Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Myocardial infarction wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac surgery wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Heart arrhythmia wikipedia , lookup
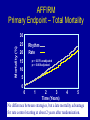
Atrial Arrhythmia Management in Advanced Heart Failure Patients Eric E. Johnson, MD, FACC, FHRS The Stern Cardiovascular Foundation Baptist Memorial Hospital-Memphis Disclosures Medtronic advisory board, speaking engagements, clinical research support. Speaker for BMS, Pfizer. Cheney Recovering at Home After Being Treated for Irregular Heartbeat MONDAY, NOVEMBER 26, 2007 Question 1: How would you manage AF in this patient? 1.) Rate control and anticoagulate 2.) Anticoagulate and begin amiodarone 3.) Cardiovert 4.) No change in therapy 5.) Go on hunting trip and not worry Dick Cheney Cheney has a long history of cardiovascular disease He had his first of five heart attacks in 1978, at age 37. Subsequent attacks resulted in moderate left ventricular dysfunction. He underwent four-vessel coronary artery bypass grafting in 1988, coronary artery stenting in November 2000, urgent coronary balloon angioplasty in March 2001 He underwent implantation of an implantable cardioverter-defibrillator in June, 2001. CBS News reported that during the morning of November 26, 2007, Cheney was diagnosed with atrial fibrillation and underwent treatment that afternoon. In July 2010, Cheney was outfitted with a left-ventricular assist device (LVAD) at Inova Fairfax Heart and Vascular Institute to compensate for worsening congestive heart failure. On March 24, 2012, Cheney underwent a seven-hour heart transplant procedure at Inova Fairfax Hospital in Falls Church, Virginia, at the age of 71. From Wikipedia Introduction • Atrial fibrillation begets atrial fibrillation. AF begets heart failure. HF begets AF. • RATE CONTROL & ANTICOAGULATION (AFFIRM) What about CHF? (AF-CHF) • Underlying substrate - optimize meds for HTN, HF • Device therapy: pacing - selective site, multiple site, minimize ventricular pacing, atrial therapies, CRT • Catheter Ablation - AVN RF & AF ablation (PVI) • AF in LVAD AND HT patients • Review of guidelines • AF is associated with increased risk of stroke, HF, and all-cause mortality • Mortality rate with AF is double that of patients in SR and linked to severity of underlying disease – SOLVD mortality 34% AF vs 23% SR • Difference in deaths due to HF rather than thromboembolism – COMET • No difference in all-cause mortality with AF at entry • Mortality increased if AF developed during follow-up • HF promotes AF, AF aggravates HF, and individuals who develop alternate condition share poor prognosis. From: Rhythm Control in Heart Failure Patients With Atrial Fibrillation: Contemporary Challenges Including the Role of Ablation J Am Coll Cardiol. 2014;64(7):710-721. doi:10.1016/j.jacc.2014.06.1169 Figure Legend: The Physiological Relationship Between Atrial Fibrillation and Heart Failure Action potential duration heterogeneity includes spatial and temporal nonuniformities (36). This mechanistic hypothesis has fallen out of favor with recent evidence (33). Date of download: 2/1/2015 Copyright © The American College of Cardiology. All rights reserved. QuickTime™ and a TIFF (Uncompressed) decompressor are needed to see this picture. AFFIRM Primary Endpoint – Total Mortality Mortality (%) 30 25 Rhythm Rate 20 15 p = 0.078 unadjusted p = 0.068 adjusted 10 5 0 3 2 5 4 Time (Years) No difference between strategies, but a late mortality advantage for rate control starting at about 2 years after randomization. 0 1 Implications of AFFIRM • Rate control is appropriate primary therapy • Anticoagulation for all with one or more risk factors for stroke • What therapies are under-represented? – Non-pharmacologic therapies • Who is under-represented in AFFIRM? – – – – Young patients Paroxysmal atrial fibrillation Disabling symptoms of AF CHF Rhythm Control Drugs in HF • What drug(s) are indicated for HF patients? 1. 2. 3. 4. 5. 6. Propafenone Amiodarone Sotalol Dofetilide 1&3 2&4 AF-CHF Trial AF-CHF Study Design Strategy Algorithm Baseline Characteristics Medical Therapy at 12 Months Primary Endpoint: Cardiovascular Death Secondary Endpoints AF-CHF Conclusions AF Ablation: Pulmonary Vein Isolation (PVI) QuickTime™ and a MS-MPEG4 v2 decompressor are needed to see this picture. From: Rhythm Control in Heart Failure Patients With Atrial Fibrillation: Contemporary Challenges Including the Role of Ablation J Am Coll Cardiol. 2014;64(7):710-721. doi:10.1016/j.jacc.2014.06.1169 Figure Legend: Approaches to Catheter Ablation in AF and HF CFAE = complex fractionated atrial electrogram; PV = pulmonary vein; PVI = pulmonary vein isolation; other abbreviations as in Figure 1. Date of download: 2/1/2015 Copyright © The American College of Cardiology. All rights reserved. AV Node Ablation • Does not eliminate AF • Effective in controlling ventricular rate • Improves: – QOL – Exercise tolerance – Left ventricular function • No deleterious effect on survival From: Rhythm Control in Heart Failure Patients With Atrial Fibrillation: Contemporary Challenges Including the Role of Ablation J Am Coll Cardiol. 2014;64(7):710-721. doi:10.1016/j.jacc.2014.06.1169 Table Title: Key Questions Specific to Catheter Ablation of AF in Patients With HF Date of download: 2/1/2015 Copyright © The American College of Cardiology. All rights reserved. Clinical Impact of AF in Patients with LVAD • AF develops in up to 50% of patients with LVADs • PAF is not associated with worse outcomes in patients with HMII LVAD • Persistent AF may be associated with increased mortality and HF hospitalization • Patients with AF may have thromboembolic events at higher INR levels JACC. 2014;64(18):1883-1890 AF post-heart transplantation QuickTime™ and a decompressor are needed to see this picture. J Am Heart Assoc. 2012 Apr; 1(2): e001461. Published online 2012 Apr 24. 2014 AHA/ACC/HRS Guideline for the Management of Patients with AF and CHF • Class I 1. In the absence of pre-excitation, intravenous betablocker administration is recommended to slow the ventricular response to AF in the acute setting, with caution needed in patients with overt congestion, hypotension, or HF with reduced EF 2. In the absence of pre-excitation, intravenous digoxin or amiodarone is recommended to control heart rate acutely in patients with HF 3. Digoxin is effective to control resting heart rate in patients with HF with reduced EF JACC. 2014;64(21):2246-2280 Guideline: AF and CHF • Class IIa 1. A combination of digoxin and a beta blocker is reasonable to control resting and exercise heart rate in patients with AF 2. It is reasonable to perform AV node ablation with ventricular pacing to control heart rate when pharmacological therapy is insufficient or not tolerated 3. Intravenous amiodarone can be useful to control heart rate in patients with AF when other measures are unsuccessful or contraindicated JACC. 2014;64(21):2246-2280 Guideline: AF and CHF • Class IIa 4. For patients with AF and rapid ventricular response causing tachycardia-induced cardiomyopathy, it is reasonable to achieve rate control by either AV nodal blockade or a rhythm-control strategy 5. For patients with chronic HF who remain symptomatic from AF despite a rate-control strategy, it is reasonable to use a rhythm-control srategy JACC. 2014;64(21):2246-2280 Guideline: AF and CHF • Class IIb 1. Oral amiodarone may be considered when resting and exercise heart rate cannot be adequately controlled using a beta blocker or digoxin, alone or in combination 2. AV node ablation may be considered when the rate cannot be controlled and tachycardia-mediated cardiomyopathy is suspected JACC. 2014;64(21):2246-2280 • Guideline: AF and CHF Class III:Harm 1. AV node ablation should not be performed without a pharmacological trial to achieve ventricular rate control 2. For rate control, intravenous nondihydropyridine calcium channel antagonists, intravenous beta blockers, and dronedarone should not be administered to patients with decompensated HF JACC. 2014;64(21):2246-2280 Increased Mortality Associated with Digoxin in Patients with AF: The TREAT-AF Study • Digoxin is widely used to control the ventricular rate in patients with AF, but evidence supporting safety and efficacy are limited • In patients with recently identified AF, treatment with digoxin was associated with an increased risk of death, independent of kidney function or cardiovascular comorbidities • Consider alternatives to digoxin in managing AF • Prospective studies are needed to confirm findings and explore mechanisms for increased mortality TREAT-AF (The Retrospective Evaluation and Assessment of Therapies in AF) JACC 2014;64(7):660-668 Conclusions 1.) Increasing evidence of interaction AF and HF 2.) Rhythm control and anticoagulation appropriate primary therapy for most patients 3.) Management of underlying substrate and device therapy when appropriate 4.) Evolving role of atrial fibrillation ablation