Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
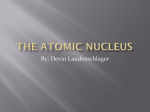
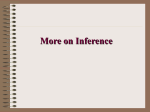
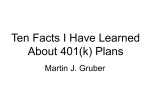
An overview of EEG signal processing algorithms for the detection of EEG biomarkers of treatment response in depression Dr. Reza Rostami Psychiatrist, Associate professor University of Tehran Major depressive disorder (MDD( • A major depressive disorder occurs without a history of a manic, mixed, or hypomanic episode. • A major depressive episode must last at least 2 weeks, and typically a person with a diagnosis of a major depressive episode also experiences at least Five (or more) symptoms from a list that includes: • Depressed mood most of the day, nearly every day • Markedly diminished interest or pleasure in all, or almost all, activities most of the day • Significant weight loss when not dieting or weight gain or increase in appetite • Insomnia or hypersomnia • Psychomotor agitation and retardation • Fatigue or loss of energy • Feelings of worthlessness or excessive or inappropriate guilt • Diminished ability to think or concentrate, indecisiveness • Recurring thoughts of death or suicide Epidemiology Lifetime Prevalence Rates of Depressive Disorders Type Lifetime Major depressive episode Range Average 5-17 12 Dysthymic disorder Range Average 3-6 5 Minor depressive disorder Range Average 10 ---- Recurrent brief depressive disorder Range 16 Burden disease • The World Health Organization predicts depression as the second burden of disease in 2020 (Muray & Lopez, 1996). • Currently depression is the fourth leading cause of disability worldwide (Muray & Lopez, 1996). • The annual cost of depression is 118 million Euros (Sobocki et al., 2006) in Europe and 400 million Dollars (Greenberg et al., 2015) in the United States. • Less than 50% of MDD patients respond to their first consumed antidepressant and only 30% experience full recovery (Trivedi et al., 2006). • Most of the patients experience a long period of trial and error before finding the right antidepressant (Bauer et al., 2007) Types of treatment in depression • • • • • Medication Psychotherapy Combination both Brain stimulation method Alternative medicine The algorithm of treatment selection for Major depressive disorder The percentage reduction of depressive symptoms in varies treatments Main Brain Stimulation Techniques • ECT - Electroconvulsive Therapy ▫ FEAST • rTMS - repeated Transcranial Magnetic Stimulation ▫ Neuronetics, Magstim, Brainsway, Neuralieve, Neostim, Neosync • DBS - Deep Brain Stimulation ▫ RST - Responsive Stimulation Therapy ▫ Epidural Cortical Stimulation • VNS - Vagus Nerve Stimulation • MST - Magnetic Seizure Therapy • tDCS - transcranial Direct Current Stimulation • TENS - transcutaneous Electrical Nerve Stimulation ▫ Cranial Electrical Stimulation (CES) Alpha-stim • EPI-fMRI - echoplanar fMRI • Transcranial pulsed ultrasound What is Vagus Nerve Stimulation (VNS) Therapy? • Mild pulses applied to the left vagus nerve in the neck send signals to the brain • Automatic intermittent stimulation • Simple in-office dose adjustment • Assured treatment adherence • FDA Approved for Epilepsy, Class I evidence From Higgins and George, Brain Stimulation Therapies for Clinicians, 2008, APPI Press. FEAST – Clinical Status • 17 Depressed Patients treated to date ▫ Columbia University (NY), MUSC • Remarkable time to recovery after FEAST (17 min average) • 7 Antidepressant remitters, 5 of last 8 • Continued development underway What is TMS? • Electrical current flowing through a coil induces a magnetic field • Scalp and skull are transparent to magnetic fields • Alternating magnetic fields induce electrical current in underlying brain tissue Overview of TMS 1) Electrical energy in insulated coil on the scalp induces 2) Pulsed magnetic field of about 1.5 Tesla in strength 3) Passes unimpeded through the cranium for 2-3 cm 4) In turn induces a focal electrical current in the brain 5) Get desired local and distal effects on the target neural circuitry 6) Delivered as single pulses or repeated trains (rTMS) How TMS Works George MS. Sci Am. 2003;289:66-73. Coil Type Figure 8 Double Cone Round TMS as a novel treatment for depression Non-invasive, office-based procedure No anesthetic required, awake, alert, no recovery room or nurses, immediate resumption of activities Flexible targeting of treatment possible, device can be moved over surface of the brain and so different circuits and disorders can be targeted Possible advantages of rTMS No cognitive side effects High tolerability generally, better than medication, more precise delivery High patient acceptability, with lack of stigma, although labor intensive Which treatment is better? • Currently a combination of antidepressant medications and psychotherapy is the most effective treatment for depression, while their individual effectiveness equals any Alternative medicine treatment or control group. • Less than 50% of MDD patients respond to their first consumed antidepressant and only 30% experience full recovery. • Most of the patients experience a long period of trial and error before finding the right antidepressant. Biomarkers • A new research scope that has attracted a lot of attention recently is the use of biomarkers to predict the response to treatment. • Different genetic, metabolic, neuroendocrinology, neuroimaging and neurophysiology parameters are proposed as potential biomarkers of response to antidepressant treatment but none has been approved. • One neurophysiologic biomarker of response to treatment which has had promising results is EEG EEG biomarkers • • • • • • • EEG alpha band activity Alpha asymmetry Alpha Peak Frequency EEG theta band activity Antidepressant treatment response index (ATR) Theta cordance Event-related potentials (ERPs) EEG alpha band activity • Pre-treatment changes in the alpha band, that is increased alpha power has been shown to differentiate responders from non-responders. • A possible mechanism involving the right temporoparietal and subcortical regions was to account for the increased alpha power seen in depressed patients who respond to SSRI treatment. • Depression may be related to dysfunction of temporoparietal mechanisms, which may mediate emotional arousal • This biological mechanism has been proposed to play a role in both increased alpha power and alpha asymmetry found in SSRI responders. • Asymmetry in the alpha band characterized by left lateralization has been demonstrated in treatment response with TCAs and the SSRI, fluoxetine. Alpha asymmetry • Inverse relation between alpha power and cortical activity, increased alpha is reflective of reduced cortical activity whereas, decreased alpha reflects increased activity. • While greater left than right hemispheric activation at occipital sites was associated with treatment response, non-responders tended to show the opposite pattern of hemispheric activation (greater right than left) in frontal and posterior regions. Alpha asymmetry in depressed patient • Findings of left lateralizaton are in conflict with reports of reduced left frontal activity (increased alpha activity) in depressed patients. • Explanation 1: Left frontal hypoactivation can be interpreted as a deficit in approach mechanisms, while right frontal hypoactivation can be interpreted as a deficit in withdrawal mechanisms. • Explanation 2: Decreased left prefrontal activation in depression may disinhibit left temporoparietal regions, resulting in enhanced left hemisphere advantage in fluoxetine responders. • Alpha asymmetry in SSRI responders may be reflective of low arousal associated with low serotonergic activity Alpha Peak Frequency • Alpha peak and rCBF: A direct relationship between regional CBF and iAPF has been established, where increased iAPF was associated with increased rCBF, most specifically in the bilateral inferior frontal gyrus (BA 45) and right insular cortex (BA 13). • Alpha peak and cerebral perfusion: A direct relationship between iAPF and cerebral perfusion on one hand and their relationship to the modulation of attention and arousal on the other hand, which are also impaired in both ADHD and depression. • Alpha peak and medication : Given that benzodiazepines have been shown to decrease the iAPF (specifically Carbamazepine, and oxcarbazepine), these studies suggest interplay between the GABAergic system and cerebral blood-flow. Alpha peak and medication • The power spectral plots of non-responders (left) and responders (right) to antidepressant medication at posterior sites. Note the decreased alpha power and lower iAPF (8 Hz) in non-responders. The red line indicates the iAPF pre-treatment and the blue line the iAPF post-treatment. Only responders to medication exhibited an increase in iAPF of approx. 0.5 Hz. Alpha peak and rTMS • Studies have demonstrated that non-responders to rTMS were characterized by a slow iAPF, suggesting regular rTMS is unlikely to be a likely candidate for this sub-group. • One study demonstrated in schizophrenia that rTMS at the iAPF demonstrated better effects on negative symptoms than LF or HF rTMS. Pre treatment Pre treatment (BDI) Pre treatment (CANTAB) Post treatment (After the 10th session) Post treatment (After the 10th session) Post treatment (After the 10th session) Post treatment (After the 20th session) The summary of studies in the field of response to treatment biomarkers(Alpha frequency) in antidepressant Pharmacolo gy Amitriptyline study Ulrich et al ,1984 Pirlindol Clomipramin e Number of Subjects Status of response Changs in EEG Resp . vs Non- Resp 9 5 Resp. vs 4 Non-Resp 11 4 Resp. vs 7 Non-Resp Power decrease in the alpha range (7.5-13 cps)/ power increase of the slower frequencies (2-5 cps)/ higher peak frequency in the alpha range/increase in the peak frequency in the alpha range of about 0.5 cps/ tendency towards a left lateralisation of the occipital alpha power 23 12 Resp. vs 11 Non-Resp Ulrich et al ,1988 22 Maprotiline 7 Resp. vs 15 Non-Resp Paroxetine Knott et al , 2000 70 51 Resp. vs 19 Non-Resp Fluoxetine Bruder et al , 2001 53 34 Resp. vs 19 Non-Resp 18 11 Resp. vs 7 Non-Resp Fluoxetine Early changes in alpha band EEG after the first TCA dose were associated with treatment response at three weeks Bruder et al, 2008 Baseline increases in alpha power and decreases in theta power were detected in responders compared to non-responders to a six-week treatment with paroxetine. EEG alpha asymmetry between brain hemispheres was shown to differentiate responder and non-responder/ Responders had great baseline EEG alpha power at occipital lobe/ responders showed greater alpha over right/ alpha power and asymmetry at occipital lobe showed good predictive ability EEG theta band activity • Studies investigating pre-treatment and early changes in the theta band have reported conflicting results. • Elevated, pre-treatment theta current density, localized by LORETA to the rACC has been associated with response to nortriptyline, citalopram, reboxetine, fluoxetine, or venlafaxine, in depressed patients. • The rACC is a main hub within the default network (DN) of the brain, which is involved in self-focused processing. • Elevated resting state activity in these brain regions is associated with focusing on reflective thought or task-independent introspection such as rumination, remembering and planning. • Pizzagalli (2011) proposes that elevated resting rACC activity may lead to treatment response through adaptive self-referential functions such as mindfulness and non-evaluative self-focus. Default Mode Network Blue : regions that negatively correlate with the default network Red: regions that positively correlate with the default network. rACC as a biomarker response to treatment • Pizzagalli et al (2001): Increased pre-treatment resting rACC theta activity in responders relative to nonresponders (red). • Pizzagalli (2011) further proposes that increased rACC activity associated with treatment response to antidepressants may play a key role in reestablishing the functional connections between the DN and TPN. • several domains of research including neuropsychology, neurophysiology and neuroimaging have demonstrated significant frontocingulate dysfunction in depression. Antidepressant treatment response index (ATR) • Antidepressant Treatment Response Index (ATR) as a composite, threeparameter QEEG index that combines prefrontal EEG theta and alpha power from baseline and week 1. • ATR is a nonlinear combination of three features: relative combined theta and alpha power (3–12 Hz), plus alpha power in two different alpha bands (8.5–12 Hz and 9–11.5 Hz). ATR also includes the change in alpha power from baseline (8.5–12 Hz) and week 1 (9–11.5 Hz). The ATR components Relative theta power Antidepressant treatment response index (ATR) Relative alpha power alpha power in two different alpha bands The summary of ATR studies in the field of response to treatment biomarkers in antidepressant Pharmacology SSRI study Iosifescu et al, 2009 Escitalopram/bupr opion Leutchter et al, 2009 Escitalopram/bupr opion Leutchter et al, 2009 Number of Subjects 82 Status of response Changes in ATR in Resp . vs Non- Resp 45 Resp. vs 37 Non-Resp ATR predicted antidepressant response with 70% accuracy (sensitivity = 82%, specificity = 54%, AUROC = 72%, p = 0.001). 73 38 Resp. vs 35 Non-Resp 375 220 Resp. vs 155 NonResp ATR was useful for predicting differential response to either Escitalopram or bupropion monotherapy. Subjects with high ATR values (above a threshold) were more than 2.4 times as likely to respond to escitalopram as those with low ATR values (68% vs. 28%; p = .001)/ Subjects with ATR values below the threshold who were switched to bupropion treatment were 1.9 times as likely to respond to bupropion alone than those who remained on escitalopram treatment (53% vs. 28%; p = .034). ATR had 74% accuracy (AUROC = 0.77) in predicting both response and remission, whereas clinical parameters or genetic polymorphisms were associated with neither response nor remission Theta cordance • Cordance is a measure that combines EEG absolute and relative power according to a specific formula. • Cordance is computed by a normalization and integration of absolute and relative power values from all electrode sites for a given EEG recording; cordance values are calculated in three steps. • First, EEG power values are computed using a re-attributional electrode montage in which power values from pairs of electrodes that share a common electrode are averaged together to yield the re-attributed power These absolute power values are used to derive relative power (percentage of power in each frequency band) for each electrode. • Second, these absolute and relative power values for each individual EEG recording are normalized across electrode sites, using a z-transformation statistic for each electrode site s in each frequency band f (yielding Anorm (s,f) and Rnorm (s,f) respectively). This normalization process places absolute and relative power values into a common unit (standard deviation or z-score units) which allows them to be combined. These z-scores are based on the average power values in each band for all electrodes within a given EEG recording (i.e., these are not z-scores referenced to a normative population). • Third, the cordance values are formed by summing the z-scores for normalized absolute and relative power (Z(s,f)=Anorm(s,f)+Rnorm(s,f), for each electrode site and in each frequency band). Cordance values have been shown to have higher correlations with regional cerebral blood flow than absolute or relative power alone Cordance Computation CORDANCE(s,f)=(ANORM(s,f)_0.5)+ (RNORM(s,f) _0.5) Electrode site Frequency band Normalized absolute power Normalized relative power • If the site is discordant associated with white-matter lesions, cordance is negative, • If the site is concordant, cordance is positive. The summary of Cordance studies in the field of response to treatment biomarkers in antidepressant Pharmacology study Venlafaxine Number of Subjects Status of response Changes in theta cordance Resp . vs Non- Resp 12 6 Resp. vs 6 NonResp 13 7 Resp. vs 6 NonResp A decrease in prefrontal theta cordance at one week after start of medication was a significant predictor of antidepressant response/ Change in prefrontal theta cordance at one week significantly distinguished medication responders from all other groups 25 13 Resp. vs 12 NonResp Cook et al, 2002 Fluoxetine Venlafaxine/ Fluoxetine Leutchter et al, 2002 SSRI Cook et al, 2005 Prefrontal theta cordance “decrease/no decrease” at one week as a predictor of clinical response (observed at week 8) led to an accuracy of 72% (sensitivity = 69%, specificity = 75%). Of six responders, five showed an early decrease in cordance; only two of the six non-responders showed an early cordance decrease. The predictor yielded an accurate classification for 75% of the subjects 12 6 Resp. vs 6 NonResp Prefrontal theta cordance decreases after one week predicted response with an overall accuracy of 88% (sensitivity = 100%, specificity = 83%) The decrease of prefrontal cordance after week 1 in responders was significant ( p =0.03) Antideppressant Bares et al, 2007 17 5 Resp. vs 12 NonResp venlafaxine Bares et al, 2008 25 12 Resp. vs 13 NonResp Event-related potentials (ERPs) • (ERPs) are a measure of change in voltage, which represent brain activity elicited in response to sensor stimulation (i.e., visual or auditory). • Recorded ERPs comprise distinctive peaks and troughs reflective of positive and negative fluctuations in voltage and are referred to as ‘components’. Different components have been identified and named based on the direction of the waveform deflection (P for Positive and N for Negative) and on the specific time course of the waveform at which, it occurs post-stimulus. • Two ERP components have been the focus of investigation in depression including the P300 (or P3) and the Loudness Dependent Auditory Evoked Potential (LDAEP). The P300 component • The P300 component is measured at 300 msec after presenting an auditory stimulus. • This ERP index is believed to reflect the cognitive processes of attention and auditory processing. • In depressed patients, a delay in the latency of the P300 component has been reported. • Higher amplitude of the P300 wave at occipital sites was associated with treatment response with fluoxetine and a TCA. • Patients who did not remit had longer P300 latency at baseline compared to those who did. • The precise neurobiological basis of the P300 in relation to treatment response is unknown Grand Grand average ERP waveforms for 20 depressed patients and 20 healthy controls to nontarget, target and novel stimuli at midline sites Loudness Dependent Auditory Evoked Potential (LDAEP). • The LDAEP is a measure of the ERP component N1/P2, taken 100-200 msec after presentation of an auditory stimulus. • The amplitude of the waveform changes with increasing loudness of the stimulus. • The LDAEP is thought to relate to the magnitude of 5-HT neurotransmission in the auditory cortex, particularly in the primary auditory cortex. • The majority of studies investigating LDAEP in antidepressant treatment response have divided their samples into a top 50% range (representative of higher slopes; ‘strong’ LDAEP) and bottom 50% range (lower slopes; ‘weak’ LDAEP) based on a median split midpoint. The summary of ERP studies in the field of response to treatment biomarkers in antidepressant Pharmacology Fluoxetine SSRI study Bruder et al, 1995 Kalayam & Alexopoul os, 1999 Number of Subjects 86 49 Paige et al, 1994 17 Fluoxetine Lee et al, 2005 100 SSRI Galliant et al, 2000 29 Reboxetine/citalperam Juckel et al, 2007 35 Reboxetine/citalperam Mulert et al, 2007 20 Reboxetine/citalperam Linka et al , 2009 26 Fluoxetine,buproprion, desipramine Treatment response was associated with higher amplitude of the P300 wave only at the occipital electrodes. Patients who did not remit at six weeks had, at baseline, longer P300 latency than remitted depressed patients and controls. When combining the P300 result with clinical predictors (psychomotor retardation and perseveration), 23 of the 24 remitted depressed patients were correctly identified (sensitivity = 95.8%, specificity = 65.9%). 11 responders to 6 nonresponders after 4 to 8 weeks of treatment with fluoxetine, buproprion, or desipramine; responders had, at baseline, larger slopes of the P2 amplitude as a function of stimulus intensity. At week 4, the HDRS score had declined by 44.3% for the group with strong LDAEP and by 34.4% for the group with weak LDAEP Patients treated with paroxetine, better four-week outcomes (measured by the HAM-D) were present in the half of the sample with “stronger” LDAEP Citalopram responders had a “strong” LDAEP at baseline, whereas responders to reboxetine had a “weak” LDAEP at baseline. Nonresponders to citalopram or reboxetine showed the inverse LDAEP characteristics, respectively Citalopram we found higher LDAEP-values in responders versus non-responders (p<0.05) and a significant correlation between pre-treatment-LDAEP and improvement in the Hamilton score after treatment (r=0.71, p<0.05) High LDAEP being associated with Citalopram response and low LDAEP being associated with reboxetine response.