Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Jatene procedure wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
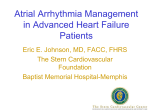
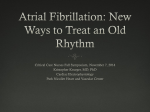
CLINICAL RESEARCH Europace (2013) 15, 1574–1580 doi:10.1093/europace/eut088 Ablation for atrial fibrillation Catheter ablation in selected patients with depressed left ventricular ejection fraction and persistent atrial fibrillation unresponsive to current cardioversion Agustı́n Bortone 1*, Pénélope Pujadas-Berthault 1, Nicole Karam2, Eric Maupas 1, Jean-Marc Boulenc 1, Philippe Rioux1, Nicolas Dürrleman 3, Vlad Ciobotaru 1, and Eloi Marijon 1,2 1 Département de Rythmologie, Unité de Cardiologie, Hôpital Privé Les Franciscaines, Nı̂mes, France; 2Paris Cardiovascular Research Center, Paris, France; and 3Unité de Chirurgie Cardio-Vasculaire et Thoracique, Hôpital Privé Les Franciscaines, Nı̂mes, France Received 28 November 2012; accepted after revision 18 March 2013; online publish-ahead-of-print 12 April 2013 Aims In congestive heart failure (CHF) patients with persistent atrial fibrillation (AF), direct current cardioversion (DCC) may reveal participation of tachycardiamediated process to left ventricular (LV) dysfunction by restoring sinus rhythm (SR). However, if DCC fails to restore SR, patients’ management remains challenging. The aim of the study was to assess the AF catheter ablation benefit in a selected group of CHF patients with LV ejection fraction (LVEF) ,40% and persistent AF unresponsive to DCC, in whom a tachycardia-mediated process is thought to be predominant. ..................................................................................................................................................................................... Methods Between January 2008 and September 2011, among 129 CHF patients with persistent AF referred to our institution, and results 34 (63.8 + 9-year old, 24 men) presented AF refractory to DCC with an estimated high likelihood of tachycardiamediated LV dysfunction according to a specific set of criteria. These 34 patients underwent stepwise AF ablation and were closely followed up. After a mean 1.9 AF ablation procedures per patient and 17.6 + 7 months after the last procedure, all patients were in SR. The New York Heart Association class improved from 2.8 + 0.3 to 1 + 0.2 (P , 0.001) and the LVEF increased from 30.4 + 6 to 54.6 + 6% (P , 0.0001) after 3–6 months of SR, with a persistent benefit as long as the SR was maintained. ..................................................................................................................................................................................... Conclusion Atrial fibrillation catheter ablation in selected CHF patients with persistent AF refractory to DCC and without any other evidence for secondary LV dysfunction leads to a substantial LVEF improvement in the majority of them. However, redo procedures are frequent in order to achieve mid-term SR maintenance. ----------------------------------------------------------------------------------------------------------------------------------------------------------Keywords Congestive heart failure † Persistent atrial fibrillation † Catheter ablation Introduction Atrial fibrillation (AF) catheter ablation can lead to left ventricular ejection fraction (LVEF) improvement in congestive heart failure (CHF) patients. However, the literature suggests that such LVEF improvement remains inconstant and variable according to the CHF aetiology.1 – 7 Because AF catheter ablation is an invasive procedure with potential complications,8,9 it should ideally be performed in CHF patients with the highest likelihood of LVEF improvement after reversion to sinus rhythm (SR). In clinical daily practice, participation of tachycardia-mediated process to ventricular systolic dysfunction may be easily assessed by the degree of LVEF improvement after reversion to SR by direct current cardioversion (DCC). However, if DCC fails to restore stable SR, AF participation to the left ventricular (LV) systolic dysfunction remains hypothetic and patients’ management becomes challenging with potential need for invasive therapies [e.g. biventricular pacing, implantable * Corresponding author. Tel: +33 466266375; fax: +33 466269728, Email: [email protected] Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2013. For permissions please email: [email protected]. AF ablation and heart failure What’s new? † We present novel and exploratory decisional work-up aiming to identify congestive heart failure (CHF) patients with persistent atrial fibrillation (AF) unresponsive to direct current cardioversion most likely to respond to catheter ablation. † Our results confirm the idea that appropriate selection of candidates for AF catheter ablation is of major importance for obtaining good results (in terms of left ventricular (LV) ejection fraction value increase) in patients presenting CHF and LV systolic dysfunction. cardioverter defibrillator insertion, and atrioventricular (AV) nodal ablation]. In the present paper, we report our experience on catheter ablation in a group of CHF patients, presenting with severely depressed LVEF (,40%) and persistent AF, unresponsive to DCC, and for whom we hypothesized that the LV dysfunction was predominantly related to the persistent AF process. Methods Selection of patients Among the CHF patients with depressed LVEF (,40%) and persistent AF referred to our Institution between January 2008 and September 2011 (n ¼ 129), we included in the present analysis CHF patients with persistent AF refractory to DCC, for whom there was no evidence for another cause of secondary LV dysfunction such as ischaemic heart disease, cardiac valve disease, severe systemic hypertension, and regular alcohol intake. Atrial fibrillation refractory to DCC was defined as persistent or longstanding persistent AF for which DCC was unable to restore SR for 30 s or longer.9 The management of CHF patients with persistent AF has been standardized and a protocol was established in collaboration with all physicians of our Institution since 2007 following particularly striking preliminary experience with two CHF patients referred to us for biventricular device insertion/AV nodal ablation and consideration for heart transplant, respectively. A step-by-step work-up was then established in January 2008 and is summarized in Figure 1. Overall, every patient with persistent AF and no evidence for other cause of LV systolic dysfunction (and in the absence of contra- or nonindication for a rhythm control strategy) underwent at least one attempt of AF reduction by DCC (1– 3 antero-posterior either monophasic 360 J or biphasic 200 J shocks) after at least 1-month of amiodarone treatment (if not contra-indicated). If SR was restored for at least 1 month, management of the patient depended on the evolution of the LVEF value after that month of stable SR (which corresponds to a minimal period of stable SR required for significant LVEF improvement (≥15%) in patients with a possible tachycardia-mediated cardiomyopathy).10 If DCC failed to restore stable SR for at least 1 month, patients were systematically offered AF catheter ablation in order to assess the participation of the persistent AF process to the LV systolic dysfunction by restoring SR for at least 1 month. All enrolled patients underwent comprehensive explorations, including physical examination, 12-lead electrocardiogram (ECG), 1575 blood tests, trans-thoracic echocardiography, continuous 48 h ECG monitoring and coronary angiogram. All patients were informed about the potential benefits and risks of the AF catheter ablation procedure, which, was performed after obtaining written consent from the patient and approval from the ethics committee of our Institution. Atrial fibrillation radiofrequency catheter ablation Prior to ablation, patients were put for at least two consecutive months on efficient vitamin K antagonists [international normalized ratio (INR 2 – 3)], with a shift, 1 week before the intervention, to low-weight-molecular heparin, or standard heparin in case of renal function impairment. Patients underwent transesophageal echocardiography 24 h before the ablation to rule out left atrial (LA) thrombi. All AF ablation procedures were conducted under general anaesthesia. A 6F deflectable quadripolar catheter (XtremTM , ELA Medical, Le-Plessis-Robinson) was positioned within the coronary sinus (CS). Two long sheaths (PrefaceTM , Biosense Webster, Inc.) were advanced into the LA after two trans-septal punctures under fluoroscopy guidance. Intravenous heparin was given with a target activated clotting time of 350 – 400 s. A 3.5 mm externally irrigated-tip ablation catheter (Navi-StarTM , Thermo-CoolTM ) was placed in the LA through one of the long sheaths, and permitted to build a LA shell using a three dimensional electro-anatomical system (CartoTM ). Subsequently, the LA shell was merged with patient’s LA computed tomography acquired prior to the ablation procedure. On the beginning of the procedure, the AF cycle length was measured at both atrial appendages.11 The first ablation step consisted in a two by two pulmonary veins (PVs) isolation at their antral level by creating a circular continuous lesion guided by a 10-pole circular catheter (LassoTM ).12 If patients remained in AF, the second ablation step consisted in CS isolation13,14 and cavo-tricuspid isthmus ablation.15 The third step implied LA linear lesions (roof, mitral isthmus, posterior line in order to isolate the posterior LA wall) deployment.16 – 18 If patients were still in AF once these three ablative steps completed, the AF cycle length was measured once again at both atrial appendages19 and the atrial chamber with the shortest cycle length was considered for complex fractioned atrial electrograms (CFAEs) ablation. The endpoint of the AF ablation procedure was SR restoration by catheter ablation either directly from AF or through atrial tachycardia (AT). In case of persistence of AF after the four ablation steps, DCC was performed. Whenever AF converted into AT, the latter was mapped and ablated. If AT could not be terminated by catheter ablation, SR was restored by DCC. When SR was obtained either by catheter ablation or by DCC, bidirectional block was assessed at the PV antra (entrance and exit block),20 the cavo-tricuspid isthmus,15,21 the LA roof, and the mitral isthmus linear lesions (whenever performed).16,17 Finally, LA wall isolation (box) was also assessed (whenever performed).18 Ablation pre-settings were 30 W/488C/20 cc/min except for the posterior wall of the LA (25 W), the CS (20 – 25 W), the mitral isthmus (35 W), and the cavo-tricuspid isthmus (40 W). The day after the procedure, all patients underwent trans-thoracic echocardiography. All patients were discharged from the institution within 7 days of the procedure. Follow-up and rhythm control management Patients were followed at the outpatient clinic of our institution at 1, 3, 6, 9, and 12 months after the ablation, and every 6 months thereafter. 1576 A. Bortone et al. Figure 1 Work-up for the management of congestive heart failure patients with persistent atrial fibrillation. NYHA, New York Heart Association; CABG, coronary artery bypass grafting; ARVD, arrhythmogenic right ventricular dysplasia; ICD, implantable cardioverter defibrillator. Standard clinical examination, 12-lead ECG, trans-thoracic echocardiography, and continuous 48 h Holter monitoring were routinely performed at each visit. Amiodarone was stopped after 3 months of stable SR while beta-blockers, angiotensin-converting enzyme inhibitors, spironolactone, and vitamin K antagonists were maintained indefinitely in all patients with a target INR of 2 – 3. Atrial tachycardia/AF recurrence was defined as any documented AT/AF episode lasting .30 s, whether symptomatic or not. In case 1577 AF ablation and heart failure of early arrhythmia recurrence (,3 months after AF catheter ablation) DCC was performed, whereas in case of AT/AF recurrence (≥3 months), a redo AT or AF catheter ablation procedure was offered to patients.9 During follow-up, LVEF was carefully evaluated and was considered as normalized when it reached 55%. Statistical analysis Descriptive variables are presented as means + SD (min – max) or percentages. Non-parametric test were used, sample means were compared with Wilcoxon test. The exact Fisher’s test was used to compare the frequencies. All tests were two-tailed, and P values of less than 0.05 were considered to indicate statistical significance. Index atrial fibrillation catheter ablation procedure and subsequent rhythm management Results Studied population Among the CHF patients with persistent AF and without any other evidence for secondary LV dysfunction (n ¼ 63), DCC was not successful in 34 patients (54%) for whom SR could be achieved for a few minutes or hours only. The characteristics of these 34 patients who represent the study population are described in Table 1. Their mean age was 63.8 + 9 year old (range: 42–77 years); there were 24 men and 10 women, 11 patients presented with longstanding persistent AF while the remaining 23 patients had persistent AF. DCC attempts were performed under amiodarone treatment in all patients. However, owing to the absence of SR restoration, amiodarone was stopped in 20 patients by their Table 1 Baseline characteristics of the study subjects Patients characteristics ................................................................................ Age (years) Gender (M/F) 63.8 + 9.6 24/10 Ventricular rate while in AF (b.p.m.) 85.4 + 9.4 NYHA functional class LVEF (%) 2.8 + 0.3 30.4 + 6.7 LA volume (mL) 172.4 + 40.6 LV volume (mL) Continuous AF duration before ablation (months) 195.2 + 36.8 11 + 12.7 Hypertension (%) cardiologist in order to prevent any side effect linked to this medication. Therefore, at the time of the index ablation procedure, only 14 patients were on amiodarone treatment. No other antiarrhythmic drug was used. All the study subjects were treated for 3–6 months with maximal tolerated oral pharmacological therapy prior to the first ablation procedure. Mean daily ventricular rate on the Holter-ECG before AF catheter ablation was 85.4 + 9 b.p.m. and the mean baseline LVEF was 30.4 + 6%. The average continuous AF duration before catheter ablation was 11 + 12 months. 14 (41.7) Diabetes mellitus (%) Previous TIA/stroke (%) 5 (14.7) 2 (5.8) Vascular disease (%) 0 (0) Obesity (%) Sleep apnoea (%) 4 (11.7) 1 (2.9) Beta-blockers (%) 34 (100) ACE inhibitors (%) Spironolactone (%) 34 (100) 32 (94.1) Impaired renal function (%) 2 (5.8) Significant cardiac valve disease Significant coronary artery disease 0 (0) 0 (0) NYHA, New York Heart Association; AF, atrial fibrillation; TIA, transient ischaemic attack; LA, left atrium; LVEF, left ventricular ejection fraction; ACE, angiotensin-converting enzyme. During the index AF ablation procedure, SR was restored by catheter ablation in 15 patients (44%)—in 6 patients directly from AF and in 9 patients after AF conversion into AT. In the remaining 19 patients (56%), AF was converted to AT in 10 patients, while in the other 9 patients AF persisted. Direct current cardioversion restored SR in all these 19 patients. The mean total procedural duration and radiation exposure time were 236.7 + 22 and 34.7 + 4 min, respectively. The mean initial AF cycle length was 160.5 + 21 ms. Pulmonary vein isolation at the antral level, CS isolation + cavo-tricuspid isthmus ablation, roof + mitral isthmus + LA posterior (box) lines deployment, and CFAEs ablation increased the AF cycle length by 8.1 + 1.3, 6.4 + 2.3, 11.5 + 1.4, and 7.5 + 1.2 ms, respectively. Pulmonary veins were electrically isolated in all patients. The cavo-tricuspid isthmus ablation was performed in the entire cohort with bidirectional block achievement in all patients.15,21 Coronary sinus isolation was also performed in the entire cohort most often following both an endocardial and epicardial approach.13,14 Left atrial roof line was performed in 29 patients and bidirectional block was achieved in all cases according to standard criteria.16 The mitral isthmus line was created in 28 patients but bidirectional block17 could be achieved in 19 cases (67.8%) only. Finally, LA box creation by deploying a postero-inferior line effectively isolated the LA wall18 in 21/24 cases (87%). Complex fractionated atrial electrograms were targeted in 23 patients (at the LA in 21 patients and at the right atrium in 2 patients). During the 26.1 + 9 months follow-up period, 12 (35%) did not present AF recurrence: 5 patients had none AT/AF recurrence, whereas 7 patients presented early AT episodes and were then treated by successful DCC without subsequent AT/AF recurrence. Fourteen patients (41%) underwent one redo ablation procedure due to persistent AT (n ¼ 10) or paroxysmal AF episodes (n ¼ 4). Among the 10 ATs, 7 were related to LA focal reentries while 3 were related to LA macro-reentrant circuits.22 Of note, in these 10 patients at least one pair of ipsilateral PVs was found as reconnected. Similarly, in the 4 patients with paroxysmal AF episodes, at least 1 pair of ipsilateral PVs (most often left sided PVs) was also electrically reconnected. Seven patients (21%) underwent two-redo AT ablation procedures and 1 patient (3%) underwent three redo ablation procedures due to AT recurrence. Among these 17 ATs, 13 were related to a LA focal reentry and the remaining 4 corresponded 1578 to LA mitral isthmus-dependent ATs. Of note, at least one pair of ipsilateral PVs was reconnected (most often left-sided PVs) in all patients while performing the first redo procedure. Conversely, while performing the second and third ablation procedures, only two patients presented recovery of the LA –PV conduction. Overall, after 1.9 catheter ablation procedures per patient and a mean follow-up of 17.6 + 7 months (range: 5–38 months) following the last catheter ablation procedure, the entire cohort was in stable SR without anti-arrhytmic drugs (except beta-blockers). However, amiodarone was transiently administered to those patients presenting with AT/AF recurrence while waiting for their redo procedures. Of note, one patient developed cardiac tamponade 6 h after his third ablation procedure and was surgically managed with uneventful subsequent evolution. No other general or local procedure-related complication was observed and we noted no embolic event during the entire follow-up period. New York Heart Association functional status and left ventricular ejection fraction progression The population New York Heart Association functional class improved from 2.8 + 0.3 to 1 + 0.2 (P , 0.001). The mean LVEF increased from 30.4 + 6 (range: 19–40) to 54.6 + 6% (range: 42 –66) (P , 0.0001) (Figure 2), while the LV diastolic volume decreased from 195.2 + 36 to 162.2 + 32 mL (P , 0.0001), both after 3 –6 months of stable SR. Figure 2 LVEF evolution after SR restoration. A. Bortone et al. In 5 patients (15%) the LVEF improved significantly (from 23.8 + 4 to 45.2 + 5%, P , 0.01) but the value remained under 50% while 14 patients (41%) had LVEF normalization (.55%). Finally, in 15 patients (44%) the LVEF reached values between 50 and 55%. Paroxysmal AF recurrences occurred in four patients with a maximal duration of AF episodes estimated to 4.5 h. Although they did not lead to a LVEF decline, they were symptomatic and motivated the redo procedures. Conversely, persistent AT recurrences were poorly tolerated and led in the majority of cases (81%) to a drastic decline of the LVEF, to values similar to those observed prior to the index catheter procedure. Of note, after SR restoration, the LVEF improvement followed the same profile than after the index procedure. The initial mean LVEF of the 29 patients who had successful SR restoration for at least 1 month (see Figure 1) was 30.3 + 7.3%. The LVEF increased after 1 month and after 3–6 months of stable SR to 46.5 + 8.3 and 51.6 + 6%, respectively. Among these 29 patients, 8 patients (27%) had LVEF improvement but to ,50% while 7 patients (24%) had LVEF normalization (.55%). The remaining 14 patients (49%) had a final LVEF value between 50 and 55%. Discussion Main findings The salient findings of the present work are the following: (i) CHF patients with persistent AF refractory to DCC and without any AF ablation and heart failure other evidence for secondary LV dysfunction, may be particularly good responders to AF catheter ablation and relatively easily selected and (ii) although AF catheter ablation appears effective and safe in this setting, AF/AT recurrences are commonly observed, most often requiring supplemental ablative procedures. Atrial fibrillation catheter ablation in congestive heart failure patients Although AF catheter ablation may lead to reversal of the LV systolic dysfunction in the CHF framework, literature suggests that the LVEF improvement after SR restoration is not constantly observed in all CHF patients and seems to mainly vary according to CHF aetiology. In this context, publications suggest that dilated cardiomyopathy is the CHF subgroup with the highest propensity for presenting LVEF improvement after reversion to SR while CHF patients presenting valvular, ischaemic, alcoholic, and hypertensive cardiomyopathies are less prone to LVEF improvement after SR restoration.1 – 7 Because AF catheter ablation carries substantial risks for patients (even if the complication rate remains low)8,9 and may be perceived as more challenging and perhaps more dangerous in the CHF setting than in other populations, identification of possible CHF responders in terms of LVEF improvement prior to AF catheter ablation is of particular concern. Ideally, AF catheter ablation should be carried out in CHF patients with an LV systolic dysfunction totally or at least substantially related to the AF process and therefore, with a high probability of LVEF improvement after reversion to SR. Selection of candidates for AF catheter ablation in the setting of CHF therefore, appears as a primordial process in order to ensure the best possible LVEF outcome after reversion to SR. From a practical standpoint, an easy manner to unmask the implication of the persistent AF process into the LV systolic dysfunction and to justify therefore, the need for performing AF catheter ablation, is to restore stable SR by DCC. If SR (at least 1 month of stable SR)10 leads to LVEF improvement, the AF catheter ablation appears clearly justified (either directly or after AF recurrence). At the opposite, if stable SR restoration does not lead to LVEF improvement, AF catheter ablation can be considered unnecessary because the persistent AF process in this case is not an important cause but only an epiphenomenon of an underlying cardiomyopathy. However, in patients with optimal oral medications and with a well-controlled ventricular rate, if DCC fails to stably restore SR, the participation of the persistent AF process to the LV systolic dysfunction is impossible to assess thus rendering patients’ management challenging with the need for invasive therapies (e.g. biventricular pacing, implantable cardioverter defibrillator insertion, and AV nodal ablation). In this specific setting of CHF patients with persistent AF unresponsive to DCC, our findings suggest that AF catheter ablation in patients without any other evidence for secondary LV dysfunction and without prior history of depressed LV systolic function while in SR, leads to a substantial LVEF improvement in most cases. Consequently, in our series, the persistent AF process appears as totally or at least substantially implicated in the LVEF depression. Accordingly, 14 patients (41%) had LVEF normalization (.55%) and can be considered as having presented a pure tachycardia-related 1579 cardiomyopathy while it is likely that the remaining 20 patients (59%) in whom the LVEF improvement was substantial but did not reach 55% (range: 42 –54%) have a dilated cardiomyopathy from an unknown cause severely worsened by the persistent AF process. Similarly, the LVEF improvement profile of the 29 patients (selected following the same step-by-step work-up) in whom DCC effectively restored stable SR for at least 1 month is equivalent to that of the 34 study subjects. Among these 29 effectively cardioverted patients, only 7 (24%) had LVEF normalization while the remaining 22 patients (76%) had an improvement in their LVEF that failed to reach 55%. We recognize that the studied population could have been managed differently as stated above with biventricular device insertion (with most probably implantable cardioverter defibrillator) followed by AV nodal ablation or considered for heart transplant owing to the severity of its clinical status and its potential poor prognosis. However, since SR restoration permitted a drastic LVEF improvement, these therapeutics strategies became irrelevant. The optimization of ventricular rate control could have been another therapeutic alternative. However, as the mean ventricular rate of the study subjects was relatively low (85.4 + 9 b.p.m.) while their LVEF was severely depressed, we felt that a more rigorous ventricular rate control would not have led to a significant LVEF improvement. Our results emphasize that beyond the ventricular rate, irregularity of contraction and loss of atrial systole both participated to LV dysfunction in the studied population23 – 27 Finally, it should be highlighted that AF catheter ablation made the mid-term management of the studied population easier, by rendering them subsequently responsive to DCC whenever AF/AT recurred. Mid- and long-term sinus restoration rate in congestive heart failure patients after catheter ablation Recent publications show that mid- and long-term SR achievement by catheter ablation in patients with persistent and long-standing persistent AF is challenging and commonly needs more than one catheter ablation procedure.9,28 – 30 Similar findings were obtained in specific series focusing on persistent AF ablation in CHF setting.1 – 6 In CHF patients with LV systolic dysfunction the challenge may be more pronounced if reversion to SR leads to a substantial LVEF improvement. Indeed, in this specific CHF population totally or partially afflicted by a tachycardia-mediated cardiomyopathy process, AF/AT recurrences may lead to a new depression of the LVEF value and even be linked, although rarely, with sudden cardiac death.31 In the present article, the rate of SR achievement after a single AF catheter ablation procedure was poor (around 35%), which is consistent with available literature. Therefore, several supplemental ablation procedures were necessary to ensure mid-term (17.6 + 7 months) stable SR to the entire population studied. However, we are aware that AF/AT recurrences might be observed during extended follow-up periods and therefore, that these patients must be closely and continuously monitored. 1580 Limitations Even if, at the best of our knowledge, this is the first published approach identifying CHF patients with persistent AF unresponsive to DCC most likely to respond to catheter ablation, we agree on some limitations. First, this is a single-centre study without a control group and with a relative limited number of patients. However, our results are highly suggestive of the beneficial role of AF catheter ablation in this specific subset of CHF patients. Second, we recognize that LVEF calculation by trans-thoracic echocardiogram in patients with AF may overestimate the LV systolic depression, particularly when the ventricular rate is uncontrolled. However, as reported in the Results section, our population demonstrated a relatively low ventricular rate. Conclusion Atrial fibrillation catheter ablation in selected CHF patients with persistent AF refractory to DCC and without any other evidence for secondary LV dysfunction appears as a strategy of particular interest given the proportion of patients who demonstrated substantial LVEF improvement after reversion to SR. It is important, however, to emphasize that the AF/AT recurrence rate is high and that the redo procedures are almost constant in order to achieve mid-term stable SR maintenance. Conflict of interest: none declared. References 1. Hsu LF, Jaı̈s P, Sanders P, Garrigue S, Hocini M, Sacher F et al. Catheter ablation for atrial fibrillation in congestive heart failure. N Engl J Med 2004;351:2373 – 83. 2. Chen MS, Marrouche NF, Khaykin Y, Gillinov AM, Wazni O, Martin DO et al. Pulmonary vein isolation for the treatment of atrial fibrillation in patients with impaired systolic function. J Am Coll Cardiol 2004;43:1004 – 9. 3. Gentlesk PJ, Sauer WH, Gerstenfeld EP, Lin D, Dixit S, Zado E et al. Reversal of left ventricular dysfunction following ablation for atrial fibrillation. J Cardiovasc Electrophysiol 2007;18:9 –14. 4. Khan MN, Jaı̈s P, Cummings J, Di Biase L, Sanders P, Martin DO et al. Pulmonaryvein isolation for atrial fibrillation in patients with heart failure. N Engl J Med 2008; 359:1778 –95. 5. Bortone A, Boveda S, Pasquié JL, Pujadas-Berthault P, Marijon E, Appetiti A et al. Sinus rhythm restoration by catheter ablation in patients with long-lasting atrial fibrillation and congestive heart failure: impact of the left ventricular ejection fraction improvement on the implantable cardioverter defibrillator insertion indication. Europace 2009;11:1018 – 23. 6. MacDonald MR, Connelly DT, Hawkins NM, Steedman T, Payne J, Shaw M et al. Radiofrequency ablation for persistent atrial fibrillation in patients with advanced heart failure and severe left ventricular systolic dysfunction: a randomised controlled trial. Heart 2011;97:740 –7. 7. Dagres N, Varounis C, Gaspar T, Piorkowski C, Eitel C, Iliodromitis EK et al. Catheter ablation for atrial fibrillation in patients with left ventricular systolic dysfunction. A systematic review and meta-analysis. J Card Fail 2011;17:964 –70. 8. Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J et al. Updated worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circ Arrhythm Electrophysiol 2010;3:32 –8. 9. Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SA et al. 2012 HRS/EHRA/ESC Expert Consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Europace 2012;14:528 –606. A. Bortone et al. 10. Van Gelder IC, Crijns HJ, Blanksma PK, Landsman ML, Posma JL, Van Den Berg MP et al. Time course of hemodynamic changes and improvement of exercise tolerance after cardioversion of chronic atrial fibrillation unassociated with cardiac valve disease. Am J Cardiol 1993;72:560 –6. 11. O’Neill MD, Jaı̈s P, Takahashi Y, Jönsson A, Sacher F, Hocini M et al. The stepwise ablation approach for chronic atrial fibrillation-evidence for a cumulative effect. J Interv Card Electrophysiol 2006;16:153 –67. 12. Arentz T, Weber R, Bürkle G, Herrera C, Blum T, Stockinger J et al. Small or large isolation areas around the pulmonary veins for the treatment of atrial fibrillation? Results from a prospective randomized study. Circulation 2007;115:3057 –63. 13. Haı̈ssaguerre M, Hocini M, Takahashi Y, O’Neill MD, Pernat A, Sanders P et al. Impact of catheter ablation of the coronary sinus on paroxysmal or persistent atrial fibrillation. J Cardiovasc Electrophysiol 2007;18:378–86. 14. Bortone A, Boveda S, Combes N, Albenque JP. Clockwise loop of the ablation catheter in the left atrium: an easy and safe approach facilitating substrate modulation in the setting of atrial fibrillation ablation. J Cadiovasc Electrophysiol 2008;19: 338 –41. 15. Shah DC, Takahashi A, Jaı̈s P, Hocini M, Clémenty J, Haı̈ssaguerre M. Local electrogram-based criteria of cavotricuspid isthmus block. J Cardiovasc Electrophysiol 1999;10:662 –9. 16. Hocini M, Jaı̈s P, Sanders P, Takahashi Y, Rotter M, Rostock T et al. Techniques, evaluation, and consequences of linear block at the left atrial roof in paroxysmal atrial fibrillation: a prospective randomized study. Circulation 2005;112:3688 –96. 17. Jaı̈s P, Hocini M, Hsu LF, Sanders P, Scavee C, Weerasooriya R et al. Technique and results of linear ablation at the mitral isthmus. Circulation 2004;110: 2996 –3002. 18. Sanders P, Hocini M, Jaı̈s P, Sacher F, Hsu LF, Takahashi Y et al. Complete isolation of the pulmonary veins and posterior left atrium in chronic atrial fibrillation. Longterm clinical outcome. Eur Heart J 2007;28:1862 –71. 19. Hocini M, Nault I, Wright M, Veenhuyzen G, Narayan SM, Jaı̈s P et al. Disparate evolution of right and left atrial rate during ablation of long-lasting persistent atrial fibrillation. J Am Coll Cardiol 2010;55:1007 –16. 20. Gerstenfeld EP, Dixit S, Callans D, Rho R, Rajawat Y, Zado E et al. Utility of exit block for identifying electrical isolation of the pulmonary veins. J Cardiovasc Electrophysiol 2002;13:971 –9. 21. Shah D, Haı̈ssaguerre M, Takahashi A, Jaı̈s P, Hocini M, Clémenty J. Differential pacing for distinguishing block from persistent conduction through an ablation line. Circulation 2000;102:1517 –22. 22. Jaı̈s P, Matsuo S, Knecht S, Weerasooriya R, Hocini M, Sacher F et al. A deductive mapping strategy for atrial tachycardia following atrial fibrillation ablation: importance of localized reentry. J Cardiovasc Electrophysiol 2009;20:480 –91. 23. Shinbane JS, Wood MA, Jensen DN, Ellenbogen KA, Fitzpatrick AP, Scheinman MM. Tachycardia-induced cardiomyopathy: a review of animal models and clinical studies. J Am Coll Cardiol 1997;29:709 – 15. 24. Clark DM, Plumb VJ, Epstein AE, Kay GN. Hemodynamic effects of an irregular sequence of ventricular cycle lengths during atrial fibrillation. J Am Coll Cardiol 1997;30:1039 –45. 25. Stevenson WG, Stevenson LW. Atrial fibrillation in heart failure. N Engl J Med 1999;341:910 –1. 26. Pozzoli M, Cioffi G, Traversi E, Pinna GD, Cobelli F, Tavazzi L. Predictors of primary atrial fibrillation and concomitant clinical and hemodynamic changes in patients with chronic heart failure: a prospective study in 344 patients with baseline sinus rhythm. J Am Coll Cardiol 1998;32:197–204. 27. Asirvatham SJ. Tachycardia-induced cardiomyopathy, without the tachycardia: yet another reason to ablate atrial fibrillation? J Cardiovasc Electrophysiol 2007;18: 15 –7. 28. Arya A, Hindricks G, Sommer P, Huo Y, Bollmann A, Gaspar T et al. Long-term results and the predictors of outcome of catheter ablation of atrial fibrillation using steerable sheath catheter navigation after single procedure in 674 patients. Europace 2010;12:173–80. 29. Tzou WS, Marchlinski FE, Zado ES, Lin D, Dixit S, Callans DJ et al. Long-term outcome after successful catheter ablation of atrial fibrillation. Circ Arrhythm Electrophysiol 2010;3:237 –42. 30. Weerasooriya R, Khairy P, Litalien J, Macle L, Hocini M, Sacher F et al. Catheter ablation for atrial fibrillation: are results maintained at 5 years of follow-up? J Am Coll Cardiol 2011;57:160 –6. 31. Nerheim P, Birger-Botkin S, Piracha L, Olshansky B. Heart failure and sudden death in patients with tachycardia-induced cardiomyopathy and recurrent tachycardia. Circulation 2004;110:247 –52.