Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
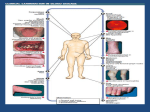
Thrombosis and Hemostasis Societies of North America April 15, 2016 Chicago, Illinois CRAIG S. KITCHENS, MD, MACP Professor Emeritus, University of Florida Gainesville FL DIC is now defined as a pattern of consequences due to the circulation of non-bound, non-inhibited THROMBIN and PLASMIN. These are generated via physiologic mechanisms (thrombin the end product of coagulation and plasmin the end product of fibrinolytic pathway) yet in pathologic quantities due to excessive amounts or duration of stimulation of the coagulation and/or fibrinolytic systems to the point that the natural inhibitors of thrombin and plasmin are overwhelmed so that they may circulate at large. Tissue Damage Infections Neoplasia Obstetric Conditions Trauma Crush injuries CNS injuries Heat Stroke Burns Hemolytic transfusion reaction Acute transplant rejection Cancers Leukemias Cancer chemotherapy Tumor lysis syndrome Miscellaneous Shock Cardiac arrest Near drowning, especially in fresh water Fat embolism Aortic aneurysm Giant hemangiomas Snake bites Gram-positive bacteria Gram-negative bacteria Spirochetes Rickettsiae Protozoa Fungi Viruses Abruptio placentae Placenta previa Retained dead fetus syndrome Amniotic fluid embolism Uterine atony Therapeutic abortion Toxemia of pregnancy Patient bleeding, thrombosing, or both, typically with progressive organ dysfunction. An underlying illness or process that may cause tissue damage, cell death, or production/release of tissue factor. Usually some perturbation exists of simple, readily available tests such as thrombin time (TT), prothrombin time (PT), partial thromboplastin time (PTT), fibrin degradation products (FDP)/D-dimer, or platelet count. These values may markedly change as the clinical situation changes. Mant & King: Am J Med 1979; 67:557 There is always an underlying problem that presents its own varied perturbations of many tests. Tests represent static “snapshots” of a highly dynamic situation. Special tests frequently are esoteric and results arrive long after the dynamic situation has changed. Diagnostic test results rarely direct or redirect therapy and may confuse the clinical picture. Table 7 Role of Blood Products in Treatment of DIC RBCs Keep hemoglobin in range of 6-10gm/dL Platelets Depends on risks for bleeding, not just the platelet count. Risk for bleeding high if less than 20,000-30,000/ L especially if due to decreased production; less so if due to sequestration or shortened platelet survival; nil if due to thrombotic causes (TTP or HIT). In DIC, reasonable target range is 50,000/ L FFP Enormously overrated in treatment of DIC, especially since recent evolution of our understanding and danger of TRALI. Some indication to supplement RBC transfusions in “total body exchange” situations Cryoprecipitate Probably best source of fibrinogen. Reasonable target is to keep fibrinogen levels between 50-100mg/dL 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. If you ask yourself “is this DIC?” it’s probably not There is always a cause that’s typically obvious What you see at the bedside depends on relative predominance of clotting vs thrombosis Keep lab tests simple and readily available Without appropriate clinical situation, lab tests are worthless “One new test for DIC” is hopelessly naïve Replace blood products judiciously Never “correct the coagulopathy” prior to needed procedure Don’t expect one therapeutic agent to work in all DIC Therapy depends on turning off the stimulus and correcting for volume, perfusion, acidosis, and hypothermia