Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
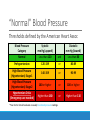
Therapeutic Considerations for Hypertension presented by Jerad Bailey, Pharm D Clinician Resource Click image to download Today’s Guest Speaker Jerad Bailey, Pharm D Lead Pharmacist, Cabin Creek Health Systems BA, Marshall University Pharm D, West Virginia University Therapeutic Considerations for Hypertension PRESENTATION BY JERAD BAILEY, PHARM.D. Presentation Goals Review of blood pressure and the condition “hypertension” Hypertension treatment protocols Therapeutic classes used for the treatment of hypertension Therapeutic effects, side effects, and considerations to be made in the outpatient setting Blood Pressure “Blood pressure (BP) is the force of blood against arterial walls as it circulates through the body.” –Center for Disease Control Systolic BP: Left ventricle is most contracted (high pressure) Diastolic BP: Left ventricle is most relaxed (low pressure) The Cardiac Cycle Blood Pressure Cardiac Output ◦ Heart Rate ◦ Stroke Volume Blood Viscosity Total Peripheral Resistance (TPR) Blood Pressure Heart Rate: The faster the heart beats, the more blood that flows through the circulatory system If each pump moves the same amount of fluid, then faster pumping means greater fluid movement Blood Pressure Stroke Volume: A larger stroke volume allows for more blood to circulate with each heartbeat A full bucket is more effective than a halfempty bucket Blood Pressure Blood Viscosity: Blood that is more viscous (thick) becomes more difficult to circulate A thinner fluid requires less effort to move and flows more freely Blood Pressure Total Peripheral Resistance (TPR): An amount of fluid (blood) flowing through a smaller area is under more pressure than flowing through a larger area Resistance means more work and more pressure “Normal” Blood Pressure Thresholds defined by the American Heart Assoc Blood Pressure Category Systolic mm Hg (upper#) Diastolic mm Hg (lower#) Normal Less than 120 and Less than 80 Prehypertension 120-139 or 80-89 High Blood Pressure (Hypertension) Stage 1 140-159 or 90-99 High Blood Pressure (Hypertension) Stage 2 160 or higher or 100 or higher Hypertension Crisis (Emergency care needed) Higher than 180 or Higher than 110 *Your doctor should evaluate unusually low blood pressure readings. Complications of Hypertension Heart and blood vessels must work harder to overcome pressure Decreased blood perfusion to heart (angina, heart failure, MI) Blockages or burst arteries leading to the brain (stroke) Renal Artery Stenosis (kidney failure) Eighth Joint National Committee More commonly referred to as “JNC 8” Best practices for treatment of hypertension Revised / Revisited 2014 Combination of lifestyle modifications and pharmacotherapeutic interventions Lifestyle Modifications Dietary considerations (low salt) ◦ Less fluid retention Physical activity ◦ Stronger heart and healthier arteries Weight loss ◦ Less work for the heart Smoking cessation ◦ Nicotine acts as a stimulant and can harden arterial walls Stress management Limit use of alcohol ◦ Alcohol weakens cardiac muscle and can cause arrhythmias Starting Pharmacologic Therapy JNC 8 Guidelines Varying goals depending on age and comorbidities Over 60: < 150/90 Under 60: < 140/90 Over 18 and with CKD: < 140/90 Over 18 and with Diabetes: < 140/90 PLEASE NOTE: Guidelines and recommendations are to be used along with physician/clinician judgment and treatment and based on individual patient’s unique needs and circumstances. Therapeutic Options Over a dozen medication classes are indicated to treat hypertension Each class may have more than one medication Combination products are available Where do we begin? First-Line Therapies JNC 8 “Starting Lineup” ◦ Thiazide diuretics ◦ Calcium Channel Blockers (CCB) ◦ Angiotensin-Converting Enzyme (ACE) Inhibitors ◦ Angiotensin Receptor Blockers (ARB) Thiazide Diuretics Hydrochlorothiazide (HCTZ) ◦ Esidrix, Microzide Chlorthalidone ◦ Thalitone Metolazone ◦ Zaroxolyn Indapamide ◦ Lozol Thiazide Diuretics Inhibit sodium and chloride reabsorption in the kidney Creates a diuretic effect Less water in the blood, less work for the heart Thiazide Diuretics Frequent urination Electrolyte imbalance ◦ Hypokalemia, Hypomagnesemia, Hypercalcemia Hyperuricemia ◦ Gout Exacerbation of comorbidities ◦ Hyperglycemia, Hyperlipidemia Skin conditions ◦ Photosensitivity, Rash Renal Failure Thiazide Diuretics Rehydrate Increased sun sensitivity Baseline / periodic labs Calcium Channel Blockers Dihydropyridines Nondihydropyridines Amlodipine Diltiazem ◦ Norvasc Felodipine ◦ Plendil Isradipine ◦ DynaCirc Nicardipine ◦ Cardene Nifedipine ◦ Procardia XL Nisoldipine ◦ Sular ◦ Cardizem, Dilacor, Tiazac Verapamil ◦ Isoptin, Calan, Verelan, Covera Calcium Channel Blockers Calcium Channel Blockers inhibit movement of calcium ions in muscle tissue, aiding in muscle relaxation Dihydropyridines mainly target muscles in arteries, reducing TPR Nondihydropyridines mainly target cardiac muscle, reducing heart rate and contractility Calcium Channel Blockers Fatigue Edema Dizziness Headache Skin conditions ◦ Rash Conductivity issues ◦ AV Block Calcium Channel Blockers Drug-Drug Interactions ◦ CYP 3A4 Substrates Electrocardiogram ACE Inhibitors Benazepril ◦ Lotensin Captopril ◦ Capoten Enalapril ◦ Vasotec Fosinopril ◦ Monopril Lisinopril ◦ Prinivil, Zestril Moexipril ◦ Univasc Quinapril ◦ Accupril Ramipril ◦ Altace Trandolapril ◦ Mavik ACE Inhibitors Angiotensin Converting Enzyme is responsible for converting Angiotensin I to Angiotensin II Angiotensin II is an extremely potent vasodilator ACE Inhibitors prevent this conversion, reducing TPR ACE Inhibitors Dry Cough Dizziness Electrolyte imbalance ◦ Hyperkalemia Skin conditions ◦ Rash Renal Artery Stenosis Angioedema (more common in African-Americans) ACE Inhibitors Pregnancy Category Therapeutic Dosing ◦ Renal Artery Stenosis Therapeutic Duplication (ARB) Angiotensin Receptor Blockers Candesartan Telmisartan ◦ Atacand ◦ Micardis Losartan Eprosartan ◦ Cozaar Irbesartan ◦ Avapro Valsartan (first available January 2015) ◦ Diovan ◦ Teveten Olmesartan (not available) ◦ Benicar Angiotensin Receptor Blockers Blocks the effects of the enzyme Angiotensin II by preventing binding to its receptor Similar end result as patient taking ACE Inhibitor (reduction of TPR), but reduced instances of coughing Angiotensin Receptor Blockers Dry Cough (less often than ACE Inhibitors) Dizziness Electrolyte imbalance ◦ Hyperkalemia Skin conditions ◦ Rash Renal Impairment Upper Respiratory Infections Angioedema (more common in AfricanAmericans) Angiotensin Receptor Blockers Pregnancy Category Therapeutic Duplication (ACE Inhibitors) Newest of the four classes of medications ◦ Most expensive of the four front-line therapies Selecting a First-Line Therapy For the general population, any of these agents are viable If severe hypertension, may start with two therapies African-American ◦ Preference for CCB or Thiazide diuretic, due to increased risk of angioedema with ACE or ARB Chronic Kidney Disease ◦ Preference for ACE or ARB, due to renal protective properties Escalation of Therapy Option 1: Max-out current therapy before adding additional agents Option 2: Add additional agent before maxing-out current therapy If a third therapy is necessary, use the remaining frontline option unless there is a compelling contraindication Once patient has a thiazide diuretic, a CCB, and either an ACE/ARB, resort to secondary therapies to help patient reach goal Backup Therapies Beta-Blockers Loop Diuretics Potassium Sparing Diuretics Alpha-Adrenergic Blockers Vasodilators/Nitrates Alpha Agonists Renin Inhibitor(s) Beta-Blockers Examples include atenolol (Tenormin), carvedilol (Coreg), labetalol (Normodyne), metoprolol (Lopressor, Toprol XL), nadolol (Corgard), and propranolol (Inderal) Blocks central and peripheral beta receptors, which causes decreased heart rate and TPR Side Effects ◦ ◦ ◦ ◦ ◦ Fatigue Decreased exercise tolerance GI upset Hypertriglyceridemia Can mask hypoglycemia Considerations ◦ Exercise intolerance a major issue initially ◦ Pregnancy Category (in 1st Trimester) ◦ Asthma medications (BetaAgonists) Loop Diuretics Includes furosemide (Lasix), bumetanide (Bumex), torsemide (Demadex) Inhibits reabsorption of sodium and chloride throughout renal system, creating a diuretic effect; less water in the blood, less work for the heart Side Effects ◦ Dehydration ◦ Electrolyte imbalance ◦ Hypokalemia ◦ Hyponatremia ◦ Hypomagnesemia ◦ Hyperglycemia Considerations ◦ Fluid overload or renal failure ◦ Interaction with diabetes medications Potassium Sparing Diuretics Includes spironolactone (Aldactone), eplerenone (Inspira), triamterene (Dyrenium), amiloride (Midamor) Side Effects ◦ Dehydration ◦ Cramps ◦ Electrolyte imbalance ◦ Hyperkalemia ◦ GI disturbance ◦ Skin conditions ◦ Rash ◦ Gynecomastia ◦ Sexual dysfunction Decreases sodium reabsorption in the kidney, decreasing water Considerations ◦ Avoid in patients with diabetes, reabsorption and increasing cholesterol, gout potassium retention; less water ◦ Caution when combining with ACE/ARB in the blood, less work for the heart Alpha-Adrenergic Blockers Includes doxazosin (Cardura), prazosin (Minipress), terazosin (Hytrin) Side Effects ◦ Edema ◦ Palpitations ◦ Postural / orthostatic hypotension ◦ Syncope Considerations Blocks alpha-adrenergic receptors, preventing vasoconstriction in arterioles and veins, decreasing TPR ◦ Combine with a diuretic due to edema ◦ May be beneficial to men with BPH ◦ Consider giving at bedtime ◦ Avoid in cardiovascular disease ◦ Drug-drug interactions with PDE5 inhibitors ◦ Viagra, Cialis, Levitra Vasodilators / Nitrates Includes hydralazine (Apresoline) and minoxidil (Loniten) Side Effects ◦ Fluid retention ◦ Tachycardia ◦ Skin Conditions ◦ Dermatitis Causes smooth muscle relaxation in arterioles, decreasing TPR ◦ Peripheral neuropathy ◦ Minoxidil: Hirsutism Considerations ◦ Reserved for treatmentresistant patients ◦ Pair with agents that offset fluid retention and tachycardia Alpha Agonists Includes clonidine (Catapres), guanfacine (Tenex), methyldopa (Aldomet), guanabenz (Wytensin) Side Effects ◦ Bradycardia ◦ Dry mouth ◦ Sedation ◦ Rebound hypertension ◦ Heart block Reduces nerve activity in Considerations sympathetic nervous system, decreasing heart ◦ Last-line therapy ◦ Side effect profile rate and TPR ◦ Adherence Renin Inhibitor(s) Only drug in class is Tekturna (aliskiren) Side Effects ◦ Electrolyte imbalance ◦ Hyperkalemia ◦ Skin conditions ◦ Rash Decreases renin activity, interfering with conversion of Angiotensinogen to Angiotensin I, reducing TPR ◦ Diarrhea ◦ Renal Failure Considerations ◦ Pregnancy category ◦ Avoid in diabetes ◦ Therapeutic duplication (ACE/ARB) References Agency for Healthcare Research and Quality American Heart Association Center for Disease Control Epocrates Joint National Committee, Eighth (JNC 8) National Institute on Alcohol Abuse and Alcoholism Pearson PLC Pharmacy Times HHQI Blood Pressure Resources Cardiovascular Health Part 1: Aspirin as appropriate and Blood pressure control BPIP Fundamental Focus: Blood Pressure Control & Smoking Cessation Patient Videos – Cardiovascular Blood Pressure Control • Blood Pressure Medication Management • How to Check My Own Blood Pressure Thank You! If you have any questions, please contact us at [email protected]. This material was prepared by Quality Insights, the Medicare Quality Innovation Network-Quality Improvement Organization supporting the Home Health Quality Improvement National Campaign, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The views presented do not necessarily reflect CMS policy. Publication number 11SOW-WV-HH-MMD-061915