoid dendritic cells. Eur J Immunol
2005; 35 : 1548-56.
68. Kobayashi A, Greenblatt RM, Anastos K, Minkoff H, Massad
LS, Young M et al. Functional attributes of mucosal immunity
in cervical intraepithelial neoplasia and effects of HIV
infection. Cancer Res 2004; 64 : 6766-74.
55. Yang R, Murillo FM, Cui H, Blosser R, Uematsu S, Takeda
K, et al. Papillomavirus-like particles stimulate murine bone
marrow-derived dendritic cells to produce alpha interferon
and Th1 immune responses via MyD88. J Virol 2004; 78 :
11152-60.
69. Adurthi S, Krishna S, Mukherjee G, Bafna UD, Devi U,
Jayshree RS. Regulatory T Cells in a spectrum of HPV-induced
cervical lesions: Cervicitis, cervical intraepithelial neoplasia
and squamous cell carcinoma. Am J Reprod Immunol 2008;
60 : 55-65.
56. Joyce JG, Tung JS, Przysiecki CT, Cook JC, Lehman ED,
Sands JA, et al. The L1 major capsid protein of human
papillomavirus type 11 recombinant virus-like particles
interacts with heparin and cell-surface glycosaminoglycans
on human keratinocytes. J Biol Chem 1999; 274 : 5810-22.
70. Shope RE. Immunization of rabbits to infectious papillomatosis.
J Exp Med 1937; 65 : 607-24.
57. Yang R, Murillo FM, Delannoy MJ, Blosser RL, Yutzy WH
4th, Uematsu S, et al. B lymphocyte activation by human
papillomavirus-like particles directly induces Ig class switch
recombination via TLR4-MyD88. J Immunol 2005; 174 :
7912-9.
58. Le Bon A, Tough DF. Links between innate and adaptive
immunity via type I interferon. Curr Opin Immunol 2002; 14 :
432-6.
59. Kanodia S, Fahey LM, Kast WM. Mechanisms used by human
papillomaviruses to escape the host immune response. Curr
Cancer Drug Targets 2007; 7 : 79-89.
60. Arany I, Goel A, Tyring SK. Interferon response depends
on viral transcription in human papillomavirus-containing
lesions. Anticancer Res 1995; 15 : 2865-9.
61. Park JS, Kim EJ, Kwon HJ, Hwang ES, Namkoong SE,
Um SJ. Inactivation of interferon regulatory factor-1 tumor
suppressor protein by HPV E7 oncoprotein. Implication for
the E7-mediated immune evasion mechanism in cervical
carcinogenesis. J Biol Chem 2000; 275 : 6764-9.
62. Um SJ, Rhyu JW, Kim EJ, Jeon KC, Hwang ES, Park JS.
Abrogation of IRF-1 response by high-risk HPV E7 protein
in vivo. Cancer Lett 2002; 179 : 205-12.
63. Ronco, LV, Karpova, AY, Vidal, M, Howley, PM. Human
papillomavirus 16 E6 oncoprotein binds to interferon
regulatory factor-3 and inhibits its transcriptional activity.
Genes Dev 1998; 12 : 2061-72.
71. Villa LL, Ault KA, Giuliano AR, Costa RL, Petta CA, Andrade
RP, et al. Immunologic responses following administration of
a vaccine targeting human papillomavirus Types 6, 11, 16, and
18. Vaccine 2006; 24 : 5571-83.
72. Harper DM, Franco EL, Wheeler C, Ferris DG, Jenkins D,
Schuind A, et al. Efficacy of a bivalent L1 virus-like particle
vaccine in prevention of infection with human papillomavirus
types 16 and 18 in young women: a randomised controlled
trial. Lancet 2004; 364 : 1757-65.
73. Harro CD, Pang YY, Roden RB, Hildesheim A, Wang Z,
Reynolds MJ, et al. Safety and immunogenicity trial in adult
volunteers of a human papillomavirus 16 L1 virus-like particle
vaccine. J Natl Cancer Inst 2001; 93 : 284-92.
74. Yang R, Murillo FM, Lin KY, Yutzy WH4, Uematsu S, Takeda
K, et al. Human papillomavirus type-16 virus-like particles
activate complementary defense responses in key dendritic cell
subpopulations. J Immunol 2004; 173 : 2624-31.
75. Yan M, Peng J, Jabbar IA, Liu X, Filgueira L, Frazer IH, et
al. Activation of dendritic cells by human papillomavirus-like
particles through TLR4 and NF-kappaB-mediated signalling,
moderated by TGF-beta. Immunol Cell Biol 2005; 83 : 83-91.
76. Ault KA. Effect of prophylactic human papillomavirus L1
virus-like-particle vaccine on risk of cervical intraepithelial
neoplasia grade 2, grade 3, and adenocarcinoma in situ: a
combined analysis of four randomised clinical trials. Lancet
2007; 369 : 1861-8.
77. Future II Study Group. Quadrivalent vaccine against human
papillomavirus to prevent high-grade cervical lesions. N Engl
J Med 2007; 356 : 1915-27.
64. Li S, Labrecque S, Gauzzi MC, Cuddihy AR, Wong AH,
Pellegrini S, et al. The human papilloma virus (HPV)-18 E6
oncoprotein physically associates with Tyk2 and impairs JakSTAT activation by interferon-alpha. Oncogene 1999; 18 :
5727-37.
78. Breitburd F, Kirnbauer R, Hubbert NL, Nonnenmacher B,
Trin-Dinh-Desmarquet C, Orth G, et al. Immunization with
viruslike particles from cottontail rabbit papillomavirus
(CRPV) can protect against experimental CRPV infection. J
Virol 1995; 69 : 3959-63.
65. Alazawi W, Pett M, Arch B, Scott L, Freeman T, Stanley
MA, et al. Changes in cervical keratinocyte gene expression
associated with integration of human papillomavirus 16.
Cancer Res 2002; 62 : 6959-65.
79. Suzich JA, Ghim SJ, Palmer Hill FJ, White WI, Tamura JK,
Bell JA, et al. Systemic immunization with papillomavirus L1
protein completely prevents the development of viral mucosal
papillomas. Proc Natl Acad Sci USA 1995; 92 : 11553-7.
66. Chang YE, Laimins LA. Interferon-inducible genes are
major targets of human papillomavirus type 31: insights from
microarray analysis. Dis Markers 2001; 17 : 139-42.
80. Ghim S, Newsome J, Bell J, Sundberg JP, Schlegel R, Jenson
AB. Spontaneously regressing oral papillomas induce systemic
antibodies that neutralize canine oral papillomavirus. Exp Mol
Pathol 2000; 68 : 147-51.
67. Nees M, Geoghegan JM, Hyman T, Frank S, Miller L,
Woodworth CD. Papillomavirus type 16 oncogenes
downregulate expression of interferon-responsive genes
81. Roberts JN, Buck CB, Thompson CD, Kines R, Bernardo
M, Choyke PL, et al. Genital transmission of HPV in a
276
INDIAN J MED RES, September 2009
mouse model is potentiated by nonoxynol-9 and inhibited by
carrageenan. Nat Med 2007; 13 : 857-61.
types 6/11/16/18 L1 virus-like particle (VLP) vaccine. Vaccine
2007; 25 : 4931-9.
82. Stanley MA, Moore RA, Nicholls PK, Santos EB, Thomsen
L, Parry N, et al. Intra-epithelial vaccination with COPV L1
DNA by particle-mediated DNA delivery protects against
mucosal challenge with infectious COPV in beagle dogs.
Vaccine 2001; 19 : 2783-92.
85. Giannini SL, Hanon E, Moris P, Van Mechelen M, Morel S,
Dessy F, et al. Enhanced humoral and memory B cellular
immunity using HPV16/18 L1 VLP vaccine formulated with
the MPL/aluminium salt combination (AS04) compared to
aluminium salt only. Vaccine 2006; 24 : 5937-49.
83. Fraser C, Tomassini JE, Xi L, Golm G, Watson M, Giuliano
AR, et al. Modeling the long-term antibody response of a
human papillomavirus (HPV) virus-like particle (VLP) type
16 prophylactic vaccine. Vaccine 2007; 25 : 4324-33.
86. Hammitt LL, Hennessy TW, Fiore AE, Zanis C, Hummel KB,
Dunaway E, et al. Hepatitis B immunity in children vaccinated
with recombinant hepatitis B vaccine beginning at birth: a
follow-up study at 15 years. Vaccine 2007; 25 : 6958-64.
84. Olsson SE, Villa LL, Costa RL, Petta CA, Andrade RP, Malm C,
et al. Induction of immune memory following administration
of a prophylactic quadrivalent human papillomavirus (HPV)
87. Smith JF, Brownlow M, Brown M, Kowalski R, Esser MT,
Ruiz W, et al. Antibodies from women immunized with
Gardasil ((R)) cross-neutralize HPV 45 pseudovirions. Hum
Vaccin 2007; 3 : 109-15.
Reprint requests: Prof. Margaret A. Stanley, Department of Pathology, University of Cambridge, Tennis Court Road
Cambridge CB2 1QP, UK
e-mail: [email protected]