Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
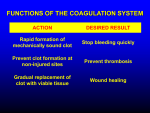
Saad A. Sheta MBBCH, MA, MD Associate Professor, Consultant Anesthesiologist KSU Evaluation of coagulation Basic Hemostatic Mechanisms: I. Primary hemostasis Defects in primary hemostasis von Willebrand’s disease Thrombocytopenia Acquired platelets function disorders II. Coagulation Defects in coagulation • Hemophilia • Acquired factors deficiency liver disease Vit. K deficiency Anticoagulant therapy Heparin Oral Anti- coagulants Massive Blood Transfusion DIC III. Fibrinolysis EVALUATION OF COAGULATION Laboratory testing is almost always needed to establish the cause of bleeding Screening tests (PT, PTT, platelet count) will often allow placement into one of the broad categories Specialized testing is usually necessary to establish a specific diagnosis Platelet Count Bleeding Time (BT) Prothrombin Time (PT) Partial Thromboplastin Time (PTT) Thrombin Time (TT) NORMAL 100,000 - 400,000 cells/mm3 (100 – 400 x 10 9/L) < 100,000 50,000 - 100,000 < 50,000 Thrombocytopenia Mild Thrombocytopenia Severe Thrombocytopenia Provides Assessment Of Platelet Count And Function 5-10% of patients have a prolonged bleeding time Most of the prolonged bleeding times are due to aspirin or drug ingestion Prolonged bleeding time does not predict excess surgical blood loss Not recommended for routine testing in preoperative patients Normal Value 2-8 Minutes COAGULATION FACTORS Fibrinogen II. Prothrombin III. Tissue Thromboplastin IV. Ca++ V. Labile Factor VI. --------Unassigned VII.Stable Factor VIII.Anti hemophilic Factor IX. Christmas Factor X. Stuart Prowers factor XI. Plasma Thromboplastin Antecedent XII.Contact Factor XIII.Fibrin Stabilizing Factor I. Partial thromboplastin time (PTT) Prothrombin time (PT) Phospholipid (provided by platelet which expose platelet F III when they activated Thromboplastin Tissue factor Phospholipids Calcium Normal Value 10-15 Sec Normal Value 25 - 40 Sec. Extrinsic pathway Intrinsic pathway Common pathway Normal Value 9- 13 Sec. Thrombin Thrombin time Fibrin clot By-passes factors II-XII Measures rate of fibrinogen conversion to fibrin Procedure: Add thrombin with patient plasma Measure time to clot Variables: Source and quantity of thrombin CBC and smear Platelet count RBC and platelet morphology Thrombocytopenia TTP, DIC, etc. Coagulation Prothrombin time Partial Thromboplastin time Coagulation factor assays 50:50 mix Fibrinogen assay Thrombin time Extrinsic/common pathways Intrinsic/common pathways Specific factor deficiencies Inhibitors (e.g., antibodies) Decreased fibrinogen Qualitative/quantitative fibrinogen defects Fibrinolysis (DIC) FDPs or D-dimer Platelet Function von Willebrand factor Bleeding time Platelet function analyzer (PFA) Platelet function tests vWD In vivo test (non-specific) Qualitative platelet disorders and vWD Qualitative platelet disorders Sex-linked recessive Factors VIII and IX deficiencies cause bleeding Prolonged PTT; PT normal Autosomal recessive (rare) Factors II, V, VII, X, XI, fibrinogen deficiencies cause bleeding Prolonged PT and/or PTT Factor XIII deficiency is associated with bleeding and impaired wound healing PT/ PTT normal; clot solubility abnormal Factor XII, pre-kallikrein, HMWK deficiencies No bleeding Platelet disorders Coagulation factor disorders Site of bleeding Skin Mucous membranes (epistaxis, gum, vaginal, GI tract) Deep in soft tissues (joints, muscles) Petechiae Yes No Ecchymoses (“bruises”) Small, superficial Large, deep Hemarthrosis / muscle bleeding Extremely rare Common Bleeding after cuts & scratches Yes No Bleeding after surgery or trauma Immediate, usually mild Delayed (1-2 days) often severe Basic Hemostatic Mechanisms I. II. III. Primary hemostasis Coagulation Fibrinolysis Basic Hemostatic Mechanisms I. Primary hemostasis Blood Vessel Spasm Cutting or breaking smaller vessels stimulates the smooth muscles in its walls to contract. May close completely Effects last only a few minutes to 30 minutes Platelets release serotonin which stimulates vasoconstriction and helps maintain vessel spasm 1. Platelets Activation 2. Platelets Adherence von Willebrand factor (intracellular glue ; stick platelets to collagen) 3. Activated platelets release of chemical products ADP, Serotonin, Platelet factor IV(ca++) , B thromboglobin, fibronectin, vWF, fibrinogen, factor V, labile factor,…. 4. PG , called Thromboxane A2 is released Further ADP further aggregation potent vasoconstrictor 5. Aggregated platelets: trap thrombin (coagulation cascade) trap plasminogen platelet plug temporary arrest bleeding 6. larger break may require a blood clot to halt bleeding In case of intact endothelium, Prostacyclin . PG its action opposite to Thromboxane A2 non-thrombogenic Quantitative disorders Inherited disorders (vWF) rare Qualitative disorders Acquired disorders von Willebrand’s disease Inherited / Qualitative ± (Quantitative) Thrombocytopenia Quantitative Acquired platelets function disorders Qualitative von Willebrand factor Synthesis in endothelium and megakaryocytes Forms large multimer Carrier of factor VIII Anchors platelets to sub endothelium Bridge between platelets Inheritance - autosomal dominant Incidence - 1/10,000 Clinical features - mucocutaneous bleeding Classification: Type 1 Type 2 Type 3 Partial quantitative deficiency Qualitative deficiency Total quantitative deficiency Diagnostic tests: Assay vWF antigen vWF activity Multimer analysis 1 von Willebrand type 2 3 Normal Normal Normal Absent Cryoprecipitate Source of fibrinogen, factor VIII and vWF Only plasma fraction that consistently contains VWF multimers DDAVP (deamino-8-arginine vasopressin) plasma vWF levels by stimulating secretion from endothelium Duration of response is variable Not generally used in type 2 disease Dosage 0.3 µg/kg q 12 hr IV Factor VIII concentrate (Intermediate purity) Virally inactivated product Decreased production (bone marrow) Increased sequestration (spleen) Dilutional (massive blood transfusion) Consumption ( burn, pre- eclampsia, DIC, CPB) Immune (heparin) Immune-mediated thrombocytopenia (ITP) Features Acute ITP Chronic ITP Peak age Female : male Antecedent infection Onset of symptoms Platelet count at presentation Duration Spontaneous remission Children (2-6 yrs) 1:1 Common Abrupt <20,000 2-6 weeks Common Adults (20-40 yrs) 3:1 Rare Abrupt-indolent <50,000 Long-term Uncommon History Is the patient bleeding? Are there symptoms of a secondary illness? (neoplasm, infection, autoimmune disease) Is there a history of medications, alcohol use, or recent transfusion? Are there risk factors for HIV infection? Is there a family history of thrombocytopenia? Do the sites of bleeding suggest a platelet defect? Assess the number and function of platelets CBC with peripheral smear Bleeding time or platelet aggregation study Platelet count (per µl) Symptoms Treatment > 50,000 None None 20-50,000 No bleeding Bleeding None Glucocorticoids iv -IG < 20,000 No bleeding Bleeding Glucocorticoids Glucocorticoids iv - IG Hospitalization Uremia Guanidino succuinic a. toxic to platelets Alcohol Cirrhosis Medication s: Aspirin (indomethacin, phenylbutazone, ibuprofen, dextran) inhibit the synthesis of thromboxane A2 (Aspirin for 16-24 hrs) FDP Basic Hemostatic Mechanisms II. Coagulation Most effective hemostatic mechanism Causes formation of a blood clot Clotting factors: Biochemicals (Plasma Protein) that promote or inhibit coagulation Whether or not blood coagulates depends on the balance between 2 groups of factors Normally, anticoagulants prevail = no clots Following injury, Biochemicals that favor coagulation may increase and blood coagulates Fibrinogen II. Prothrombin III. Tissue Thromboplastin ++ IV. Ca V. Labile Factor VI. --------Unassigned VII. Stable Factor VIII. Anti hemophilic Factor IX. Christmas Factor X. Stuart Prowers factor I. XI. Plasma Thromboplastin Antecedent Contact Factor XIII. Fibrin Stabilizing Factor XII. Vit. K dependent Coagulation Factors Factors V & VIII Can not stay in the storage blood Don not become active cleavage (serve as co-factors) Factor VIII (Extra hepatic, MW 400,000 ) VIII C Smaller Hemophilia A VIII R Ag Larger Hemophilia A + vWF Separate genetic control Intrinsic system (surface contact) Extrinsic system (tissue damage) Contact Factor XII XII a Tissue factor Pl..Thromboplastin Antecedent XI XI a Christmas Factor IX IX a VIII VII a Stable Factor VII VIII a Xa Stuart Prowers Factor X V Prothrombin II Fibrinogen Va II a Thrombin Fibrin Prothrombin activator: damaged tissue signals this to be produced Prothrombin (Factor II) : α globulin (liver) It is converted to thrombin by: Prothrombin activator ++ Ca Thrombin catalyzes a reaction that fragments fibrinogen Long fibrin threads stick to exposed surfaces of damaged blood vessels creating a meshwork that entraps blood cells and platelets Resulting mass is a blood clot which may block a vascular break and prevent further blood loss The major event in blood clot formation is the conversion of: soluble fibrinogen (a plasma protein) into insoluble threads of fibrin Serum: clear, yellow fluid that remains after clot Same as plasma, minus the clotting factors Normally: Blood flow prevents massive clot formation within the cardiovascular system by rapidly carrying excess thrombin away, keeping its concentration too low to enhance further clotting Blood coagulation is usually limited to blood standing still or moving slowly. Clotting ceases where clot contacts circulating blood Abnormal Clot Formations Thrombus: a clot abnormally forming in a vessel Embolus: If a clot dislodges or if a fragment of it breaks loose and is carried away by blood flow Continues to move until it reaches narrow place in vessel where it may lodge and block flow Often associated with conditions that change endothelial lining of vessels. e.g. Atherosclerosis = accumulations of fatty deposits Artery cross sections. A.) Light micrograph of a normal artery. B.) Thinner wall of this artery changed as a result of atherosclerosis Hemophilia Acquired factors deficiency liver disease Vit. K deficiency Anticoagulant therapy Heparin Oral Anti- coagulants Massive Blood Transfusion DIC Hemophilia Hemophilia A Coagulation factor deficiency Inheritance Incidence Hemophilia B Factor VIII X-linked recessive 1/10,000 males (80-85%) Factor IX X- linked recessive 1/50,000 males (10-15%) SEVERITY RELATED TO FACTOR LEVEL < 1% - Severe - spontaneous bleeding 1-5% - Moderate - bleeding with mild injury 5-25% - Mild - bleeding with surgery or trauma LAB: PROLONGED PTT COMPLICATIONS : Soft tissue bleeding Clinical manifestations Hemophilia A & B are indistinguishable Hemarthrosis (most common) Fixed joints Soft tissue hematomas (e.g., muscle) Muscle atrophy Shortened tendons Other sites of bleeding Urinary tract CNS, neck (may be life-threatening) Prolonged bleeding after surgery or dental extractions Depends upon Type of surgery The level of native factors (VIII &IV) Half life of infused factors Hematologist consultation in case of massive bleeding Intermediate purity plasma products Virucidally treated May contain von Willebrand factor High purity (monoclonal) plasma products Virucidally treated Non functional von Willebrand factor Recombinant factor VIII Virus free/No apparent risk Non functional von Willebrand factor Mild bleeding Target: 30% dosing q8-12h; 1-2 days (15U/kg) Hemarthrosis, oropharyngeal or dental, epistaxis, hematuria Major bleeding Target: 80-100% q8-12h; 7-14 days (50U/kg) CNS trauma, hemorrhage, lumbar puncture Surgery Retroperitoneal hemorrhage GI bleeding Adjunctive therapy -aminocaproic acid (Amicar) or DDAVP (for mild disease only) Formation of inhibitors (antibodies) 10-15% of severe hemophilia A patients 1-2% of severe hemophilia B patients Viral infections Hepatitis B Hepatitis C HIV Human parvovirus Hepatitis A Other HIV -positive (n=382) 53% Negative Hepatitis B virus only Hepatitis C virus only Hepatitis B and C HIV-negative (n=345) 47% 1 1 24 74 20 1 45 34 Blood 1993:81;412-418 Agent High purity factor IX Recombinant human factor IX Dose Initial dose: 100U/kg Subsequent: 50U/kg every 24 hours Acquired factors deficiency liver disease Vit. K deficiency Anticoagulant therapy Heparin Oral Anti- coagulants Massive Blood Transfusion DIC Decreased synthesis of II, VII, IX, X, XI, and fibrinogen Since factor VIII of extrinsic pathway has the shortest 1/2 life, the onset of liver dysfunction will initially prolong PT (later PTT &a PTT) Dietary Vitamin K deficiency (Inadequate intake or malabsortion) Dysfibrinogenemia Enhanced fibrinolysis (Decreased alpha-2-antiplasmin) DIC Thrombocytoepnia due to hypersplenism Treatment for prolonged PT/PTT Vitamin K 10 mg SQ x 3 days - usually ineffective Fresh-frozen plasma infusion 25-30% of plasma volume (1200-1500 ml) immediate but temporary effect Treatment for low fibrinogen Cryoprecipitate (1 unit/10kg body weight) Treatment for DIC (Elevated D-dimer, low factor VIII, thrombocytopenia) Replacement therapy Fat soluble vitamin malnutrition → ↓ Vitamin k Relies upon bile for proper absorption biliary obstruction malabsortion → ↓ Vitamin k Intestinal flora play san important role in converting vitamin k sterilization of the gut by antibiotics Enema → ↓ Vitamin k Anticoagulant (Coumodin) competing with the binding site at liver Administration ↓ Vitamin k Factors: II, VII, IX, X are vitamin K dependent final step in their synthesis a carboxyl group is added to each clotting factor Naturally occurring anticoagulant Bearing a string negative charge Acts via anti-thrombin III which binds to thrombin and prevents it from converting fibrinogen to fibrin Acts with other cleavage enzymes on the intrinsic and common pathways Dosages: DVT: 24-48,000 units/24hs (IV infusion) Prophylaxis: 5000 units/8-12hrs → 7-10 days Laboratory lest of choice: PTT should be 1.2-2.5 normal Reversal Protamine sulphate : slowly IV 1mg/100units heparin More than 50 mg (anticoagulant ,flushing, bradycardia, hypotension) Intrinsic system (surface contact) Extrinsic system (tissue damage) Contact Factor XII XII a Tissue factor Pl..Thromboplastin Antecedent XI XI a Christmas Factor IX IX a Heparin → VIII VIII a Heparin→ Xa Stuart Prowers Factor X V Va II a Prothrombin II Fibrinogen Stable Factor VII VII a (-) anti-thrombin Thrombin Fibrin ← Heparin Dosage: 3-10mg daily ( → PT 2-4 x normal) Vitamin K1 (Phytomenadione ) as effective orally, iv, im Dosage in warfarin induced hemorrhage (or anticoagulant Over dosage) 2.5-20 mg Reversal takes 12 hours (vitamin k dependent dotting factors return to the plasma in order of their ½ life) if surgery can’t wait → FFP Permanent anticoagulant therapy (AF & value prosthesis ) → heparin during the period of suspended oral anticoagulant in an attempt to ↓ thromboembolic sequel e 5000 U of heparin/8-12hrs sc until warfarin is established This sub-pharmacological dose does not cause bleeding during surgery Clinical situation Guidelines INR therapeutic-5 Lower or omit next dose; Resume therapy when INR is therapeutic INR 5-9; no bleeding Lower or omit next dose; Resume therapy when INR is therapeutic Omit dose and give vitamin K (1-2.5 mg po) Rapid reversal: vitamin K 2-4 mg po (repeat) INR >9; no bleeding Omit dose; vitamin K 3-5 mg po; repeat as necessary Resume therapy at lower dose when INR therapeutic Chest 2001:119;22-38s (supplement) Clinical situation Guidelines INR > 20; serious bleeding Omit warfarin Vitamin K 10 mg slow IV infusion FFP or PCC (depending on urgency) Repeat vitamin K injections every 12 hrs as needed Any life-threatening bleeding Omit warfarin Vitamin K 10 mg slow IV infusion PCC (or recombinant human factor VII a) Repeat vitamin K injections every 12 hrs as needed Chest 2001:119;22-38s (supplement) Crystalloid, albumin, hetastarch → dilution of clotting factors Stored RBCs Dilutional Thrombocytopenia, ↓ Labile factors V &VIII DIC PT & a PTT require only minimum 30% of normal coagulant activity of any of the dotting factors, in order for these tests to be normal Systemic activation of coagulation Intravascular deposition of fibrin Thrombosis of small and midsize vessels with organ failure Depletion of platelets and coagulation factors Bleeding Poor bleed flow: Shock- hypotension , vascular occlusion Poor blood flow allows: platelets to aggregate, expose factors, initiate the intrinsic pathway of coagulation Liver disease: The diseased liver has a decreased ability to clear activated dotting factors, as well as FDP Releases thromboplastin into circulation → DIC. Tissue thromboplastin massive crush injuries major strokes obstetric catastrophes Amniotic fluid embolus Abruptio placenta Fetal death Presence of a phospholipid surface: In the process if DIC, the diffuse circulation of phospholipids throughout the blood steam, can produce so much thrombin that the antithrombin Ш is overwhelmed antithrombin Ш to limit & regular coagulation by binding to thrombin & other active cleavage enzymes in the intrinsic pathway The circulating phospholipids comes from TWO sources: Platelets can be activated throughout the blood stream by immune complexes or even by bacteria ( e.g.. Septic Shock) Diffuse Platelet aggregation & activation may also develop in pts who have large areas of denuded endothelium burn diffuse vacuities pre-eclampsia Consumption of coagulation factors; presence of FDPs Release of thromboplastic material into circulation Coagulation Fibrinolysis Fibrinogen a PTT PT TT Fibrinogen Plasmin Thrombin Presence of plasmin Fibrin Monomers FDP Fibrin(ogen) Degradation Products Fibrin Clot (intravascular) Plasmin Intravascular clot Platelets Platelets are consumed Fibrinolytic system fires up, Lyzing blood clots in an attempt to maintain blood fluidity Plasmin → FDP If FDPs are produced at a faster rate than they can be cleared → anticoagulant effect (normal half life 9hrs) (-) platelet aggregation Prevent the normal cross – linking of fibrin w is necessary to make a lot insoluble Blood flow, if compromised, should be improved by: Augmenting of CO Correction of acid Base disturbances Source of the circulating phospholipids must be removed: ↓fibrinolytic activity ↓ FDP Platelet transfusion FFP , Fresh blood, specific Component Heparin (Questionable give additional time to treat cause ) High dose impairs hemostasis Low dose: 15 U/kg 20 U/kg/hr for 24hrs Platelet count & fibrinogen level Heparin stopped or reduced Amino coproic acid ( ACA ) not recommended inhibit formation of plasmin → severe thrombo-embolic episodes Prophylactic Desmopression (DDAVP) ↓blood loss & transfusion requirements Dipyridamol limited platelet activation and aggregation Basic Hemostatic Mechanisms III. Fibrinolysis Blood vessel spasm, platelet plug formation, and blood coagulation provide homeostasis following tissue damage Activation (endothelial damage) Plasmin does not circulate in bl. stream as such because anti-plasmin circulate in conc. 10 X that of plasmin Plasminogen inactive TPA PLASMIN INHIBITORS Its precursor (plasminogen) circulate in bloodstream As clot evolves, it incorporates the plasminogen & an enzyme Called tissue plasminogen activator TPA (which convert plasminogen to plasmin) Plasmin ENZYME FOR FIBRINOLYSIS LYSIS FIBIN CLOT Fibrin Plasmin is produced within fibrin clot & shield from antiplasmin Then out of fibrin clot to blood FDP Anticoagulant Interfere with fibrin polymerization Metabolized by the liver Picked up with RES Antiplasmin rapidly neutralize & prevent wide spread uncontrolled fibrinolysis Excreted in kidney Is the bleeding local or due to a hemostatic failure? Local: Single site of bleeding usually rapid with minimal coagulation test abnormalities Hemostatic failure: Multiple site or unusual pattern with abnormal coagulation tests Evaluate for causes of peri-operative hemostatic failure Preexisting abnormality Special cases (e.g. Cardiopulmonmary bypass) Diagnosis of hemostatic failure Review pre-operative testing Obtain updated testing Identify and correct any specific defect of hemostasis Laboratory testing is almost always needed to establish the cause of bleeding Screening tests (PT,PTT, platelet count) will often allow placement into one of the broad categories Specialized testing is usually necessary to establish a specific diagnosis Use non-transfusional drugs whenever possible RBC transfusions for surgical procedures or large blood loss Definition Anemia is operationally defined as a reduction in one or more of the major RBC measurements: Hemoglobin concentration Hematocrit RBC count Anemia is a sign, not a disease Anemias are a dynamic process Its never normal to be anemic The diagnosis mandates lab work-up Etiology of Anemia • Anemias due to DECREASED ERYTHROPOIETIN PRODUCTION Renal disease Endocrine deficiency (pituitary, adrenal, thyroid, testis) Starvation Hemoglobinopathy (reduced oxygen affinity) • Anemias due to INADEQUATE MARROW RESPONSE TO ERYTHROPOIETIN Deficiency state (iron, vitamin B12, folate) Anemia of chronic disease (inflammation, infection, or malignancy) Sideroblastic anemia Myelo-dysplasia Pure red cell aplasia • ERYTHROCYTE LOSS Hemorrhage Hemolysis ANEMIA reticulocyte count UNDERPRODUCTION reticulocyte count INCREASED DESTRUCTION OR LOSS Increased reticulocytes (greater than 2-3% or 100,000/mm3 total) are seen in Blood loss Hemolytic processes 25% of hemolytic anemia will present with a normal reticulocyte count due to immune destruction of red cell precursors Retic counts are most helpful if extremely low (<0.1%) greater than 3% (100,000/mm3 total) To be useful the reticulocyte count must be adjusted for the patient's hematocrit The hematocrit is lower reticulocytes are released earlier from the marrow so one can adjust for this phenomenon. Thus: RC corrected = RC x (Hct /45) Reticulocyte index (RPI) = RC corrected / Maturation time (Maturation time = 1 for Hct=45%, 1.5 for 35%, 2 for 25%, and 2.5 for 15%.) RPI = 1 : (N. non-anemic ) RPI < 2 : hypo proliferative RPI > 2 : hyper proliferative UNDERPRODUCTION Low MCV Normal MCV (110 – 115) High MCV (>115) MCV (femtoliters) = 10 x HCT(percent) ÷ RBC (millions/µ) Microcytic Anemia Normocytic Anemia Macrocytic Anemia Megaloblastic B12/folate deficiency Iron deficiency Thalassemias Anemia of chronic dz Sideroblastic Pan cytopenias Red cell aplasia Anemia of chronic dz Sideroblastic Non-megaloblastic liver dz Hypothyroid Drugs that impair DNA synthesis Aplastic anemia Sideroblastic INCREASED DESTRUCTION OR LOSS LDH Bilirubin Haptoglobin Hemolysis G6PD deficiency Sickle cell Hereditary spherocytosis Autoimmune hemolytic anemia Drug-induced Hypersplenism DIC, TTP, HUS Acute Blood Loss ↓ Red cell mass → ↑ plasma vol. to preserve blood volume ODC → Right (Hb molecules less avid for O2 at any given PP to improve oxygenation) via ↑ 2,3 DPG ↑ Stroke volume ↑ Heart rate Maintenance of O2 delivery in anemia is dependent upon ↑ CO & Hb % Hb is an important buffer for CO2 induced pH change ODC will be adversely affected by hypocapnia (← to the left) Transfused Hb has 70% of normal 2,3 DPG level & there are unload O2 poorly → 24hrs is required to restore 2,3 DPG to normal level Key questions in history Is there evidence of bleeding? Duration Ethnicity Medications Physical exam Jaundice Lymphadenopathy, HSM, bone tenderness Other signs of heme abnormalities Hemolytic Anemias Hemolytic anemias are either acquired or congenital. The laboratory signs of hemolytic anemias include: Increased LDH (LDH1) Increased indirect bilirubin sensitive but not specific sensitive but not specific Increased reticulocyte count Decreased haptoglobin Urine hemosiderin specific but not sensitive specific but not sensitive specific but not sensitive The indirect bilirubin is proportional to the hematocrit, so with a hematocrit of 45% the upper limit of normal is 1.00 mg/dl and with a hematocrit of 22.5% the upper limit of normal for the indirect bilirubin is 0.5mg/dl Since tests for Hemolysis suffer from a lack of sensitivity and specificity, one needs a high index of suspicion for this type of anemia Avoid drugs that trigger hemolytic crisis Non opioid analgesics Antibiotics Sulphonamide Avoid drugs that associate with met Hb Prilocaine nitrupusside A Hemoglobinopathy with autosomal-dominant inheritance Homozygote: Sickle cell Disease (2 abnormal genes) Synthesize no Hb A RBCs contain 90-100% Hb S Heterozygotes: Sickle cell trait (1 abnormal gene) RBCs contain 20-40% Hb S *Hb-S : globin gene mutation Valine substitute Glutamic acid *Deoxygenation Valine translocated from position 6 to an external position interact with other hydrophobic elements within neighbouring globulin chain insoluble globin polymers sickling Deoxygenation of SS erythrocytes leads to intracellular hemoglobin polymerization, loss of deformability and changes in cell morphology OXYG - STATE DEOXYG -STATE Hb-S has different electrohporetic mobility (higher net electric charge) Deoxygenated Hb-S is less soluble, forming rod-like tactoids, distort RBC Sickle form Sickle cells prematurely destroyed hemolytic anemia Sickle cells cause increased blood viscosity impaired blood flow initiate thrombosis A) Deoxy-hemoglobin S B) Paired strands of 14-stranded polymer (electron micrograph) deoxy-hemoglobin S (crystal structure) C) Hydrophobic pocket for 6b Val D) Charge and size prevent 6 Glu from binding Dykes, Nature 1978; JMB 1979 Crepeau, PNAS 1981 Wishner, JMB 1975 1- Oxidative damage to cell membrane 2- Poor deformability of RBCs Sickling 3- RBCs become prone to dehydration prematurely removed by RES Hemolysis Infarction abnormal adhesion to endothelial cells Vaso-occlusion Vaso-occlusion Hypoxia Sickling tissue infarction….Cytokines Pain more Local Hypoxia& acidosis Micro vascular Blood Flow A- Hemolysis B- Vaso-occlusion • (RBCs survival) *Anemia. *Jaundice. *Gall stones. *CHF. *Leg ulcers. Bone marrow hyperplasia (Dysmorphic features). Delayed growth ( BW) • • • • Painful crisis (bone , muscle) Acute chest syndrome. CV stroke Eye damage. Functional hypo-splenism or auto-splenectomy C- Organ dysfunction LOCAL INFARCTIONS CAUSE THE CLINICAL PICTURE OF SICKLE CELL CRISIS Problems: ANEMIA CRISIS & PREVENTION PRE-EXISTING ORGAN DAMAGE SURGICAL PROCEDURE ( SICKLE RELATED ) INFARCTION RISK PREOPERATIVE ASSESS & PREMEDICATION I. Diagnosis II. Transfusion Therapy III. Fasting Limited I. Assess organ damage II. Sedation Over-sedation should be avoided Preoperative Assess & premedication I. Diagnosis CBC : Irreversibly sickled cell, target cells - Anemia, reticulocytosis - leukocytosis - Thrombocytosis - ESR - Bilirubin (indirect) - Electrophoresis Hb-S (with acidification) Solubility test (Ethnic Group) (adding reducing agent : 2% sodium Meta- bi-sulfate) Hb ppt if Hb-S > 15% Preoperative Assess & premedication II. Transfusion Therapy Mechanisms Simple transfusion – give blood Partial exchange transfusion - remove blood and give blood Erythrocytapheresis – use aphaeresis to maximize blood exchange Preoperative blood transfusion is considered to be a standard practice to maintain Hb > 10 gm/dl (intermediate or high risk) Hb A > 40)% For minor procedures , is no need for transfusion Transfusion Therapy Used correctly prevent organ damage Used unwisely serious complications. New England Journal of Medicine. 1995 ;333 :206-13 There no difference in the outcome in patients undergoing minor surgery whether the Hb-S is reduced to (30-34%) or Hb is maintained around 10 gm/dl Operative Hb-S levels has little correlation with the anesthetic management for SCD patients BJA 1998 ;80 :820-28 IF THE PATIENT IS STABLE AND THE RETICULOCYTE COUNT HIGH, TRANSFUSIONS CAN (AND SHOULD) BE DEFERRED Chronic steady-state anemia Uncomplicated pain episodes Infection Minor surgery Uncomplicated pregnancies A septic necrosis In severely anemic patients, simple transfusions should be used Common causes of acute anemia: acute splenic sequestration transient red cell aplasia Hyper-hemolysis (infection, acute chest syndrome, malaria) In general, patients should be transfused if there is sufficient physiological derangement to result in heart failure, dyspnea, hypotension, or marked fatigue Tends to occur during an acute illness or when hemoglobin falls under 5 g/dL. EXCHANGE TRANSFUSION: Bleed One Unit (500 Ml), Infuse 500 Ml Of Saline Bleed A Second Unit And Infuse Two Units Repeat. If The Patient Has A Large Blood Mass, Do It Again BENEFITS (FIRST CHOICE) Phenotypically Matched, Leuko-depleted Packed Cells A Post-transfusion Hematocrit Of 36 Percent Or Less Avoid Hyper Viscosity A COMPREHENSIVE TRANSFUSION PROTOCOL SHOULD INCLUDE ACCURATE RECORDS OF : The Patient’s Red Cell Phenotype Allo-immunization History, Number Of Units Received Serial Hb S Percentages Results Of Monitoring For Infectious Diseases And Iron Overload. Transfusions Usually Fall Into Two Categories: EPISODIC, ACUTE TRANSFUSIONS TO STABILIZE OR REVERSE COMPLICATIONS Limited studies have shown that aggressive transfusion (get Hb S < 30%) may help in sudden severe illness May be useful before general anesthesia LONG-TERM, PROPHYLACTIC TRANSFUSIONS TO PREVENT FUTURE COMPLICATIONS CONTROVERSIAL USES: Prior to contrast media exposure Sub-clinical neurological damage Priapism Leg Ulcers Pregnancy CONDUCT OF ANESTHESIA PRIME CONCERNS AVOID 5 HS: HYPOXIA Hypothermia Hypovolemia Hypercarpia Hypotension ADEQUATE ANALGESIA CONDUCT OF ANESTHESIA OTHER CONCERNS FIO2 MONITORING POSITIONING CAREFUL AVOID TOURNIQUET VENTILATE TO MILD RESPIRATORY ALKALOSIS AVOID BIER’S BLOCK POSTOPERATIVE HDU OXYGEN CHEST PHYSIOTHERAPY HYDRATION AVOID THE 5HS EARLY AMBULATION INFECTION IS A PARTICULAR RISK ANALGESIA