Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
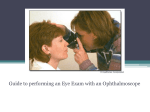
LITERALLY! with Debra Gates BVSc. Most clinics have a direct ophthalmoscope sitting on the bench, but I suspect that many of us are not confident in its use. Most ophthalmoscopes offer a variety of light beams, but for vets the large diameter beam is used routinely as long as the pupil is adequately dilated. Dark adaptation will help with dilation but the best product to use is 1% Tropicamide which is sold by Alcon as Mydriacyl. It takes effect after 20 minutes and lasts 4-5 hours. This is much better than atropine which can leave the pupil dilated for 5-7 days in dogs and horses. The little numbers on the scope can be a bit of a mystery, but relate to the lenses used to focus in different parts of the eye, and accommodate for any optical correction the user may need. Before starting have your patient firmly restrained with a steadying hand under the angle of the jaw and be as systematic as possible in your examination. Begin with the ophthalmoscope on a 0 or +1 diopter setting at arm’s length from the patient as it is easier to pick up lens opacities from there. Gradually move in until you are as close to the eye as you can comfortably get and change to -2 (red 2). This setting will suffice for examination of the disc and fundus in most situations. The fundus will be real and upright and magnified 14x. The bad news is that your field of view will be very narrow and you will have to work systematically to examine the entire eye. Start at the disc and then divide the fundus into quadrants, covering each in turn. The patient’s eye movements will both help and hinder your quest. Like most things it all gets easier with practice. Try to keep both of your eyes open while you perform the examination as it will reduce fatigue. Use your right eye to observe on the left side and vice versa. Indirect ophthalmoscopy utilises a 20 diopter lens and an independent light source to form an inverted and reversed view of the fundus. Your eye, the light-source, lens and patient’s pupil should as far as possible lie in the same axis. Therefore the light is held beside your temple or in front of your nose. Alternately you can use a head-mounted light and keep both hands free. The critical thing though is to have the plane of the indirect lens perpendicular to the lens of the eye. Indirect ophthalmoscopy is undervalued, as the wideangle view is easier to interpret and gives a great deal of information rapidly, but because of lesser magnification (2-4x) it won’t provide as much detail as is gleaned through a direct technique. There are some excellent texts available on ophthalmology, but nothing beats getting in there and learning from doing.