Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Baker Heart and Diabetes Institute wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Coronary artery disease wikipedia , lookup
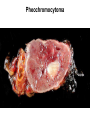
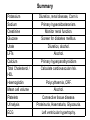
Cardiovascular courses 29th October 2008 Interpreting blood tests and the ECG: practical risk assessment Dr T S Dhanjal PhD MRCP Aims of the talk • Understand why we do blood tests. • What to the blood tests mean? • The importance of risk stratification. • The Electrocardiograph (ECG). Why investigate ? • To detect the secondary causes of hypertension. • Assess for the consequences of hypertension. • Risk stratification to determine overall cardiovascular risk. • Monitoring of treatment. • Detection of disease association. Detection of secondary hypertension Serum Potassium Low Lowish 3.7 – 4.0 Normal High 3.7 – 5.2 mEq/l Hyperaldosteronism Renal Failure Primary (Conn’s) Secondary (RAS) Biochemical Conn’s Serum measurements Potassium Conn’s syndrome Secondary hyperaldosteronism (RAS, renin secreting tumours) Liquorice (11b DHD inhibitor) Liddle’s syndrome Sodium Renin Aldosterone Hyperkalaemia • May develop in Renal Failure. • Drugs – ACE I – ARBs – Potassium sparing diuretics Serum Sodium • High / highish – Primary hyperaldosteronism • Low / lowish – Secondary hyperaldosteronism (Malignant Hypertension or renal disease) – Diuretic overuse Urea & Creatinine • Creatinine – breakdown product of creatine phosphate in muscle. – usually produced at a fairly constant rate by the body. – Filtered by the kidney and not re-absorbed. – If the filtering of the kidney is impaired then blood levels will rise. – Used to determine Creatinine Clearance which estimates the Glomerular Filtration Rate (GFR). Monitoring Creatinine levels • Isolated essential hypertension rarely results in renal impairment. • But concomitant disease (diabetes) or treatment (ACE I / ARB) can exacerbate. • Intrinsic renal disease can cause hypertension. • Serum creatinine only rises with marked damage to nephrons so not a good test to detect early stage kidney disease. • Problem with measuring creatinine clearance is a 24 hour urine collection is required. Is eGFR the answer ? • NSF for renal sevices requires laboratories to estimate GFR using the MDRD formula. • Fundamentally based on serum creatinine measurments so why should it be any better? • Just as sensitive as measuring serum creatinine over time. • BUT variability of eGFR increases as actual GFR improves. Poggio et al 2005 Reciprocal creatinine chart Blood Glucose • Type 2 DM increases risk of cardiovascular, renal, retinal and neuropathic complications. • Screen in hypertensive patients: – Random glucose > 11.1 mmol/l. – OGTT. • Is it more important to aggressively control hypertension ? – UKPDS trials Other serum biochemical tests • Uric acid – 40% of patients with hypertension. – Increased with alcohol, thiazide diuretics. • Liver function tests – Excess alcohol intake. – Steatohepatitis – diabetes, metabolic syndrome. • Serum calcium – Hypocalcaemia secondary to CRF. – Hypertension associated with 1˚ Hyperparathyroidism. – Hypercalcaemia also associated with thiazide diuretics. 24 hour urine collection • Young, thin patients with paroxysmal symptoms. • Urinary metanephrines. – Metabolite of epinephrine created by action of catechol-O-methyl transferase on epinephrine. • Creatinine Clearance using the Cockroft & Galt formula. • Sodium excretion to quantify salt intake. • Degree of proteinuria - renal biopsy ? Pheochromocytoma Haematology • Detection of polycythaemia – Raised RBC, Hb & RBC volume. – Primary (PCV) or secondary (hypoxia). – Gaisbok’s syndrome. • Mean Cell Volume – Increased by alcohol and hypothyroidism. • Connective tissue disease – Platelets, ESR, autoimmune antibodies etc. Lipid profile • For assessment of cardiovascular risk. Cardiovascular risk assessment • JBS 2: Joint British Societies' guidelines on prevention of cardiovascular disease in clinical practice, Heart, 2005. • Prepared by: British Cardiac Society, British Hypertension Society, Diabetes UK, HEART UK, Primary Care Cardiovascular Society, The Stroke Association. • The specific objective to reduce the risk of CVD and its complications in high risk patients. • 3 categories: – Any form of established atherosclerotic CVD. – Diabetes mellitus (type 1 or 2). – Asymptomatic people without established CVD but who have a combination of risk factors which puts them at high total risk (estimated multifactorial CVD risk 20% over 10 years) of developing atherosclerotic CVD for the first time. Measure total cholesterol AND HDL Joint British Societies' cardiovascular disease (CVD) risk prediction chart: non-diabetic men. Prepared by: British Cardiac Society, British Hypertension Society, Diabetes UK, HEART UK, Primary Care Cardiovascular Society, The Stroke Association, Heart 2005;91:v1-v52 Assessment of end-organ damage • Kidneys – Urinalysis. • Microvasculature – Retinopathy. • Heart – ECG. – Echocardiography. Left Ventricular Hypertrophy • LVH is one of the earliest manifestations of hypertensive heart disease. • Leads to diastolic dysfunction and heart failure secondary to systolic dysfunction. • Other cardiac complications: – Myocardial Infarction. – Atrial Fibrillation Electrocardiographic assessment of LVH (1) Sokolow-Lyon index: There are two criteria with these widely used indices: * Sum of S wave in V1 and R wave in V5 or V6 >/= 3.5 mV (35 mm) and/or * R wave in aVL >/= 1.1 mV (11 mm) Cornell voltage criteria – These more recent criteria are based upon echocardiographic correlative studies designed to detect a left ventricular mass index >132 g/m2 in men and >109 g/m2 in women. For men: S in V3 plus R in aVL >2.8 mV (28 mm) For women: S in V3 + R in aVL >2.0 mV (20 mm) Cornell voltage-duration measurement QRS duration×Cornell Voltage > 2440 ms × mV Electrocardiographic assessment of LVH (2) Sensitivity and specificity for selected ECG criteria of LVH Sensitivity (%) Specificity (%) Sokolow Lyon Voltage 22 100 Cornell Voltage Criteria 42 96 Cornell Voltage Duration Criteria 51 95 RaVL > 11 mm 11 100 Romhilt-Estes > 4 points 54 85 Romhilt-Estes > 5 points 33 94 Criterion Summary Potassium Sodium Creatinine Glucose Diuretics, renal disease, Conn’s. Primary hyperaldosteronism. Monitor renal function. Screen for diabetes mellitus. Urate Diuretics, alcohol. LFTs Alcohol. Calcium Primary hyperparathyroidism Total Cholesterol / HDL Calculate cardiovascular risk. Haemoglobin Mean cell volume Polycythaemia, CRF. Alcohol. Platelets Connective tissue disease. Urinalysis Proteinuria, Haematuria, Glycosuria. ECG Left ventricular hypertrophy.