Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Genomic imprinting wikipedia , lookup
Human genome wikipedia , lookup
Oncogenomics wikipedia , lookup
Polymorphism (biology) wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Skewed X-inactivation wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Y chromosome wikipedia , lookup
Behavioural genetics wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Gene therapy wikipedia , lookup
Epigenetics of human development wikipedia , lookup
Dominance (genetics) wikipedia , lookup
Gene expression programming wikipedia , lookup
Gene expression profiling wikipedia , lookup
Point mutation wikipedia , lookup
Genome evolution wikipedia , lookup
Human genetic variation wikipedia , lookup
Genetic engineering wikipedia , lookup
X-inactivation wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
History of genetic engineering wikipedia , lookup
Neocentromere wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Population genetics wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Designer baby wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Medical genetics wikipedia , lookup
Microevolution wikipedia , lookup
Quantitative trait locus wikipedia , lookup
Public health genomics wikipedia , lookup
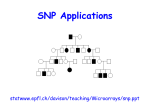
1996 Oxford University Press Human Molecular Genetics, 1996, Vol. 5, No. 8 1193–1197 A ninth locus (RP18) for autosomal dominant retinitis pigmentosa maps in the pericentromeric region of chromosome 1 Su Ying Xu1, Marianne Schwartz2, Thomas Rosenberg3 and Andreas Gal1,* 1Institut für Humangenetik, Universitäts-Krankenhaus Eppendorf, Butenfeld 32, D-22529 Hamburg, Germany, of Clinical Genetics, Department of Pediatrics, Rigshospitalet, Copenhagen, Denmark and 3National Eye Clinic for the Visually Impaired, Hellerup, Denmark 2Section Received April 16, 1996; Revised and Accepted May 24, 1996 We studied a large Danish family of seven generations in which autosomal dominant retinitis pigmentosa (adRP), a heterogeneous genetic form of retinal dystrophy, was segregating. After linkage had been excluded to all known adRP loci on chromosomes 3q, 6p, 7p, 7q, 8q, 17p, 17q and 19q, a genome screening was performed. Positive lod scores suggestive of linkage with values ranging between Z = 1.58–5.36 at θ = 0.04–0.20 were obtained for eight loci on proximal 1p and 1q. Close linkage without recombination and a maximum lod score of 7.22 at θ = 0.00 was found between the adRP locus (RP18) in this family and D1S498 which is on 1q very near the centromere. Analysis of multiply informative meioses suggests that in this family D1S534 and D1S305 flank RP18 in interval 1p13–q23. No linkage has been found to loci from this chromosomal region in six other medium sized adRP families in which the disease locus has been excluded from all known chromosomal regions harbouring an adRP gene or locus suggesting that there is (at least) one further adRP locus to be mapped in the future. INTRODUCTION Retinitis pigmentosa (RP) designates a frequent but heterogeneous genetic form of retinal dystrophy affecting ∼1 in 3000 people and responsible for the visual handicap of ∼1.5 million individuals worldwide (for references and review, see 1,2). The condition can be inherited as an autosomal dominant, autosomal recessive or X-linked trait, whereas a considerable portion are simplex cases in which the pattern of inheritance remains undetermined. Typical clinical symptoms of RP include night blindness, reduced visual acuity and progressive loss of peripheral vision leading to blindness usually after the fourth decade. Ophthalmological examinations show constricted visual fields, attenuated vessels and abnormal accumulation of pigment in the retina. *To whom correspondence should be addressed Autosomal dominant retinitis pigmentosa (adRP) accounts for ∼20% of all RP cases and is characterized by significant allelic and non-allelic heterogeneity (for references and review, see 1,3). Eight loci for adRP have been mapped genetically to date on chromosomes 3q, 6p, 7p, 7q, 8q, 17p, 17q and 19q (for review, see 4 and references therein, and 5). Of the eight corresponding adRP genes, those on 3q and 6p encode rhodopsin (for review, see 1 and references therein) and peripherin (for review, see 6 and references therein), respectively. Here we report the mapping of a further adRP locus (RP18) on the pericentric region of human chromosome 1. RESULTS We studied a large Danish adRP family of seven generations (Fig. 1). Clinical diagnosis was based on a history of night blindness, typical ocular fundus with peripheral bone spicule formation and severe constriction of the retinal arterioles, and progressive visual field defects beginning as mid-peripheral ring scotomas. Disease manifestation was rather uniform, with both sexes equally affected. Twelve subjects had one or several eye examinations performed at the National Eye Clinic, including full field electroretinography (ERG) and dark adaptometry a.m. Goldmann Weekers. Many of the patients claimed that night blindness was present ‘from birth’ on. Nevertheless, pathological dark adaptation starting with a prolonged mesopic phase and elevation of the fully dark-adapted threshold did not occur until the end of the first decade. Atrophy of the retinal pigment epithelium with typical bone spicule hyperpigmentation was also observed from the second half of the first decennium. From the beginning of the second decade, the ERG showed abolished rod responses and strongly attenuated cone responses with prolonged implicit times. ERG was extinguished from the beginning of the third decade if measured by conventional techniques. Visual field defects progressed during the third and fourth decades, leaving the central area relatively spared. Accordingly, visual acuity remained above 0.3 in the majority of patients for the first three decades. Most of the affected subjects had myopia in the range of –2 to –4 diopters, but a few cases with slight hypermetropia or high myopia were also encountered. Some of the patients developed a moderate 1194 Human Molecular Genetics, 1996, Vol. 5, No. 8 Figure 1. Pedigree of RP110. Genotypes detected at the four loci given are arranged according to most likely haplotypes. The disease phenotype of individuals VI.7, VI.8 and VII.1 is unknown. Arrowheads mark the two meiotic breakpoints used to map the disease locus. photophobia; glaucoma was diagnosed in three patients in their sixties. Complicating cataracts were observed as fine subcapsular opacifications which did not require lensectomy. Some of the older patients were totally blind from the age of 80. After linkage had been excluded to all known adRP loci (data not shown), a genome screening was performed. Over 150 DNA polymorphisms of the CA repeat type were analysed. Positive lod scores suggestive of linkage were detected with two reference loci of the Mappairs set (Research Genetics, Inc., Huntsville, AL, USA; Screening Set/Weber Version 4a), D1S534 on 1p and D1S1167 on 1q (Table 1 and Fig. 2). In order to localize the disease locus (RP18) more precisely, the family was genotyped for a total of eight additional ‘anonymous’ DNA polymorphisms from this chromosomal region (7). This analysis provided significant positive lod scores, Zmax ranging between 2.19 and 7.22, for five loci on 1q (Table 1). Close linkage without recombination and a maximum lod score of 7.22 at θ = 0.00 was found in this family between RP18 and D1S498, which is on 1q very near the centromere (ref. 8 and Fig. 2). One or more recombinants were seen with all other loci tested. Figure 1 shows the genotype of all family members at D1S498 as well as at D1S534 and D1S305 which are, respectively, the closest proximal and distal markers to D1S498 analysed. Genotypes are arranged according to the most likely haplotypes. Two recombinants define the interval in which RP18 maps in this family. Individual V.10 is affected by RP and recombinant for D1S534 but non-recombinant for D1S498 and D1S305, which places RP18 centromeric to D1S534 on 1p or on 1q. Individual VI.6, too, is affected by RP and is recombinant for D1S305 but not for D1S498 and D1S534, which maps RP18 centromeric to D1S305 on 1q or on 1p. All data together suggest that in this family D1S534 and D1S305 flank RP18 in interval 1p13–q23 (Fig. 2). In this chromosomal region, there are two genes of particular interest regarding RP, which encode two different G protein α-subunits, GNAT2 (guanine nucleotide-binding protein, α-transducing, polypeptide-2; ref. 9) and GNAI3 (guanine nucleotide-binding protein, α-inhibiting, polypeptide-3; ref. 10). Both genes have been mapped to 1p13 by in situ hybridization (11) with human cDNA probes. However, no data were available on the position of these two genes on the genetic map of chromosome 1. Therefore, and using the genomic sequence published earlier, we have designed oligonucleotide primers for PCR amplification and single strand conformation polymorphism (SSCP) analysis to detect DNA polymorphisms in the 5′ end of GNAI3 suitable for linkage analysis. Two different two-allele restriction fragment length polymorphisms (RFLPs) have been identified which are both due to single base substitutions at nucleotide positions –72 and –61 (numbering as given in ref. 10) and can be detected easily by restriction digestion analysis of PCR products by BanI and BpuI, respectively (see Materials and Methods). 1195 Human Acids Molecular Genetics, Vol.No. 5, No. Nucleic Research, 1994,1996, Vol. 22, 1 8 1195 Table 1. Two-point lod scores between the adRP locus (RP18) and 11 loci from chromosome 1 Physical locationa Loci Recombination faction (θ) Zmax θ (zmax) Cytogenetic Mb 0.000 0.01 0.05 0.10 0.20 0.30 0.40 D1S188 – 103.73 –∞ –8.59 –4.03 –2.33 –1.06 –0.68 –0.45 0.00 0.50 GNAI3 p13 – –∞ –0.95 0.31 0.71 0.78 0.52 0.17 0.81 0.16 D1S534 – 112.36 –∞ 5.11 5.35 5.05 4.08 2.85 1.42 5.36 0.04 D1S498 – – 7.22 7.09 6.56 5.88 4.43 2.85 1.20 7.22 0.00 D1S305 – 139.56 –∞ 2.18 3.23 3.36 2.92 2.07 0.98 3.37 0.09 D1S176 – 144.20 –∞ 1.76 2.73 2.78 2.25 1.40 0.49 2.81 0.08 SPTA1 q21 146.31 –∞ 0.45 1.60 1.86 1.74 1.29 0.67 1.88 0.12 CRP q21–q23 146.58 –∞ 1.05 1.54 1.57 1.27 0.82 0.36 1.58 0.08 D1S1167 – – –∞ 2.02 3.64 3.93 3.51 2.57 1.30 3.93 0.10 D1S104 q21–q23 150.71 –∞ 0.79 1.92 2.18 2.02 1.52 0.83 2.19 0.12 D1S196 – 152.23 –∞ –1.28 –0.03 0.38 0.57 0.48 0.27 0.57 0.20 1p 1cen 1q aData taken from references 8, 9 and 11. We have genotyped members of the family for the two above-mentioned RFLPs. In order to increase informativity, individual genotypes obtained for each of the polymorphisms were combined into haplotypes which were then used in linkage analysis. Haplotypes are shown in Figure 1. Clearly, haplotype 2 is co-segregating with the disease phenotype in this family. However, individual V.10, an affected male, inherited haplotype 3 from his affected mother, i.e. he is recombinant for GNAI3. This finding formally excludes GNAI3 as a candidate gene for the adRP segregating in this family. As V.10 is non-recombinant for D1S498 and D1S305, these data place GNAI3 proximal to both marker loci. Individual V.13, too, is recombinant for the GNAI3 versus RP18 linkage relationship. As this person is non-recombinant for D1S534 and for D1S498, all these data taken together map GNAI3 telomeric to D1S534 on 1p. Pairwise lod scores between RP18 on one hand and D1S534 and GNAI3 on the other hand reach their maximum at, respectively, θ = 0.04 and θ = 0.20 (Table 1). As GNAI3 recombines with D1S534 at a frequency of ∼0.15 (Z = 1.152 in this family; data not shown), results of the two-point analyses are in line with the suggested map position of GNAI3. DISCUSSION The data presented in this communication strongly suggest that a gene implicated in autosomal dominant RP maps in the pericentromeric region of chromosome 1. On a recent integrated map including physical and genetic data (8), D1S534 and D1S305, the two loci flanking RP18, are placed <30 Mb apart, which defines the maximal size of the critical region and corresponds to about one-ninth of the total length of chromosome 1. RP18 represents the ninth locus for the autosomal dominant form of RP assigned by linkage analysis and confirms the extreme non-allelic genetic heterogeneity of the trait. It is not yet known what proportion of patients with RP have mutations in the corresponding gene on chromosome 1. Both linkage studies on Figure 2. Schematic presentation of the order of marker loci typed and the most likely position of the adRP locus (RP18) mapped in the pericentromeric region of chromosome 1. families and screening of larger collections of individual patients suggest that mutations of rhodopsin and peripherin account for, respectively, ∼25 and 5% of all adRP cases (for review see, 1196 Human Molecular Genetics, 1996, Vol. 5, No. 8 respectively, 1 and 6 and references therein). In contrast, the majority of the remaining seven adRP loci have each been assigned in a single large family or have been detected in a few families (for references and review, see 1,4,12). We have found no linkage to the corresponding marker loci on chromosome 1 in six other medium sized adRP families in which the disease locus has been excluded from all known chromosomal regions harbouring an adRP gene or locus (unpublished results). Therefore, it is likely that there is—at least—one further adRP locus to be mapped in the future. We have found two recombinants between GNAI3 and RP18 which practically excludes the possibility that a mutation in GNAI3 is the primary genetic cause of the disease in this family. As both recombinants were in individuals affected by RP, phenotypic misclassification due to reduced penetrance can also be rejected. GNAT2 encodes the α-subunit of a retina-specific transducin expressed exclusively in cone photoreceptors (9). Transducin is a heterotrimeric (α,β,γ) protein whereas the α-subunit defines both the specificity for interaction with the receptor and the effector function. Stimulated receptor activates transducin/the α-subunit by catalysing the exchange of the α-bound GDP for GTP and the dissociation of the α-subunit from the β- and γ-subunits (for review, see 11 and 13 and references therein). As RP affects primarily the rod photoreceptors, we consider that the probability is low that the disease segregating in the Danish family is due to a mutation in GNAT2, although formal proof is missing. Independent support for this assumption comes from the observation that mammalian G protein α-subunit genes belong to a multigene family thought to be generated by a series of genome duplications during evolution. A recent model hypothesizes that GNAT2 and GNAI3 evolved from a single ancestral gene by a subsequent tandem duplication (11), i.e. that the two genes are physically linked. A similar pair of G protein α-subunit genes (GNAT1 and GNAI2) has been found on chromosome 3p21 (11). Given the fact that in the Danish family GNAI3 maps ∼20 cM from RP18 and under the assumption of close physical proximity of GNAI3 and GNAT2 in 1p13 on one hand and in view of the expression of GNAT2 in cone photoreceptor cells on the other hand, our data suggest that GNAT2 is a very unlikely candidate for the gene mutated and responsible for the adRP in the Danish family described here. Molecular genetic and biological analysis of other candidate genes from this chromosomal region (8), e.g. KCNA3 (potassium voltage-gated channel) or NGFB (nerve growth factor) will be carried out to prove or disprove their role in the pathogenesis of this form of retinal dystrophy. MATERIALS AND METHODS Family RP110 Medical files on affected members of the seven-generation kindred studied here (Fig. 1) were retrieved from the Danish Retinitis Pigmentosa Register (14). Autosomal dominant inheritance was documented by several instances of male-to-male transmission. Penetrance seems to be complete as no case of a skipped generation was observed. The whole study was carried out in accordance with the Helsinki Declaration II and approved in advance both by the Danish National Register Authority (Registertilsynet) and the Scientific Ethical Committee (KF 01–226/93). Informed, written consent was obtained from all participants. Molecular genetic analysis Blood samples for linkage analyses were obtained from 20 patients, eight unaffected relatives older than 21 and therefore considered as not affected, three unaffected relatives below the age of 20 and thus classified with disease phenotype unknown, and six spouses. Experimental procedures for genotyping were carried out following standard protocols. Detection of allelic fragments was done by silver staining essentially as described elsewhere (15). Linkage analysis was performed with the Liped program (16). For PCR amplification of a 293 bp DNA segment from the 5′ end of the GNAI3 gene, oligonucleotide primers GNAI3-5′F (5′-GCCA-CCGCCCAGCAATAGAC-3′) and GNAI3-5′R (5′-CCCGACCAGACCCCGTTCAG-3′) were designed based on published sequence data (10). SSCP analysis and direct sequencing of PCR products of aberrant electrophoretic mobility were carried out as described elsewhere (15). Single-base substitutions were found at nucleotide positions –72 (T→C) and –61 (C→T). The T/C and C/T changes result in gain of a recognition site for BanI and BpuI and allelic cleavage products of 293/273 + 20 and 293/260 + 33 bp, respectively. Allele frequencies for linkage analysis were calculated from the genotypes of eight spouses in the family. ACKNOWLEDGEMENTS The experimental work described here was financially supported by the Deutsche Forschungsgemeinschaft. The Danish Retinitis Pigmentosa Register received grants from the Danish Association of the Blind (DBS) whereas blood sampling was financially supported by Cykelhandler P. Th. Rasmussens og Hustru Alma Rasmussens Mindelegat. REFERENCES 1. Gal, A., Apfelstedt-Sylla, E., Janecke, A.R. and Zrenner, E. (1996) Rhodopsin mutations in inherited retinal dystrophies and dysfunction. In Osborne, N.N. and Chader, G.J. (eds), Progress in Retinal and Eye Research. Pergamon Press, in press. 2. Haim, M., Holm, N.V. and Rosenberg, T. (1992) Prevalence of retinitis pigmentosa and allied disorders in Denmark. I. Main results. Acta Ophthalmol., 70, 178–186. 3. Haim, M. (1993) Retinitis pigmentosa: problems associated with genetic classification. Clin. Genet., 44, 62–70. 4. Dryja, T.P. and Li, T. (1995) Molecular genetics of retinitis pigmentosa.Hum. Mol. Genet., 4, 1739–1743. 5. Bardien, S., Ebenezer, N., Greenberg, J., Inglehearn, C.F., Bartmann, L., Goliath, R., Beighton, P., Ramesar, R. and Bhattacharya, S.S. (1995) An eighth locus for autosomal dominant retinitis pigmentosa is linked to chromosome 17q. Hum. Mol. Genet., 4, 1459–1462. 6. Molday, R.S. (1994) Peripherin/rds and rom-1: molecular properties and role in photoreceptor cell degeneration. In Osborne, N.N. and Chader, G.J. (eds), Progress in Retinal and Eye Research. Pergamon Press, pp. 271–298. 7. Gyapay, G., Morissette, J., Vignal, A., Dib, C., Fizames, C., Millasseau, P., Marc, S., Bernardi, G., Lathrop, M. and Weissenbach, J. (1994) The 1993–94 Généthon human genetic linkage map. Nature Genet., 7, 246–339. 8. Forabosco, P., Collins, A. and Morton, N.E. (1995) Integration of gene maps: updating chromosome 1. Ann. Hum. Genet., 59, 291–305. 9. Morris, T.A. and Fong, S-L. (1993) Characterization of the gene encoding human cone transducin α-subunit (GNAT2). Genomics, 17, 442–448. 10. Itoh, H., Toyama, R., Kozase, T., Tsukamoto, T. Matsouka, M. and Kaziro, Y. (1986) Presence of three distinct molecular species of Gi protein α subunit. Structure of rat cDNAs and human genomic DNAs. J. Biol. Chem., 263, 6656–6664. 1197 Human Acids Molecular Genetics, Vol.No. 5, No. Nucleic Research, 1994,1996, Vol. 22, 1 8 1197 11. Wilkie, T.M., Gilbert, D.J., Olsen, A.S., Chen, X-N., Amatruda, T.T., Korenberg, J.R., Trask, B.J., de Jong, P., Reed, R.R., Simon, M.I. Jenkins, N.A. and Copeland, N.G. (1992) Evolution of the mammalian G protein α subunit multigene family. Nature Genet., 1, 85–91. 12. Xu, S., Nakazawa, M., Tamai, M. and Gal, A. (1995) Autosomal dominant retinitis pigmentosa locus on chromosome 19q in a Japanese family. J. Med. Genet., 32, 915–916. 13. Wittinghofer, A. (1994) The structure of transducin Gαt. More to view than just Ras. Cell, 76, 201–204. 14. Haim, M., Holm, N.V. and Rosenberg, T. (1992) Population survey of retinitis pigmentosa and allied disorders in Denmark. Completeness of registration and quality of data. Acta Ophthalmol., 70, 165–177. 15. Bunge, S., Fuchs, S. and Gal, A. (1996) Simple and nonisotopic methods to detect unknown gene mutations in nucleic acids. In Adolph, K.W. (ed.), Methods in Molecular Genetics. Academic Press, Orlando, FL, Vol. 8, pp. 26–39. 16. Ott, J. (1974) Estimation of the recombination fraction in human pedigrees: efficient computation of the likelihood for human linkage studies. Am. J. Hum. Genet., 26, 588–597.