Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
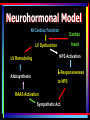
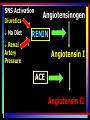
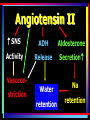
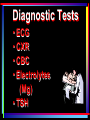
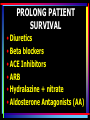
Systolic or Diastolic: What’s the Difference? Cynthia MacDonald, MSN, RN,CS, APRN Adult Nurse Practitioner Low Country Lung & Critical Care Hospitalist – Trident Health System Statistics • 40-60% pts w/ HF have nl LV function, but have diastolic dysfunction • Estimated 15% have mildly abnl sys fx (EF 45-54%) w/ dias dysfunction Public Health Impact • HF w/ preserved EF – better prognosis – 8-9 % mortality 1 yr vs 19% for systolic dysfunction Patient: JS, 70 yo white female CC: SOB Hx: HTN, HLP, GERD Ht: 5’4” Wt: 170 lbs BP: 176/98 Pulse: 112 RR: 16 Meds: atenolol 50mg qday, Zocor 40 mg q hs, omeprazole 40 mg PE: NAD, S1 S2 2/6 murmur LSB, lungs CTA, Abd taut, +HJR, 2+ LE edema Heart Failure Definition • Clinical syndrome • Heart not able to pump blood to meet body’s needs Heart Failure •Systolic – Decreased pumping ability •Diastolic – Relaxation abnormality Systolic Dysfunction • Impaired forward output caused by decreased LV contraction. • Damaged or weakened heart muscle • Hallmark - EF </= 40% Diastolic Dysfunction • Normal EF • Noncompliant, stiff LV • Less able to relax • Interferes with adequate filling; • Raises filling pressures • • • • • • • Coronary Artery Disease Valvular Heart Disease High Blood Pressure Tachycardia induced CMP Myocarditis Sarcoidosis Cocaine abuse Noncardiac Causes • • • • • • • Thyroid Disease OSA Alcohol Abuse Infection Drugs Diabetes Rheum D/O - lupus Diastolic Heart Failure • • • • • • Preserved LV function Signs & Symptoms of HF Abnormal LV Filling Elevated Filling Pressures Impaired response to stress Difficulty tolerating hemodynamic stress – Afib, tachycardia, elevated BP DIASTOLE • 2/3 cardiac cycle • Tachycardia – decrease filling/relaxation time/filling • Afib – lose atrial contraction, reduce LA emptying, LV filling & LV stroke volume Diastolic HF • Ischemia raises LA & pulm venous Pressure; worsens diastolic dysf • Respiratory sx (wheezing, SOB, inability to take a deep breath, & pulm edema “Angina equivalents” • BP Elevation - abrupt, severe, or refractory elevation of BP • Increases LV wall stress decreases myocardial relaxation PATHOPHYSIOLOGY of HEART FAILURE Neurohormonal Model Nl Cardiac Function Cardiac Insult LV Dysfunction NPS Activation LV Remodeling Responsiveness Aldosynthesis to NPS RAAS Activation Sympathetic Act. Natriuretic Peptides ANP - atria BNP - ventricles • Triggered by stretch • Vasodilator, diuretic, natriuretic properties • Inhibits RAAS – suppresses aldosterone, ADH, epinephrine NP System Overwhelmed in Acutely Decompensated Heart Failure Angiotensin II Epinephrine Norepinephrine Endothelin Aldosterone ANP BNP Renin-AngiotensinAldosterone System (RAAS) • Activated by hypoperfused kidneys • Leads to vasoconstriction & volume retention • Renin released by kidney SNS Activation Diuretics Na Diet Angiotensinogen RENIN Renal Artery Pressure Angiotensin I ACE Angiotensin II Angiotensin II SNS ADH Aldosterone Activity Release Secretion Vasoconstriction Water Na retention retention Assessment & Evaluation • Patient History • Physical Exam • Diagnostic Tests Patient: JS, 70 yo white female CC: SOB Hx: HTN, HLP, GERD Ht: 5’4” Wt: 170 lbs BP: 176/98 Pulse: 112 RR: 16 Meds: atenolol 50mg qday, Zocor 40 mg q hs, omeprazole 40 mg PE: NAD, S1 S2 2/6 murmur LSB, lungs CTA, Abd taut, +HJR, 2+ LE edema ========================== Other Questions/Information needed Labs/Tests to order Patient History Symptoms SOB – exertion, nocturnal, orthopnea – sleeps recliner • Fatigue, ↓ exercise tolerance • Edema – LE, abdominal – bloating, pants tight, ↓ appetite • Symptoms of OSA PHYSICAL EXAM • Cardiac exam Heart sounds Heart rhythm • JVD/HJR • Lungs clear/crackles/rhonchi • Abdomen-bloating, taut • Peripheral edema Diagnostic Tests • ECG • CXR • CBC • Electrolytes (Mg) • TSH Echocardiogram • • • • • • • • Evaluate EF, valves, chamber sizes LVH Relaxation abnormality Diastolic Dysfunction Reduced EF Elevated RVSP Pulmonary HTN Wall motion abnormality Treat Sx Meds Low Na Diet Lifestyle Changes Treatment Goals • • • • Relieve Symptoms Control BP Reduce LV afterload Improve cardiac function – • • • • slow/reverse deterioration in myocardial function; slow pathologic remodeling Decrease mortality/extend survival Improve QOL Cost effective treatment Improve self-mgmt skills Treatment Goals • decrease risk of hospitalization • Titrate as tolerated to medication target ranges for optimal clinical benefit • Treatment beyond clinical congestion may improve outcomes • Prevent end organ dysfunction PROLONG PATIENT SURVIVAL • Diuretics • Beta blockers • ACE Inhibitors • ARB • Hydralazine + nitrate • Aldosterone Antagonists (AA) Additional Pharm Therapy • Prevention of arrhythmias • Prevention embolic events • Treatment of Anemia Proven Therapies for Chronic Systolic Heart Failure • • • • • • • Diuretics ACE Inhibitors Angiotensin receptor blockers (ARBs) Beta-blockers Aldosterone antagonists Implantable cardiac defibrillators (ICDs) Cardiac resyncronization therapy (CRT) Bi-ventricular pacemakers • Patient education Systolic Dysfunction • Loop Diuretics (usually double home po dose, give IV • ACE • Beta Blockers • ARBs • Spironolactone • Nitrates • Digoxin (use less) Diastolic Dysfunction Treatment Recommendations • Treat known risk factors (HTN, DM, OSA) • Ventricular rate control for all patients • Drugs for all patients: – Diuretics • Drugs for appropriate patients: – ACEI – ARBs – Beta-Blockers, CCB • Coronary revascularization in selected patients • Restoration/maintenance of sinus rhythm Diastolic Dysfunction • Diuretics - LV filling pressure • Na Restriction • Beta blockers • ACE • ARB • CCB - Verapamil & diltiazem HR & promotes vent. relax Treat Underlying Cause • HTN HR = • Ischemia Filling time • Arrhythmias ?OTC meds w/ • Anemia Ephredrine/ • Fever pseudoephredrine • Tachycardia • Caffeine, Nicotine Clues to Uncontrolled BP • ASYMPTOMATIC • Sx – headache, feels bad, hears heartbeat in ears • Echo findings – LVH, pulm HTN, elevated RVSP, diastolic dysfunction or relaxation abnormality • CXR – Cardiomegaly (CMG) • Look at trends if pt in hospital or if monitoring at home; different times Causes of Inadequate Response Associated conditions • • • • • • • • smoking Obesity High salt/sodium intake sleep apnea insulin resistance Alcohol intake anxiety/panic attacks chronic pain Low Sodium Diet • No salt or high Na seasonings • Accent, MSG, Nature’s seasoning – Meat Tenderizer – Lemon Pepper • Processed foods • Canned goods • Fast Foods • 1.5 - 2 Gm sodium (Na diary) Screen for Sleep Apnea • Epworth sleepiness scale • Do you sleep through the night? • Nocturia • Wakes up tired; Daytime drowsiness • Palpitations (especially at night) • Sleepy when driving • Snoring, gasps, snorts, choking • Ask family members • Irritability • Car accidents/work injuries • Restlessness; Toss & Turn, restless legs Clues to sleep apnea • “Roller Coaster BP” (pt self monitor – take BP at different times) • 3, 4, 5 meds – BP not controlled • Fluid retention problems • Body habitus (don’t be fooled by thin people); Class 3-4 Palate • BS difficult to control • Too tired to exercise • Caffeine, nicotine (diet soda, tea) Mallampati score Health Conditions & OSA • • • • • • • • • Hypertension (roller coaster BP) Palpitations; dysrhythmias A Fib; PAF; A Flutter ↑ risk MI, CVA, SCD, blood clots GERD DM; difficult to control BS Memory, concentration, focus Irritability; depression; bipolar D/O Fibromyalgia Patient: JS, 70 yo white female CC: SOB Hx: HTN, HLP, GERD Ht: 5’4” Wt: 170 lbs BP: 176/98 Pulse: 112 RR: 16 Meds: atenolol 50mg qday, HCTZ 25mg Zocor 40 mg q hs, omeprazole 40 mg PE: NAD, S1 S2 2/6 murmur LSB, lungs CTA, Abd taut, +HJR, 2+ LE edema Na 130, K 2.5, Mg 1.5 Echo – EF 60%. LVH, relaxation abnormality (grade 1 diastolic dysfunction, 1+ MR EKG – NSR, LVH Freq nocturia, wakes up tired, daytime sleepiness, restlessness, no dreaming, memory probs MEDICATIONS TREATMENT OF HEART FAILURE Treatment • Loop Diuretic • ACE • BB - carvedilol, metoprolol succinate, bisoprolol • titrate these up first • add on AA • add hydralazine + nitrate in African Amer - persistent Class III, IV & EF < 40% MEDICATION • Hydralazine - start at 25mg tid & isosorbide dinitrate 20 mg tid target 75mg tid & isosorbide dinitrate 40 mg tid • Women & AA don't benefit as much from ACE • Women benefit same from BB AA may not benefit as much from BB except for carvedilol • CCB - no direct role in treatment of Systolic HF can add on vasoselective CCB such as amlodipine & felodipine neutral effect on mortality Don't recommend ACE, ARB, & AA (as well as no Direct Renin Inhibitor) Oral Agents • • • • • • • • Diuretics (thiazide, loop, K+-sparing) Beta Blockers Calcium channel blockers Angiotensin-converting enzyme inhibitors (ACE I) Angiotensin II receptor blockers (ARB) Adrenergic inhibitors (peripheral, central alpha-antagonists Direct vasodilators (hydralazine, minoxidil, nitrates) Direct Renin Inhibitor (tekturna-aliskiren) DIURETICS • Loop diuretics • Appropriate dosing • Monitor Wt, K, Mg, Na, BUN/Cr • Zaroxolyn – 30 min before loop diuretic • Loop diuretic + HCTZ © CMacDonald 3/00 DIURETICS Thiazides Inhibit active exchange of Cl-Na in the cortical diluting segment of the ascending loop of Henle Cortex K-sparing Inhibit reabsorption of Na in the distal convoluted and collecting tubule Medulla Loop diuretics Inhibit exchange of Cl-Na-K in the thick segment of the ascending loop of Henle Loop of Henle Collecting tubule Adverse effects • Postural • ↑ SNS activation hypotension • neuro• hypokalemia hormonal • hyperglycemia activation (↑ • hyperuricemia renin production & RAAS • Rash • hypomagnesem activation • azotemia ia Electrolyte Replacement • Monitor K, Mg, Na, Cr closely • Careful w/ CRI • Check Mg if hard to get K up •K - > 4 • Mg ≥ 2.0 © CMacDonald 3/00 ACE Inhibitors • Inhibits ACE; Prevents Angiotensin I to Angiotensin II (potent vasoconstrictor) • afterload; BP; • Cardiac output; Renal blood flow • Reduces TPR • Correct volume status • Reverse/limit remodeling • Start low dose; split dose ACE Inhibitors Increases Cardiac Output by decreasing afterload; makes it easier for heart to pump • Suppresses Aldosterone secretion (some) • Still underutilized • Maximize dose • Adverse Effects • Hypotension • Worsening of renal function • Hyperkalemia • Cough • Angioedema • Rash • Neutropenia Beta-Blockers Drug Initial Dose Bisoprolol 1.25 mg/day (Zebeta) Carvedilol* 3.125mg BID (Coreg) Metoprolol* 25 mg/day (Toprol XL) Target Dose 5mg/day (< 85 kg) 10 mg/day (> 85 kg) 25 mg BID (<85kg) 50 mg BID (> 85 kg) 150 – 200 mg/day Beta Blockers HR - filling time • Blood Pressure • Mortality HF & MI • risk of another heart attack • Reverse remodeling; improve function • Caution – asthma, reactive airway disease; not COPD • • • • • sensitivity to catacholamines Prevent LV dilation Negative inotrope Warn pt – will feel worse before feeling better Titrate up slowly; monitor BP & HR Contraindications • Bronchospasm • Advanced heart block • Sinus bradycardia • Cardiogenic shock • Acute pulmonary edema Titration and Adverse Effects • Begin at low doses, if tolerated (2 wk intervals). • Monitor pts. closely –hypotension –edema –worsening heart failure –bradycardia –heart block –bronchospasm Considerations • Stabilize pts. on standard therapy before initiation of beta-blocker • Use with caution in pts. with bradycardia • Careful review of pt. before uptitration of dose • Decrease dose or discontinue if pt. develops worsening heart failure Angiotensin II Receptor Blockers (ARBs) • Blocks Angiotensin II at receptor sites • Dilates blood vessels • Lowers BP • Don’t use before ACE © CMacDonald 3/00 ARBs • SVR • aldosterone & epinephrine secretion • Correct hypovolemia prior to initiating therapy Calcium Channel Blockers • Use Diastolic Dysfunction; not for tx LVSD • Dilates blood vessels & helps to decrease angina • BP • Slow HR in LVDD • Negative inotropy • Diltiazem, verapamil - HR, BP • Amlodipine – BP Calcium Channel Blockers • Diltiazem start 30mg q 6hrs to slow HR & lower BP; titrate up as tolerate & then can change to long acting (120 , 180, 240, 300, 360mg) • Verapamil – 40, 80, 120 mg; tid – Max 480mg/day Aldosterone antagonists • Helps to limit remodeling & fibrosis • Aldactone/spironolactone (start 12.5 to 25 mg/day) • Contraindications: – serum creatinine > 2.5 m/dL – serum K+ > 5.0 mmol/L • Adverse Effects: – worsening renal function, GI upset, hyperkalemia, gynecomastia, rash Spironolactone/Eplerenone • Aldosterone inhibitors • Prevents aldosterone from attaching to receptors • Promotes Na excretion • excretion of K • Decrease/discontinue K • Monitor K, Cr closely • Prevents fluid retention • Used to treat chest discomfort & other symptoms of angina • Dilates blood vessels • More blood flows through coronary arteries to heart. Hydralazine/ Isosorbide Alternative in patients with contraindications or intolerance to ACE Inhibitors • Monitor for side effects • Hydralazine – H/A, tachycardia, fluid retention, lupus, N/V/D • Nitrates - H/A, dizziness, nausea, hypotension • Digoxin force of contraction • blocks sympathetic stimulation (slower HR – treat Afib w/ RVR) • EF < 40-45% • Not used - diastolic dysfunction • Used less for systolic dysfunction • Draw blood 12 hrs after dose • Don’t stop if already on dig Contraindications • Significant sinus or AV block • Bradycardia • Dosing 0.25 mg/day, lower for elderly, renal dysfunction, or potential drug interactions • Monitoring of serum level is controversial Tekturna (Aliskiren) • Direct Renin Inhibitor • Cautious in renal dz, high K • Should not be on ACE, ARB, Renin inhibitor (can be on 2 of these) • Watch Cr • Diarrhea, GERD, hyper K, Elev Cr, BUN, angioedema, hypotension • Not used much now Patient: JS, 70 yo white female CC: SOB Hx: HTN, HLP, GERD Ht: 5’4” Wt: 170 lbs BP: 176/98 Pulse: 112 RR: 16 Meds: atenolol 50mg qday, HCTZ 25mg Zocor 40 mg q hs, omeprazole 40 mg PE: NAD, S1 S2 2/6 murmur LSB, lungs CTA, Abd taut, +HJR, 2+ LE edema Na 130, K 2.5, Mg 1.5 Echo – EF 60%. LVH, relaxation abnormality (grade 1 diastolic dysfunction, 1+ MR EKG – NSR, LVH Freq nocturia, wakes up tired, daytime sleepiness, restlessness, no dreaming, memory probs • Stop HCTZ, replete K & Mg • Chg atenolol to 100 mg bid or change to coreg 6.25-12.5 mg bid or Toprol or diltiazem • Add ACE – Lisinopril (bid dosing if bid dosing w/ BB or CCB) • Daily wts – prn loop diuretic • Can add AA • Refer for sleep eval/study • HR target – 60-70s Patient: JS, 70 yo white female CC: SOB Hx: HTN, HLP, GERD Ht: 5’4” Wt: 170 lbs BP: 176/98 Pulse: 86 RR: 16 Meds: atenolol 50mg qday, HCTZ 25mg Zocor 40 mg q hs, omeprazole 40 mg PE: NAD, S1 S2 2/6 murmur LSB, lungs CTA, Abd taut, +HJR, 2+ LE edema Na 130, K 2.5, Mg 1.5 Echo – EF 30%, 1+ MR EKG – NSR w/ PACs Freq nocturia, wakes up tired, daytime sleepiness, restlessness, no dreaming, memory probs • Stop HCTZ, replete K & Mg • Diurese w/ loop diuretic • Chg atenolol to coreg 6.25-12.5 mg bid • Add ACE – Lisinopril (bid dosing) • Daily wts – prn loop diuretic • Add AA • Refer for sleep eval/study • HR target – 60-70s Cardiac Resynchronization Therapy (CRT) • Criteria QRS >/= 130 msec • Sinus rhythm • EF ≤ 30% • Dysynchony of RV & LV • Improved LV function • Decrease LV volume BiV Pacer • Atrial synchronized biventricular pacing • Correction of electrical = correction of mechanical • Improved coordination of contraction • Improved timing - valve opening & closing BiV Pacer • Pacing leads placed in RA & RV • Specially designed pacing lead passed through coronary sinus into a cardiac vein on left lateral freewall ICD (implantable cardioverter defibrillator) • • • • • • EF < 35 - 40%, cardiac arrest, SCD V Tach or V Fib Inherited heart abnormality Acts as pacemaker if slow HR Defibrillate chaotic rhythm (V Fib) Saves lives What every heart failure patient should know: • • • • • • • Symptoms of heart failure medications names/doses Obtain daily weights Eat a low sodium diet Diagnose OSA/CSA Exercise Weight Loss • Low Na Diet • Fluid Restriction Sodium holds onto fluid Lifestyle changes • Stop Smoking • Lose Weight • Avoid alcohol • Control HTN, Lipids, DM Regular Exercise • Progress slowly; Start with short, frequent intervals • Improved conditioning • Feels better • Perform ADLs END OF LIFE ISSUES • Educate both pt & family – Expected course of illness – Final treatment options • Hospice services • Planning undertaken before pts become too ill to participate in decisions