Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
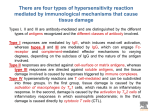
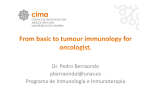
Examination dates • • • • • • • - 25 gennaio 12.00-14.00 aula da definire - 08 febbraio 12.00-14.00 aula da definire - 22 febbraio 12.00-14.00 aula da definire - 15 giugno 12.00-14.00 aula da definire - 28 giugno 12.00-14.00 aula da definire - 12 luglio 12.00-14.00 aula da definire - 30 settembre 12.00-14.00 aula da definire Immunity • Active • Preferred, it induces immunological memory • Passive Immunological memory • At the cellular level, immunological memory depends on epigenetic changes in T lymphocytes and B lymphocytes that allow a faster effector response to pathogens. Immunological memory in B cells may also reflect genetic alterations as immunoglobulin M (IgM) antibodies switch to IgA or IgG and somatic mutations enhance antibody affinity. There are two main kinetic patterns of expression for genes that are expressed at higher levels in memory T cells than in naive T cells. First, there are genes that are highly expressed in resting memory T cells compared with resting naive T cells. These highly expressed genes in resting memory T cells include genes involved in migration, homeostasis and readiness for activation. Second, there are genes that are highly expressed only after the activation of memory T cells; these genes are termed poised genes. Such poised genes are tightly regulated when the T cell is in the resting state but are rapidly induced after T cell activation. It is apparent that the function of these poised genes is not desired in the resting state, and therefore they are minimally expressed. These two patterns of expression for genes that are highly expressed in memory T cells show that the expression of such genes is precisely controlled in a time- and space-dependent manner to fulfil the function of memory T cells. An example from macrophages Vaccination The World Health Organization (WHO) estimate that vaccination averts 2-3 million deaths per year (in all age groups), and up to 1.5 million children die each year due to diseases which could have been prevented by vaccination. They estimate that 29% of deaths of children under five years old in 2013 were vaccine preventable. Vaccines: a success story in modern medicine “with the exception of safe water, no modality, not even antibiotics, has had a major effect on mortality reduction and population growth” Plotkin ‘A Short History of Vaccination’ in Vaccines Vaccines are one of the most important successes in modern medicine and immunology The greatest triumph in vaccination has been the global eradication of smallpox, announced by the World Health Organization in 1979. What vaccines do • Most vaccines generate antibodies that neutralize the pathogen and its associated toxins, and stop infection • In many cases, pre-existing antibodies must already be present at the time of infection (so vaccination must be performed before the subject is exposed to the pathogen) – Example: tetanus, for which you need antibodies to neutralize the fast damage caused by the powerful toxin • Indeed the toxin is so powerful that disease inducing doses may not be sufficient to induce an immune response, and survivors of tetanus need to be immunized anyway… • Immune responses to infectious agents generate several different antibodies, but only some of them are protective – Vaccination strategy should optimize the selection of protective antibodies Features of effective vaccines • Close to 100% safe (even a low level of toxicity is not acceptable) • Very effective: most if not all of the immunized people must be protected • Long-lasting: it is not practical to immunize entire populations repeatedly, the vaccine must generate memory • Cheap • Concept of “herd immunity”: as long as most of the individuals are immunized and therefore protected, not necessarily all of the individuals must be immunized (even unvaccinated members of the community are well protected, because the chance to encounter the pathogen is decreased) • Anyway, 80% or >80% levels of immunized population are required, so that when levels fall below sporadic epidemics can occur Vaccination in history • 2000 bC: Athenians who survived the 1st outbreak of plague were resistant to the disease when a 2nd outbreak occurred • E. Jenner (1749-1823) – Optimized “variolation” using cowpox • Smallpox from sick people was originally used, with several people dying from the disease (3-4%) • Jenner introduced cowpox and demonstrated its efficacy by intentionally infecting vaccinated people with smallpox (small amounts) – None of these approaches could have been considered acceptable by current ethical standards Limitations in vaccination strategies • Vaccination works extremely well for diseases that can be efficiently tackled by a strong Abmediated response • Many diseases (AIDS, malaria, tubercolosis) need both Ab- and cell-mediated immunity • Current vaccination approaches are relatively weak in eliciting a strong cell response Evolution in the development of vaccines • Initial approaches – Use of organisms with reduced pathogenicity started as a purely empirical approach, and evolved to the generation of genetically attenuated pathogens • Functional genomics studies of the pathogens • Identify genes important for disease • Generate strain with mutated genes: unable or with dramatically reduced ability to induce disease • Use these strains to vaccinate – Alternative approach: use killed organisms, or purified components of organisms • Example of “inactivated” purified component: use of inactivated toxins for tetanus – Modern vaccinology: based on better understanding of pathogenicity/immunogenicity, response to pathogenes, regulation of the immune system Public Health Clinical Medicine Public Health Individual Health Etica Medica Pub.Health Ethics Needs of the society vs individuals Autonomy Vaccination and public health Prospettiva individuale: Cosa dobbiamo agli altri? Prospettiva sociale: Quando l’intervento dello stato è giustificato? Giustizia sociale: Costi e benefici sono distribuiti equamente? Il dilemma centrale delle politiche vaccinali • LIBERTÀ DI SCELTA INDIVIDUALE? È un diritto dell’individuo l’astenersi dalla partecipazione alle campagne vaccinali? Queste scelte vanno rispettate come libera espressione dell’autonomia individuale? Sono da biasimare in quanto scelti miopi/egoistiche? • VACCINAZIONI OBBLIGATORIE? Lo stato ha il diritto di imporre campagne vaccinali obbligatorie? In quali casi (epidemie? pandemie?) Su quali basi giuridiche e morali? L’imposizione dell’obbligo vaccinale è un caso di paternalismo statale ingiustificato? Vaccino Salk(1952): virus inattivato, somministrato per via intramuscolare Vaccino Sabin(195): virus attenuato, somministrato per via orale I casi di polio negli USA diminuiscono drasticamente: 1952 58.000 casi 1955 inizio campagne vaccinali 1957 5.600 casi 1961 161 casi …la luna di miele con i vaccini Europa polio-free (OMS) Epidemia in Olanda Ultimo caso polio in Italia Vaccinazione obbligatoria in Italia Introduzione vaccino virus attenuato -Sabin 8300 casi di polio in Italia Introduzione vaccino virus ucisso - Salk 1957 1958 1964 1966 1983 1992 2002 Le campagne vaccinali di massa (obbligatorie) hanno permesso di eliminare malattie pericolose e invalidanti come il vaiolo e la poliomielite. Queste campagne hanno permesso, inoltre, di raggiungere l’immunità di gruppo: una certa percentuale di individui vaccinati protegge dall’infezione anche gli individui non vaccinati L’immunità di gruppo è un bene pubblico da mantenere •Vaccines must also be perceived to be safe. Bordetella pertussis causes whooping cough, which in small infants results in significant hospitalization (32% of cases), pneumonia (10% of cases)and death (0.2% of cases) •The whole cell vaccine against Bordetella pertussis was developed in the 1930's and childhood vaccination in the US reduced the annual rate of infection from 200/100,000 in the 1940's to less than 2/100,000. •Whole cell vaccine, given with tetanus and diphtheria toxoids, was associated with inflammation at the injection site. In a few children, high temperature and persistent crying occurred; very rarely, seizures or a transient unresponsive state were seen. •Anecdotal reports that irreversible brain damage might be a rare consequence of pertussis vaccination, coupled with two deaths in Japan, lead to a decline in vaccination rates in the late 1970's and a rise in whopping cough and death due to pertussis infection, especially in Japan and in Great Britain. •As a result of those 2 deaths in Japan that were feared to have been due to the vaccine, the vaccine was temporarily suspended, the given only to older children •A few years later there was a big outbreak (13000 cases) and 41 kids died. •Careful studies did not confirm that pertussis vaccination was a primary cause of brain injury, but in response to public concerns an acellular vaccine was developed containing purified antigens that induce protective immunity •This vaccine is as effective as the whole cell vaccine and does not induce the common side-effects of the original vaccine. •Recent anecdotal reports of association between childhood vaccination (particularly with MMR) and autism have raised concerns in parents; worldwide studies have found no association between the incidence of vaccination and autism. Il vaccino MMR è un vaccino trivalente contro morbillo, parotite e pertosse. Nel 1998 un medico inglese Andrew Wakefield pubblica uno studio su Lancet, proponendo una possibile associazione tra campagne vaccinali e casi di autismo. Propone che i tre vaccini vengano somministrati separatamente Nel Febbraio 2010, Lancet ritira la pubblicazione. Wakefield colpevole di frode scientifica Si possono giustificare campagne obbligatorie? Se sì, con quali argomenti? L’argomento del danno agli altri “the only purpose for which power can be rightfully exercised over any member of a civilized community, against his will, is to prevent harm to others. His own good, either physical or moral, is not a sufficient warrant” John Stuart Mill, On Liberty, 1859 La ratio legale per l’obbligatorietà • 1905: la Corte Suprema decide il caso Jacobson vs. Massachusetts: “There are manifold restraints to which every person is necessarily subject for the common good. […] a community has the right to protect itself against an epidemic of disease which threatens the safety of its members” Il problema dei free-rider Sono definiti free-rider coloro che godono dei benefici di un bene pubblico (nel nostro caso immunità di gruppo) senza partecipare alla sua creazione Il caso dei free-rider pone particolari problemi morali? Alcuni sostengono che, se l’immunità di gruppo non è minacciata, il comportamento dei free-rider non è moralmente reprensibile. Sarebbe sbagliato vaccinare oltre la soglia di immunità di gruppo Il valore morale dell’astensione non dipende dall’azione in sé ma dalle conseguenze. Figure 14-21 Live-attenuated viral vaccines • Many currently used antiviral vaccines (developed decades ago) consists of attenuated or inactivated viruses – Inactivated: treated to make them unable to replicate – Attenuated: grown by culturing the virus in vitro using nonhuman cells, they become less able to grow in human cells • They induce immunity but not disease • Compared to inactivated vaccines, they are >>>potent because they elicit efficient CD4 and CD8 T cell responses Figure 14-24 part 1 of 2 Figure 14-24 part 2 of 2 Caveats of attenuated vaccines • virus reactivation and induction of the disease – extremely rare, especially with new approaches to attenuation • In immuno-compromised individuals, attenuated viruses can be virulent and cause disease New approaches to development of attenuated vaccines • Identification of virulence genes – Introduce several mutations/delete the gene • Extremely rare the reactivation • Generation of an avirulent (nonpathogenic) virus that can be used to vaccinate Figure 14-25 part 1 of 2 Figure 14-25 part 2 of 2 Attenuated vaccines against bacteria and parasites • BCG: protects children against disseminated tubercolosis, but not effective against the adult pulmonary disease • Originally obtained from a pathogenic isolate of Mycobacterium bovis – More recent derivatives exploit recombinant DNA technologies ( example: BCG overexpressing a M.tubercolosis-antigen) Genetically attenuated parasites • Sporozoites with key mutated genes cannot infect productively liver cells, but can circulate in the bloodstream and elicit an immune response that (preclinical studies) is protective against infection by WT sporozoites Route of vaccination • It is important to consider the point of entry of the infectious agent – Even if immunity is systemic, it is possible to have differences in the efficacy of the immune response in different organs, and therefore one goals it to achieve maximum efficacy at the usual point of entry for the pathogen (i.e. lungs for influenza virus, etc…) • Usually vaccination occurs by injection – Intranasal vaccines are more effective to protect from upper respiratory tract infections by influenza viruses – Injected vaccines are more effective to protect from lower respiratory tract complications of the disease – Injection is expensive, requires trained people, etc…. • Orally administered antigens may induce tolerance rather than protection – it is important to understand the rules of mucosal immunity, a task that is ongoing Conjugate vaccines • Effort to produce acellular vaccines using isolated constituents of a pathogen • A single constituent rarely if ever can be obtained from a single antigen – Need to activate different types of immune cells to initiate an effective immune response • Conjugate vaccines: example vaccines against H. influenzae type B, responsible for meningitis – Vaccines directed against capsular polysaccharides • Children <2 yrs of age cannot develop good antibodies (because they need T cells to develop protective antibodies, while in older children and adults protective antibodies against capsule polysaccharides do not need T cells) – Bacterial polysaccharides have been coupled to protein carriers, that provide peptide antigens recognized by T cells • Now there is an effective T cell response Protective effect of vaccination against group C N. meningitis using conjugate vaccines Peptide-based vaccines • Approach to identify antigenic peptides: – Empirical – Reverse immunogenetics (see tomorrow for more details) • Peptide-based vaccines have drawbacks: – Difficult to identify antigens that are presented equally well by all MHC molecules – Tolerance my be induced – MHC class I processing pathway is not involved, so activation of CD8 T cells is restricted – Are not sufficient to stimulate the immune system, requiring adjuvants • Development of new peptide vaccines (example new HPV vaccines) – Use of very long peptides (100aa long), that can generate when processed several peptide epitopes that can be presented by different MHC molecules Figure 14-26 Computer Aided Vaccine Design • Problem of Pattern Recognition – ATGGTRDAR – LMRGTCAAY – RTTGTRAWR – EMGGTCAAY – ATGGTRKAR – GTCVGYATT Epitope Non-epitope Epitope Non-epitope Epitope Epitope • Commonly used techniques – Statistical (Motif and Matrix) – AI Techniques Adjuvants • Peptide-based vaccines require adjuvants to mimic how infection activates innate immunity, that induces dendritic cells to become optimally stimulatory for T cells • Alum (inorganic aluminum salts) are approved in US for use as adjuvants, In Europe also squalene (an oil) is used – Alum activates NLRP3 (innate immunity bacterial sensor mechanisms), thus inducing the inflammatory reactions that in the end lead to adaptive immune response DNA vaccination • Intramuscular injection of DNA (plasmids) encoding viral immunogens in mice-> – Umoral and cellular response that results in immunization of the mouse • In preclinical models, vaccination by DNA induces weak protection in many cases – Potentiation by plasmids expressing cytokines, or co-stimulatory molecules Figure 14-28 part 1 of 2 Figure 14-28 part 2 of 2 Could vaccines breed viciousness? • Gandon et al. used mathematical modeling to show that vaccines designed to reduce pathogen growth rates, or neutralize toxins, can diminish selection against virulent pathogens (host mortality) • The idea is that immunity (say to the toxin) reduces the risk of host death and shifts the optimal virulence higher. If hosts don’t suffer from the toxin, the pathogen can evolve to higher levels of virulence if that helps transmission (increases R0) • Post-vaccination, pathogens evolve to higher levels of intrinsic virulence in unvaccinated individuals • Can erode population-wide benefits and even increase overall mortality rates • Infection-blocking vaccines don’t have this problem Virulence-antigen vaccines • In principle, vaccines can also be used as evolutionary tools to favor evolution towards benignness, and Gandon et al.’s results do not apply generally. • Vaccines can exert selective forces: influenza, measles, hepatitis B • The virulence-antigen strategy describes how to use evolution to our advantage: • Target just the most virulent forms of a pathogen by making the virulence gene the target • Such vaccines should disproportionately suppress severe forms, but leave behind mild forms that can act as natural “vaccine” Virulence-antigen vaccines • The diptheria vaccine works in just this way • Active component is derived from diptheria toxin • When iron levels are low, Corynebacterium diptheriae produces the toxin, killing nearby cells and freeing up iron • Toxin is impotent in immunized person, just a waste of energy (about 5% of the protein budget to make a product that doesn’t work) • Toxigenic variants should be at a disadvantage • Accordingly, diptheria, but not C. diptheriae, has disappeared in areas using the vaccine • Mild forms persist even after immunization stops