Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
[CANCER RESEARCH 50, 4177-4189. July 15, 1990]
Special Lecture
Development of Antiestrogens and Their Use in Breast Cancer: Eighth Cain
Memorial Award Lecture1
Leonard J. Lerner and V. Craig Jordan
Department of Pharmacology, Jefferson Medical College, Thomas Jefferson University, Philadelphia, Pennsylvania 19107 [L. J. L.J, and Departments of Human
Oncology and Pharmacology, University of Wisconsin Clinical Cancer Center, Madison, Wisconsin 53792 [V. C. J.J
Abstract
This paper describes the laboratory discovery and clinical testing of
the first nonsteroidal antiestrogen, MER-25 (ethantoxytriphetol). The
compound blocks estrogen action in all species tested and has only slight
but transient estrogenic effects. No other antisteroidal actions are noted.
MER-25 is antiestrogenic in primates and was investigated in the clinics
in a wide range of gynecological conditions, including breast and endometrial cancer. Unfortunately toxic side effects (hallucinations, etc.)
precluded further investigation. A derivative of triphenylethylene, clomiphene, has some partial agonist (estrogen-like) actions in laboratory
animals and following clinical evaluation is now an established agent for
the induction of ovulation in subfertile women. Although clomiphene is
active in advanced breast cancer, it was not developed further. In the late
1960s a related compound, tamoxifen, was evaluated to treat a number
of estrogen-responsive disorders but was successfully introduced in the
1970s for the treatment of advanced breast cancer. Although there was
only modest initial interest in the palliative use of tamoxifen, an enormous
increase in basic and applied studies with antiestrogens resulted in a
definition of the target site-specific and tumoristatic actions of tamoxifen.
Close cooperation between laboratory and clinical evaluation has guided
the subsequent development of tamoxifen which is now available to treat
all stages of breast cancer. Long-term adjuvant tamoxifen therapy, a
concept developed in the laboratory, is currently the treatment strategy
of choice. The considerable success of tamoxifen has focused attention
on new antiestrogens with different pharmacological properties for other
potential clinical applications.
Introduction
Estrogen is involved in a large number of physiological phe
nomena throughout the body. The mechanism by which this
hormone produces its effects is complex and may not be uni
versal for all of the activities reported to be estrogenic. Estrogen
is also involved in some pathologies. Here too, its role has not
been completely defined. The removal of estrogen or interfer
ence with its action is helpful in elucidating the role of estrogen
and the mechanism of its activity in both physiological and
pathological processes.
Perhaps the earliest association of reproductive tissue and
behavioral responses to a hormonal secreting organ was the
cessation of estrus in domesticated animals following ovariectomy and the diminution of aggressive behavior in male animals
and humans after castration. Indeed, almost 100 years ago there
was recognition that the ovary was involved in mammary car
cinoma and that removal of that endocrine gland could be
beneficial to the patient (1).
Ablation of other endocrine organs including adrenalectomy
(2) and hypophysectomy (3) were also found to be beneficial in
some breast cancers. Surgical removal of these glands or the
ovaries, however, did more than decrease or eliminate endoge
nous estrogen from the body. A number of hormones and
nonhormonal substances were removed, some of which were
Received 4/5/90.
1Presented at the 80th Annual Meeting of the American Association for
Cancer Research, May 24, 1989, San Francisco, CA.
not involved in the pathology. However, it is reasonable to
expect a complex tissue such as the mammary gland, which
requires a number of hormones and probably growth factors
for its normal growth and function, to have the involvement of
more than one hormone in its pathology.
Certainly there are a number of possible ways of interfering
with estrogen interaction with its target tissue other than by
removing the steroid-secreting glands. Reduction of pituitary
gonadotropin secretion by sex steroids or by blocking the bioconversion of androgen to estrogen are ways of decreasing the
endogenous pool of estrogens. Biologically available estrogen
can also be reduced by increased catabolism or altering the
plasma level of estrogen-binding protein. Another way to inter
fere with estrogen activity is to block it at the level of its
receptor in estrogen target tissues.
Development of Nonsteroidal Estrogens
The most common of the wide spectrum of biological activi
ties associated with estrogens, regardless of chemical classifi
cation or source, is the uterotrophic response and the cornification of vaginal epithelium. These activities have been incor
porated into the bioassays that have defined every natural and
synthetic compound designated as an estrogen. Development
of a sensitive bioassay in rodents by Allen and Doisy (4) enabled
characterization and classification according to potency of the
natural steroidal estrogens and nonsteroidal plant estrogens.
This formed the basis to identify the structural requirements
for activity, as well as potency.
Cook et al. (5) found that the phenanthrene nucleus was not
necessary for estrogenic activity. The laboratory of Dodds and
his collaborators therefore synthesized a large number of diphenolic and triphenolic compounds resulting in the develop
ment of potent, clinically important estrogenic substances such
as diethylstilbestrol (6), hexestrol, and dienestrol (7). At this
same time in the mid-1930s, Robson and Schonberg reported
that triphenylethylene had estrogenic activity (8) and that oral
potency and prolongation of activity could be achieved by
bromination (9). This finding led, in the 1940s, to the synthesis
of a number of triphenylethylene derivatives including more
potent halogenated compounds by the William S. Merrell Co.
in the United States (10, 11) and by Imperial Chemical Indus
tries in the United Kingdom.
While all of the compounds called estrogens increase uterine
weight and stratify and cornify the vaginal epithelium, the
spectrum of other biological activities associated with estradiol
may or may not be present in all of these estrogens. Moreover,
the quantitative aspect of one of the activities may not be related
to other activities of the same compound.
Knowledge of structure-activity relationships allows for the
rational design of chemical agents with greater specificity for a
particular pharmacological action.
Some of the physiological interactions of the steroidal hor-
4177
Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1990 American Association for Cancer Research.
ANTIESTROGENS AND BREAST CANCER
mones were known in the first half of the 20th century. These
interactions could be additive, augmentative, synergistic, or
antagonistic depending upon the particular steroids, dosage of
each, order and time course of administration, as well as the
end point and species of animal under study. A small dose of
an estrogen administered to an immature rabbit prior to treat
ment with progesterone allows for maximal growth and devel
opment of the uterus.
It is now known that this effect is a result of increased
estrogen-induced uterine hyperemia and induction of proges
terone receptors. Large doses of the estrogen, however, can
reduce the subsequent effect of the progestational agent in the
rabbit.
ETHAMOXYTRIPHETOL (MER 25)
Estrogen Antagonism
Treatment of an immature or ovariectomized rodent with a
progestogen, androgen or corticoid can antagonize the uterotrophic effect of estrogens (12-16). Antagonism, however, is
closely linked to the relative and absolute dose of the agonist
and the antagonist.
The first estrogens that demonstrated antagonism of the
stimulation of another estrogen were estriol (17) and 16-epiestriol (18). These weak estrogenic steroids partially inhibited the
uterotrophic effect of estradiol in the rat. This antiestrogenic
activity was manifested only over a narrow range of doses (19),
and at lower doses the two estrogens induced additive uterine
growth responses (20). Moreover, for the end point of vaginal
cornification in rats and mice, estriol was always additive with
estradiol (21).
The nonsteroidal synthetic estrogens and their structurally
related weak or inactive relatives were an attractive source in
the search for modulators or inhibitors of estrogenic activity.
Several weakly estrogenic stilbene and triphenylethylene com
pounds demonstrated partial antagonism of estrone- or estradiol-induced uterotrophic activity in mice in my laboratory (L.
J. L.). At a presentation of data (22) on the antiestrogenic
activity of one of the diphenolic compounds Dr. Roy Hertz
from the NIH remarked that the findings were interesting but
a clinically useful antiestrogen would have to be much more
potent.
Discovery and Development
of Ethamoxytriphetol
(MER-25)
In 1954, a compound related to triphenylethylene and chlorotrianisene was synthesized at Merrell to study its possible
cardiovascular effects, but it was found to be inactive. The
structural similarities ofthat compound to those of the triphenylethylenes that were being studied for antiestrogenic activity
in my laboratory (L. J. L.) prompted us to test its endocrine
activity.
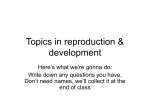
That compound,
l-/?-2-(diethylamino)ethoxyphenyl-2-(/>methoxyphenyl)-l-phenylethanol
was later given the generic
name of ethamoxytriphetol and the reference designation of
MER-25 (Fig. 1). The initial dose of MER-25 was selected on
the basis of experience that showed that even the most active
of the compounds tested up to that time were of low potency
and only partially inhibited the uterotrophic effect of estrone
or estradiol.
Weanling mice were given s.c. injections of MER-25 in olive
oil for 3 days at a daily dose of 1.7 mg (170 mg/kg). One-half
of the animals were also given daily injections of estradiol
benzoate (0.1 ^g/animal). The results of this experiment were
surprising since the uterine weights of the mice that had been
N1TROMIPHENE (CN-55, 945)
NAFOXIDINE(U-11,100A)
TAMOXIFEN (ICI 46, 474)
Fig. 1. Structures of MER-25 and antiestrogens derived from triphenyleth
ylene.
given MER-25 with or without estradiol benzoate were identical
to those of animals given injections of the olive oil alone. In
addition, uterine vascularity and intraluminal fluid, which also
increases with estrogen treatment, were absent in the MER-25treated groups. Moreover, body weight remained normal. The
study was repeated several times and the complete blockade of
the estrogen-induced uterotrophic response was confirmed.
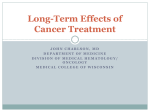
The inhibition of estradiol action in the mouse uterus by
MER-25 was dose related and simultaneous administration of
graded doses of estradiol was able to prevent the antiestrogenic
effects of MER-25 in a dose-related manner (Fig. 2). This study
demonstrated that MER-25 is a competitive antagonist of es
trogen action.
The nature of the competitive mechanism of this and deriv
ative antiestrogens was elucidated when Jensen et al. (23, 24)
found that they prevented binding of labeled estradiol to the rat
uterus. Numerous studies in vivo and in vitro have confirmed
that the nonsteroidal antiestrogens act at the level of the estro
gen receptor. However, the exact nature of the mechanism(s) is
still incompletely understood. Moreover, other activities have
been documented for this class of pharmacological agents.
These include inhibition of estrogen-induced protein synthesis,
thymidine incorporation, DNA synthesis, cell cycle blockage at
the Gìphase, inhibition of calmodulin, and non-estrogen-re
lated events.
Not all of these activities, however, have been found univer
sally with all antiestrogens and results from studies in vivo do
not necessarily support findings in vitro. Some of these effects
may be a result of the relative estrogenic to antiestrogenic
activities of the compound studied or to the biological half-life
of each activity. A comparison of an estrogenic antiestrogen
4178
Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1990 American Association for Cancer Research.
ANTIESTROGENS AND BREAST CANCER
50
(11F)
~.
O)
Estradiol
0.3 Mg
33 (16F,3P,4N)
40
(11F)
(1N,3P,7F)
(9N,1P,1F)
Fig. 2. Uterotrophic and antiestrogenic ac
tivities of MER-25 in immature mice. Groups of
animals were treated for 3 days with (A) estradici
benzoate (0.3 ng) and MER-25 (O) or MER-25
alone (A) or (B) different doses of estradici
benzoate with (d) or without (•)5 mg MER-25.
All doses are 3-day total dosages. Data in paren
theses, number of animals exhibiting full (/"),
l
30
(1N.7P.2F)
^
/>
4N.4P.3F)
20
partial (P), or no (AOuterine intraluminal fluid.
'Control
n
rControl
(25N)
(1P.33N)
(38N)
I
TOTAL
0.2
1.0
DOSE MER-25
(partial agonist) with a nonestrogenic antiestrogen (pure antag
onist) for each of the activities may help resolve this problem.
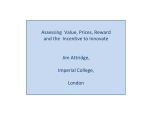
The antiuterotrophic effect of MER-25 was also demon
strated in immature, ovariectomized, and adult rats (25-30). In
the immature rat, a MER-25:estradiol benzoate ratio of 400:1
reduced the Uterotrophic effect of the estrogen by approximately
45% and complete suppression of the estrogen activity was
obtained with a ratio of 10,000:1 (Fig. 3). Uterine as well as
oviductal growth stimulated by estradiol was inhibited in a
dose-related fashion as were a number of biochemical parame
ters elevated by estrogen. These included nucleic acids, phospholipids, glucose-6-phosphate dehydrogenase and other en
zyme activities, nitrogen, and water.
These initial studies prompted my colleagues and I (L. J. L.)
to investigate the pharmacological spectrum of activities of
MER-25 in different species in various stages of maturity. Our
studies evaluated the antihormonal and antifertility properties
of MER-25 in acute and long-term studies (15, 26). Each study
brought new information but also raised new questions. MER25 was an antiuterotrophic agent regardless of the route of
administration or the estrogen used as the agonist, but it had
little or no activity as an antagonist of androgen or progester
one-induced Uterotrophic activity.
140
Total Dose of MER-25 - mg
Fig. 3. Uterotrophic and antiestrogenic activities of MER-25 in ovariecto
mized immature rats. Groups of animals were treated for 4 days with a total dose
of 2.0 fig estradiol benzoate (
), MER-25 <&\,estradiol benzoate plus MER25 (•)or injection vehicle (sesame oil) alone (
). Animals were killed on day
5 and blotted uteri were weighed wet.
(mg)
5.0
0.03
TOTAL
30.0
0.3
DOSE
ESTRADIOL
3000
<M9>
MER-25 was also a complete inhibitor of the effect of endog
enous estrogen or administered estrogen at the level of the
vagina. Cornification of vaginal epithelium by estrogen was
blocked and MER-25 did not induce any cornification when
administered to immature or ovariectomized mice or rats, dem
onstrating a lack of inherent estrogenicity.
Further Studies with MER-25
There was some evidence that this compound did posses very
weak and short-lived estrogen activity at other end points. At
relatively low doses, it induced a weak Uterotrophic effect which,
many times, was only borderline in significance. When a single
dose of this agent was administered to immature mice, a slight
increase in uterine weight was noted 48 h after treatment but
was not seen on subsequent days (26). Those doses that were
weakly Uterotrophic also elevated uterine alkaline phosphatase
(27).
In immature rats, lower doses induced minimal increases in
uterine weight (28). Low doses of MER-25 induced a short
lived increase in glucose-6-phosphate dehydrogenase, glucose
isomerase, and lipids (30). In the immature rabbit pretreated
with estrogen to allow for progesterone-induced endometrial
development, MER-25 effectively inhibited the estrogen activity
(presumed induction of progesterone receptors), thereby blunt
ing the effect of the progesterone (26). MER-25, however, when
administered instead of estradiol, permitted a weak uterine
growth response to subsequent progesterone treatment. Other
indications of weak estrogenic activity were the acceleration of
vaginal opening in prepuberal rats and mucification of the adult
rat vagina (26, 27). Offspring of rats treated with MER-25
during the last third of gestation demonstrated early opening
of their vaginas (27).
MER-25 has only weak antigonadotropin activity, but it
effectively blocks estrogen- or castration-induced pituitary hy
pertrophy and gonadotroph degranulation (26). It was found to
be devoid of any other hormonal activity.
Mouse uteri stimulated by testosterone were unaffected by
simultaneous treatment with this estrogen antagonist (26, 27).
High doses of MER-25, however, partially inhibited androgenstimulated uterine weight increase and biochemical changes in
the immature rat (29). Immature castrated male rats given
injections of MER-25 and testosterone propionate demon
strated no antagonism of the androgen-induced changes in the
seminal vesicles although there was a partial inhibition of the
4179
Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1990 American Association for Cancer Research.
ANTIESTROGENS AND BREAST CANCER
augmented weight and nucleic acids of the ventral prostate (32).
Antiestrogenic activity was also found in the chick. MER-25
inhibited estrogen-induced
oviductal growth and elevated
plasma phospholipids (26). MER-25 did not alter these same
estrogen target parameters at any dose used, indicating a lack
of estrogenicity in this species. Tamoxifen and other triphenylethylene antiestrogens (33, 34) were later also found to be
devoid of estrogen activity in the chick oviduct. This is confirm
atory evidence for a species-related hormonal profile for this
chemical class of compounds.
MER-25, if it were to have clinical potential, had to have
antiestrogenic activity in a primate. Ovariectomized Macaca
mulatta monkeys, maintained on estradici, were periodically
given varying p.o. doses of MER-25. The antagonist induced a
sharp reduction in the cornified vaginal cells of these estrogenized animals and at higher doses the decrease in cornified cells
was to the castration level. Accompanying this was a lessening
of the sex skin swelling and reddening and eventually estrogen
withdrawal bleeding (26). Other studies in intact cycling mon
keys demonstrated that endogenous estrogen was inhibited by
antagonism or via reduced gonadotropin secretion since the
menstrual cycles were lengthened and the percentage of corni
fied cells in the vaginal smear decreased.
These studies paralleled those in intact rats where a daily p.o.
dose of 1 mg lengthened the estrous cycle and 5 mg/day stopped
cycling (26). The rats resumed normal cycling of 2-6 days
following the last dose.
This prototype antiestrogen was further investigated in order
to determine its pharmacological properties especially in rela
tion to those biological phenomena where endogenous estrogen
or gonadotropins had been shown to be involved.
Effect of Antiestrogens on Reproduction
The reproductive system and all of its accessory tissues re
quire a changing balance of hormones for their development
and function. Changes in the absolute and relative quantities of
these hormones may lead to functional disorders and pathology.
Treatments that increase or decrease the available pool of the
particular hormone or alter its activity may correct the problem.
Similarly a physiological process such as ovulation can be
interrupted by addition of hormones.
It was interesting to explore the actions of MER-25, an
antiestrogen having weak gonadotropin-inhibitory
and very
weak selective estrogenic activities, on reproduction. The com
pound was administered to female rats at various times prior
to or after mating (26, 27). None of the pretreated animals
mated, since none of the animals exhibited estrus behavior or
showed vaginal cornification. Treatments that were initiated
after mating on day 1 of pregnancy probably inhibited nidation
or altered ova transport since no fetuses or products of concep
tion were found. Administration of the compound on days 4-7
postmating prevented blastocyst implantation. When treatment
was delayed until the 13th day of pregnancy, gestation contin
ued and live pups were delivered, but parturition was delayed
and was difficult with several of the young dying probably due
to the effects of estrogen deprivation on uterine contraction.
The postcoital antifertility effect of MER-25 was confirmed
by other investigators (35, 36) and similar results were obtained
for other triphenylethylene antiestrogens including clomiphene
and MRL-37 in my laboratories (L. J. L.) and by other inves
tigators (37, 38). None of the antiestrogenic agents were suffi
ciently efficacious in primates, although ovum implantation in
the monkey uterus was inhibited by several (39) and at least
one such agent was developed for postcoital antifertility utility
(40), but it was never marketed.
MER-25 was also shown to augment pregnancy maintenance
by progesterone in Ovariectomized rats similar to that obtained
with estrone (27). However, in rats fed a protein-free diet where
estrone helps maintain pregnancy, the administration of MER25 negated the supportive effect of the estrogen (27).
The activities of MER-25 were expressed relative to the
hormonal and developmental state of the animal. In adult
cycling rats, this compound decreased the weights and function
of the ovaries, pituitary, and uterus. It also antagonized the
effect of estrogen on the latter two organs (26). Administration
of MER-25 to pubertal rats, however, produced different re
sults. Ovarian weights, nucleic acids, and enzyme activities were
elevated after 4 days of treatment (41). The increases in the
ovaries were similar to that obtained by treatment with human
chorionic gonadotropin (41). Estradici treatment at the same
time prevented the MER-25-induced augmentation of ovarian
weight and biochemical activities.
The increase in ovarian activity following MER-25 treatment
of the pubertal rat may parallel the ovarian stimulation in
women after administration of antiestrogens including MER25 and clomiphene citrate.
Utility of Antiestrogens for Ovulation Induction
In the 1950s Dr. James H. Leathern used the human cho
rionic gonadotropin-treated
hypothyroid rat as a model for
polycystic ovaries. His work stimulated us to study the effect
of MER-25 in this model. The antiestrogen blocked the uterine
hypertrophy induced by the hyperactive ovary and reduced
ovarian weight; however, cystic follicles were still evident. These
studies were repeated and extended by Leathern and his grad
uate students. MER-25 prevented the induction of cystic ovaries
and alteration in ovarian ascorbic acid concentration (42). Fur
thermore, pretreatment with MER-25 prior to induction of the
hypothyroid state followed by gonadotropin administration was
also effective in blocking cystic development (43).
A preliminary study in nymphomaniac cows bearing cystic
ovaries was performed by W. Hansel and R. M. Melampy using
a low use of MER-25 that I (L. J. L.) had suggested. These
cows promptly resumed normal behavior; however, no meas
urement of ovarian follicular size or ovulation was recorded.
These findings in animals encouraged us to initiate explora
tory studies on selected patients to determine the effects of
MER-25 on menstrual or ovarian disorders. Kistner and Smith
(44) reported that patients treated for endometrial hyperplasia
and carcinoma with MER-25 demonstrated higher urinary ex
cretion of estrogen and follicle-stimulating hormone and had
temperature changes indicative of ovulation. These investiga
tors also induced ovulation with this compound in patients with
Stein-Leventhal syndrome (45). At this same time Tyler et al.
(46) reported that 6 of 18 patients with severe anovulatory
problems ovulated within 7 days of starting MER-25 therapy.
This antiestrogen, however, induced undesirable and unex
pected central nervous system symptoms leading to cessation
of its use. Fortunately my laboratory (L. J. L.) had been devel
oping, at the same time, another related but more potent
antiestrogen that had some qualitative differences from MER25. That compound, MRL-41 or clomiphene citrate (47) (orig
inally called chloramiphene) (Fig. 1), was, in comparison to
MER-25, weakly estrogenic (25). Clomiphene was provided to
R. W. Kistner, E. T. Tyler, and R. B. Greenblatt to study its
ability to induce ovulation. Shortly thereafter Greenblatt et al.
4180
Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1990 American Association for Cancer Research.
ANTIESTROGENS AND BREAST CANCER
(48) reported that this compound successfully induced ovulation
in women and similar successes were reported by the other
investigators. Ovulation was induced with doses that were
smaller than those used for MER-25 and no central nervous
system disturbances were found.
These studies ushered in a new mode for treating anovulatory
and infertile patients having functional ovaries which has had
widespread use in in vitro fertilization technology.
Effect of Antiestrogens on Lipids
Estrogens are known to regulate the synthesis and metabo
lism of lipids. This produces a change in the relative concentra
tion of various lipid fractions in the plasma and disposition in
tissues. Indeed endogenous estrogen is a normal protective
regulator for the cardiovascular system and the decreased syn
thesis of these steroids at menopause is associated with an
increase in atherosclerosis and coronary disease. Men are more
prone to these disorders than are premenopausal women. A
chemical compound that demonstrates an estrogen-like activity
on lipids without affecting the reproductive system would there
fore be desirable. Another possible partitioning of the biological
spectrum of activities of estrogen might result from the admin
istration of an estrogen such as estradiol and of a "nonestrogenic" antiestrogen.
An experiment in 1-week-old chicks showed that estradiol
benzoate could increase oviductal weight by 1500% while dou
bling the plasma phospholipid concentration. MER-25 admin
istration did not alter either end point even at doses 300 times
larger than that of the estrogen. When both substances were
administered to these birds the estrogenic effect on the plasma
phospholipids as well as on the oviduct were blocked (26).
Even though MER-25 failed to show an estrogen-like effect
on the chick plasma phospholipids, this antiestrogen and a
number of other compounds having different spectra of estro
genic and/or antiestrogenic activities were investigated in the
rat. MER-25, clomiphene citrate, and a related compound,
triparanol, were hypocholesterolemic (41) with the latter com
pound being 5 times more potent than the other two. Studies
in vitro with rat liver homogenates demonstrated that MER-25
and clomiphene inhibited the conversion of mevalonate to
cholesterol whereas triparanol produced its major blocking
effect after mevalonic acid (41, 49).
The nonestrogenic weak antiestrogen 2,2'"-(l-methyl-4,4diphenylbutylidene)bis(/>-phenyleneoxy)bistriethylamine
oxalate lowered plasma cholesterol in rats fed normal and hyperlipemic diets by blocking cholesterol biosynthesis between mev
alonate and lanosterol (49). It also reduced serum free fatty
acids and triglycérides.
It may be interesting to investigate the relationship of cho
lesterol biosynthesis inhibition and anticancer potential of the
antiestrogens in light of present knowledge concerning the
catalogue of factors required for cellular growth, development,
regulation, and multiplication.
Demonstration
Cancer
of the Efficacy of an Antiestrogen in Breast
Laboratory studies with MER-25, clomiphene, and many
other related compounds suggested a variety of potential clinical
utilities based on the particular pharmacological spectrum of
each compound. In mid-1956 a list of some of these utilities
was suggested for evaluation with MER-25. These included,
"1) precocious development, 2) anti-fertility, 3) habitual abor
tion, 4) fertility in the female, 5) dysmenorrhea, 6) all kinds of
menstrual disturbances including menorrhagia or prolonged
menstrual periods, 7) menopause, 8) endometriosis, 9) acne,
10) cancer—a) to test for or substitute for adrenalectomy in
cancer, b) as a substitute for ovariectomy, c) mammary carci
noma, d) prostatic cancer—alone or in combination with an
estrogen, in an attempt to maintain the effects of estrogen on
the prostate and avoid side reactions of estrogens, 11) benign
prostatic hypertrophy, 12) postpartum breast engorgement, and
13) precipitate the menopause when desirable."
While that list was compiled largely on the basis of laboratory
data on MER-25 presented by L. J. L., it is interesting that the
anticancer indications were not derived from animal tumor
models since such models were not available. The stimulation
for such evaluation in human cancers came largely from the
availability of a unique compound that could block the effect of
estrogen completely and also have weak gonadotropin inhibi
tion activity.
Several well known competent clinical investigators were
suggested for each of the areas. The two who were asked to
investigate MER-25 in breast disorders including cancers were
Dr. Roy Hertz at the NIH and Dr. Robert Kistner at Harvard
University. The dosages suggested were derived from the labo
ratory studies in animals including those performed in the
monkey. Dr. Kistner also investigated other diseases of the
breast, uterus, and ovaries.
Both investigators confirmed antiestrogenic activity in their
patients. Kistner and Smith (44) reported that patients with
chronic cystic mastitis not only had pain relief but also had
reduced glandular proliferation and breast size. He also found
that two of four patients with breast carcinomas experienced
pain relief and a reduction of calcium excretion while on MER25 therapy. Hertz also treated several patients with metastatic
breast cancer and obtained similar favorable results. These
studies demonstrated the utility of an antiestrogen in breast
cancer.
Unfortunately the investigation of MER-25 as a therapeutic
agent had to be discontinued because Drs. Hertz, Kistner, and
Tyler reported that their patients were experiencing hallucina
tions, psychotic episodes, nightmares, disturbed sleep, or other
indications of undesirable central nervous system activity.
Clomiphene which was the next most advanced in preclinical
investigation or another of the structurally related antiestrogens
could have been evaluated for anticancer activity in the early
1950s. However, the clinical evaluation of these compounds for
those indications was never undertaken due to the concentration
of effort on the use of clomiphene in induction of ovulation in
anovulatory infertile women. In fact clomiphene citrate was
later shown to have efficacy in breast cancer in a few patients
in 1964(50).
Resumption of investigation of similar antiestrogens for
breast cancer had to wait for more than a decade. Chemists and
biologists in the United Kingdom reexplored the triphenylethylenes for antiestrogenic and antifertility activity and eventually
for antitumor activity. The clinical efficacy of one of these
compounds, tamoxifen, established antiestrogens as the stand
ard endocrine treatment in breast cancer.
Development of Tamoxifen
Tamoxifen (ICI 46,474; Nolvadex) (Fig. 1) is a nonsteroidal
antiestrogen with antifertility properties in laboratory animals
(51-54). The compound exhibits an interesting species-specific
pharmacology (55); it is a pure antiestrogen in chicks (33) and
4181
Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1990 American Association for Cancer Research.
ANTIESTROGENS AND BREAST CANCER
an antiestrogen with partial estrogenic activity in rats (52) but,
in short-term tests, it is classified as an estrogen in mice (51,
52, 56). However, it appears that the prolonged administration
of tamoxifen to ovariectomized mice causes the uterus and
vagina to become refractory to the stimulatory effects of estra
dici (37, 57, 58).
Tamoxifen is a competitive inhibitor of estradici binding to
estrogen receptors (59, 60) and the compound inhibits the
binding of estrogen to estrogen target tissues in vivo (57, 6164).
Antiestrogens can inhibit estrogen-regulated events in cells
in culture; e.g., tamoxifen slows the growth of MCF-7 breast
cancer cells [in phenol red containing media (65, 66)]; however,
the addition of increasing concentrations of estradiol will re
verse the effects of tamoxifen and the cells will continue to
grow ("estrogen rescue") (67). Nevertheless, high concentra
tions of antiestrogens will cause estrogen irreversible actions
(68, 69). An "antiestrogen binding site" has been described (70)
but its relevance to the cytocidal actions of tamoxifen is not
clear. It is clear, however, that the high affinity of tamoxifen to
a variety of proteins causes ubiquitous binding of the drug in
vivo and probably accounts for its long biological half-life
Current research is focused on the action of growth factors
to regulate the breast cancer cell cycle. Estrogens decrease cell
cycle time and tamoxifen causes a reversible blockade at the G,
phase (71, 72). Antiestrogens inhibit estrogen-stimulated in
creases in transforming growth factor a, a stimulatory factor
(73), and there is a complementary rise in transforming growth
factor ß,
an inhibitory growth factor (74). Although the actual
regulatory mechanisms that orchestrate the inhibitory and stim
ulatory actions of growth factors are unclear, this is an area of
intense investigation.
The knowledge that tamoxifen is an inhibitor of estrogen
action focused attempts to develop an appropriate clinical ap
plication. Tamoxifen was initially evaluated in a number of
endocrine-responsive conditions (75-80) and the drug subse
quently became available in some countries for the induction of
ovulation in subfertile women. However, the discovery that the
presence of the estrogen receptor may predict the hormone
responsivness of advanced breast cancer (81) naturally led to
the evaluation of tamoxifen to control tumor growth [tamoxifen
inhibits the binding of estrogen to estrogen receptors derived
from breast tumors (82)]. Much of the credit for steering the
use of tamoxifen toward the treatment of advanced breast
cancer must go to the late Dr. Arthur L. Walpole of ICI,
Pharmaceuticals Division, Macclesfield, United Kingdom. Ear
lier in his career Dr. Walpole had been particularly interested
in carcinogenesis and cancer therapy but in the 1960s his
attention was directed, as head of the fertility control program,
to the development of antifertility agents (83). Much of the
early preclinical antitumor work was subsequently conducted
in my (V. C. J.) laboratory funded through the good offices of
Arthur Walpole at ICI.
Antitumor Actions of Tamoxifen in Laboratory Models
The first systematic laboratory study of the antitumor action
of tamoxifen was conducted at the Worcester Foundation for
Experimental Biology in Shrewsbury, MA (82, 84-88). One of
the results of this research (89, 90) was to encourage the clinical
evaluation of tamoxifen in the United States by the Eastern
Cooperative Oncology Group.
Most of the early research on tamoxifen used carcinogeninduced rat mammary tumor models (85-90) but during the
past half-decade interest has focused on an evaluation of the
antitumor action of tamoxifen in athymic mice, heterotransplanted with breast cancer cell lines (91-95).
Carcinogen-induced Models. Mammary tumors can be in
duced in 50-day-old Sprague-Dawley rats by a single feeding
(20 mg in 2 ml peanut oil) of DMBA. Tamoxifen will inhibit
the initiation (85, 87) and growth (61, 88, 96-98) of DMBA2induced tumors. The model system could be likened to the
treatment of advanced breast cancer but the tumors do not
metastasize and therefore a direct analogy with breast cancer is
impossible. This fact is important inasmuch as the fashion for
the treatment of breast cancer was changing in the mid-1970s.
A strategy was devised to use adjuvant hormonochemotherapy
to destroy micrometastases following mastectomy, a treatment
aimed at curing a majority of patients. Unfortunately no animal
model system was, or is, available to duplicate the clinical
situation to test the value of this treatment strategy in the
laboratory. Nevertheless the DMBA- and yV-methylnitrosoureainduced rat mammary carcinoma models were adapted to eval
uate whether antiestrogens could "cure" animals with a micro
scope tumor burden.
When DMBA is administered to Sprague-Dawley rats, the
initiated mammary cells are promoted by circulating hormones
to effect transformation. Palpable tumors appear 100-150 days
after DMBA. There is therefore a period when microscopic
disease can be treated to establish whether it is possible to cure
the animals with antiestrogens. If different doses are adminis
tered for 4 weeks starting at different times after DMBA (99,
100), a delay occurs in the appearance of tumors. In contrast
continuous therapy causes the majority of animals to remain
tumor free (101-103). Nevertheless of tamoxifen therapy is
stopped, tumor growth recurs (104).
A similar situation occurs with the carcinogen jV-methylnitrosourea; a short course of tamoxifen delays the appearance
of tumors but the animals remain tumor free during a contin
uous treatment regimen (105, 106).
Athymic Mouse Models. Breast cancer cell lines can be heterotransplanted into athymic immunodeficient mice. Estradiol
encourages the growth of hormone-responsive lines (e.g., MCF7) but hormone nonresponsive lines (e.g., MDA-MB-231) will
grow with or without estrogen treatment. Tamoxifen and its
metabolites inhibit estrogen-stimulated growth of estrogen re
ceptor-positive tumors but in general do not inhibit the growth
of receptor-negative tumors (91, 92). However, this model has
been used successfully to determine whether tamoxifen pro
duces a tumoristatic or tumoricidal effect on implanted hor
mone-responsive breast cancer cells. If animals are treated for
1, 2, or 6 months with sustained release preparations of tamox
ifen the tumor cells are not specifically destroyed. When the
animals are treated with estradiol to identify surviving tumor
cells, tumors regrow in every case (92, 93).
Overall the experimental evidence points to the fact that
tamoxifen is a tumoristatic rather than a tumoricidal agent.
Long-term adjuvant tamoxifen treatment, or treatment until
relapse, is predicted to be the best therapeutic strategy to control
the recurrence of breast cancer following mastectomy. This
application of tamoxifen can be called chemosuppression.
Long-Term Adjuvant Tamoxifen Therapy
Despite the developing laboratory data that demonstrated
that tamoxifen is a tumoristatic agent (99-102), the vast ma2The abbreviation used is: DMBA, dimethylbenzanthracene.
4182
Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1990 American Association for Cancer Research.
ANTIESTROGENS AND BREAST CANCER
jority of clinical trials initially evaluated 1 or 2 years of adjuvant
tamoxifen therapy. There were several sound reasons for this:
(a) a short course of tamoxifen might produce a tumoricidal
effect before the onset of resistance since it was known that
patients with advanced disease respond to tamoxifen for only
1-2 years; (b) the adjuvant use of tamoxifen might encourage
the early outgrowth of receptor-negative disease (the rationale
was that it would be wiser to save the drug until recurrence so
that physicians would have something available to treat the
patient); and (c) the long-term side effects of tamoxifen were
unknown (thousands of women with advanced disease had been
treated, but only until relapse, 1-2 years later).
Although tamoxifen was initially used conservatively the
recent overview of all randomized clinical trials (107) has
demonstrated the survival advantage of postmenopausal, nodepositive women who received 1 or 2 years of adjuvant tamoxifen
therapy. Swayed by the encouraging clinical trial results and
the laboratory findings (101, 107) clinical trials are currently
focused on an evaluation of 5, 10, or in some cases indefinite
adjuvant tamoxifen therapy in pre- and postmenopausal pa
tients with node-positive and node-negative disease.
In 1977, on the basis of encouraging laboratory data (101),
Dr. Douglass C. Tormey organized a pilot nonrandomized
adjuvant clinical study to identify any unusual side effects
produced by long-term adjuvant tamoxifen therapy (5 years)
and to evaluate the potential efficacy of the treatment strategy
(108). The results demonstrated the safety of tamoxifen and
provided promising preliminary data to establish the Eastern
Cooperative Oncology Group protocols EST 4181 and EST
5181 to evaluate chemotherapy and different lengths of tamox
ifen therapy in randomized clinical trials (109).
The National Surgical Adjuvant Breast and Bowel Project
has chosen a similar course of action. Based upon their suc
cessful evaluation of 2 years of adjuvant tamoxifen and chemo
therapy (110) they conducted a registration study of chemo
therapy and tamoxifen for 2 years followed by an additional
year of tamoxifen for those patients who did not have recur
rence. The results are encouraging and support the view that
long-term tamoxifen therapy benefits the patient (111).
Several clinical trials have also evaluated the efficacy of longterm adjuvant tamoxifen therapy alone. A French study (112)
has compared 3 years of adjuvant tamoxifen therapy versus no
treatment. Tamoxifen produced a survival advantage especially
in receptor-positive patients. Similarly a large clinical trial in
Scotland (113) has evaluated whether it is an advantage to treat
patients for 5 years with adjuvant tamoxifen. This clinical study
is particularly interesting because it addresses the question of
whether to use tamoxifen as an adjuvant therapy or to use the
drug only when the patient develops advanced disease. In the
Scottish study, patients in the control arm received tamoxifen
at first recurrence. The results demonstrate that long-term
adjuvant therapy with tamoxifen provides an effective control
of disease recurrence and a survival advantage for the patient.
There appears to be no need to delay the drug until recurrence
because early drug resistance does not develop.
The National Surgical Adjuvant Breast and Bowel Project is
currently conducting a trial of long-term adjuvant tamoxifen
therapy (10 years) in pre- and postmenopausal patients with
node-negative estrogen receptor-positive disease. The prelimi
nary results are again encouraging (114) inasmuch as tamoxifen-treated women have an extended disease-free survival.
Overall the clinical trials community has demonstrated some
advantages for long-term adjuvant tamoxifen therapy. To date
the trial population has been diverse with both pre- and post
menopausal women receiving tamoxifen alone and women with
node-negative disease who might be treated for decades. This
expanded and extended use of tamoxifen requires an ongoing
evaluation of the pharmacology and potential toxicological
consequences of indefinite therapy. Obviously it is important
to establish the safety of tamoxifen to reassure both physicians
and patients and to avoid unwarranted restrictions on this
valuable chemosuppressive therapy.
Clinical Pharmacology
The clinical pharmacology of tamoxifen was initially inves
tigated in patients with advanced breast cancer (115-118). The
drug is readily absorbed following p.o. administration and
accumulates to steady-state levels by the end of the first month
of treatment (116). The serum levels of tamoxifen at steady
state are extremely variable (50-300 ng/ml) but blood levels
are not related to response (119). The principal metabolite of
tamoxifen is ,/V-desmethyltamoxifen which produces blood lev
els approximately twice as high as those of tamoxifen by the
end of the first month of treatment. The serum half-lives of
tamoxifen and W-desmethyltamoxifen are extremely long (7
and 14 days, respectively) (120), probably because the com
pounds are highly protein bound.
Tamoxifen is extensively metabolized in patients (121, 122)
(Fig. 4) but to date no significant quantities of estrogenic
metabolites have been noted that would cause concern during
long-term adjuvant tamoxifen therapy. ,/V-Desmethyltamoxifen
is further metabolized to metabolite Y which has a glycol side
chain (123, 124). Tamoxifen is also converted to 4-hydroxytamoxifen but this is observed only at low concentrations in
serum (118). However, this metabolite has an extremely high
binding affinity for the estrogen receptor (the same as that of
estradici) (125); therefore it probably plays a significant role in
supporting the antitumor action of tamoxifen. Recently 4hydroxy-yV-desmethyltamoxifen has been identified in patients
(126). This metabolite has been shown in the laboratory to be
N-DESMETHYLTAMOXIFEN
N.N. DIDESMETHYLTAMOXIFEN
4-HYDROXY N-DESMETHYL
TAMOXIFEN
METABOLITE Y
Fig. 4. Metabolites of tamoxifen identified in patients.
4183
Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1990 American Association for Cancer Research.
ANTIESTROGENS AND BREAST CANCER
formed from either 4-hydroxytamoxifen or jV-desmethyltarnoxifen(127).
The blood levels of tamoxifen and its metabolites are stable
for up to 10 years of adjuvant therapy and no metabolic toler
ance seems to occur. This fact and the low incidence of reported
side effects (121) makes tamoxifen an ideal long-term chemosuppressive agent for the adjuvant treatment of breast cancer.
Potential Side Effects of Long-Term Adjuvant Tamoxifen Ther
apy
Tamoxifen therapy is being extended beyond a decade. Indeed
node-negative patients with only a moderate risk of recurrence
may in fact receive the drug indefinitely. This raises important
questions about the potential long-term side effects of nonsteroidal antiestrogens (Table 1).
Estrogen is important in prevention of the development of
osteoporosis in women; therefore the long-term administration
of an "antiestrogen" would seem to imply that women may
become predisposed to osteoporosis. Similarly estrogen pro
tects women from coronary heart disease by altering the circu
lating levels of cholesterol. Again it would seem that the longterm administration of an "antiestrogen" might not be benefi
cial. However, tamoxifen exhibits some estrogen-like effects
that appear to have target site specificity (55). Tamoxifen is an
antiestrogen in the rat uterus (52) but displays estrogen-like
effects in bone (128, 129). There are only few clinical data (130,
131) to support these beneficial laboratory findings but tamox
ifen is clearly not detrimental to bone in patients. The beneficial
effects of nonsteroidal antiestrogens on serum cholesterol has
been noted previously in animals (41) and tamoxifen has been
shown to lower serum cholesterol (mainly, low density lipoprotein) in patients (132, 133).
Obviously the beneficial estrogen-like effects of tamoxifen in
some target sites may prove to be a disadvantage in others.
Estrogens can cause an increase in thromboembolic disorders
and estrogen replacement therapy has been associated with an
increase in endometrial carcinoma. Tamoxifen does not, how
ever, cause a significant increase in thromboembolic disorders
when administered alone but there is a small decrease in antithrombin III during long-term adjuvant tamoxifen therapy
(132, 134). The decrease (generally not more than 30%) is,
however, not great enough to cause clinical concern. Neverthe
less patients with a history of thromboembolic disease probably
should not be treated with tamoxifen.
There is very little information about the effects of tamoxifen
on the human uterus although tamoxifen does have some
efficacy for treating endometrial carcinoma (135). Nevertheless
tamoxifen has been implicated (anecdotally) in the development
of endometrial carcinoma (136). Realistically, however, there
is little possibility that tamoxifen could control the growth of
all endometrial tumors as only about 1 of 3 are hormone
responsive. Interestingly enough there is one provocative labo
ratory observation (137) that tamoxifen can encourage the
growth of a human endometrial carcinoma in athymic mice.
Indeed this effect appears to be tumor specific (138). If athymic
mice are bitransplanted with the endometrial tumor EnCalOl
and the breast tumor MCF-7 and treated with estrogen and
tamoxifen, the endometrial tumor is stimulated to grow whereas
Table 1 Potential side effects of long-term adjuvant tamoxifen therapy
Antiestrogenic actions
Estrogenic actions
Reproductive
Osteoporosis, coronary heart disease
Clotting, uterine stimulation
Ovarian, teratogenesis
the growth of the breast tumor is controlled by tamoxifen. One
large clinical trial (139) has shown that a similar phenomenon
can occur during long-term adjuvant tamoxifen therapy; Le,
second breast tumors are reduced but there is an increase in
endometrial carcinoma. To date these data have not been con
firmed by any other major clinical trials organization and it is
important to state that adjuvant tamoxifen therapy should not
be denied to a patient on the basis of this potential side effect.
It should be obvious that tamoxifen is of proven benefit (107)
for the treatment of breast cancer, a disease that is invariably
fatal, and endometrial carcinoma, should it occur, has a good
prognosis. Routine gynecological examination must be per
formed to monitor the health and well-being of the patients
during adjuvant tamoxifen therapy.
Finally, since more and more premenopausal patients are
receiving adjuvant tamoxifen therapy, it should be stressed that
they are at risk for pregnancy and require counseling about
barrier contraceptives. Short-term tamoxifen treatment causes
an increase in ovarian estrogen synthesis (140) and premeno
pausal patients on long-term adjuvant tamoxifen regimens (with
or without chemotherapy) continue to menstruate and have
elevated circulating ovarian steroid hormone levels (141, 142).
It is currently not known what the long-term effects of tamox
ifen on the ovary will be; this is a topic for future clinical
investigation.
Clearly the elevated levels of estrogen, a known tumor mitogen, might be able to impair the antitumor action of the
antiestrogen. Tamoxifen is, however, an effective antitumor
agent in premenopausal women with advanced disease (121).
This clinical situation has been investigated in the athymic
animal model, and similar high circulating levels of estradici
(500-800 pg/ml) do not reverse the antitumor action of tamox
ifen (50 ng/ml).3 However, compliance issues with tamoxifen
will be very important in premenopausal patients during longterm adjuvant tamoxifen. Strategies to lower circulating estro
gen like oophorectomy or the administration of luteinizing
hormone-releasing hormone agonists during adjuvant tamoxi
fen therapy should be evaluated in future clinical trials.
New Antiestrogens
A study of the structure-activity relationships of tamoxifen
has provided an important insight into the mechanism of action
of both estrogens and antiestrogens. Early work demonstrated
that antiestrogens had a weak interaction with the estrogen
receptor (59, 143) and it was widely believed that this property
was essential to inhibit hormone action (144); i.e., an estrogen
would bind tightly to the receptor and the resulting complex
could initiate estrogen-dependent events whereas an antiestro
gen would bind to the receptor to block the access of estrogen
but the complex would "fall apart" before it could itself initiate
estrogen action. The discovery of the pharmacological proper
ties of monohydroxytamoxifen
(4-hydroxytamoxifen)
(125,
145) changed this view of antiestrogen action. 4-Hydroxytamoxifen has an affinity for the estrogen receptor similar to that
of estradici but it is a potent inhibitor of estrogen action.
Subsequent confirmation of this work (146, 147) and the avail
ability of radiolabeled material for studies in vitro and in vivo
(147-150) has established the drug as a standard laboratory
biochemical.
During the 1980s a number of assay systems in vitro were
used to describe the structure-function relationships of anties3 Y. lino and V. C. Jordan, unpublished observation.
4184
Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1990 American Association for Cancer Research.
ANTIESTROGENS AND BREAST CANCER
trogens (151-157). These model systems are important as they
provide information about the direct effects of ligands on the
cell without metabolic transformation. In the future this knowl
edge will undoubtedly dovetail with current research on the
molecular biology of the estrogen receptor to understand the
complex conformation changes that occur in the receptor pro
tein to program cell replication.
As a result of the successful use of tamoxifen to treat breast
cancer, several new antiestrogens are now being evaluated in
the laboratory and the clinic. The structures of several of the
new compounds are shown in Fig. 5. The literature on new
antiestrogens is increasing dramatically and interested readers
should consult recent reviews (122, 158).
One notable advance is the investigation of nonestrogenic
antiestrogens for potential clinical applications. The discovery
process appears to have gone full circle (MER-25 has few
estrogenic properties) to find compounds without the estrogenlike properties of the triphenylethylenes. At present only one
compound (ICI 164,384) is available for evaluation and it has
demonstrated activity as an inhibitor of estradiol action both in
vivo and in vitro (159-162). Interestingly the steroid also has
the ability to inhibit tamoxifen-stimulated tumor growth in the
laboratory (Ref. 94; Fig. 6). Various pure antiestrogens are
currently being evaluated in the laboratory and some are
undergoing toxicology testing. When (or if) any of these new
compounds become available for clinical application, they may
provide some additional clues about estrogen-regulated breast
cancer growth. One question has been whether the antitumor
activity of tamoxifen is related to its estrogenic or antiestrogenic
properties (or neither?) This could soon be resolved. It is
possible that pure antiestrogens could produce longer responses
in advanced disease or be useful as a second line therapy after
long-term adjuvant tamoxifen treatment. This presupposes that
a significant proportion of patients who eventually fail tamox
ifen therapy do so because of the estrogen-like properties of
tamoxifen. Unfortunately the potential of pure antiestrogens to
produce osteoporosis or early atherosclerosis may preclude
their use as a front line long-term adjuvant therapy in nodenegative disease.
TRIOXIFENE
DROLOXIFENE
TOREMIFENE
'"ICH j),0C N (CMjljCH,
ICI 164, 384
CH,
Fig. 5. Structures of new antiestrogens that are being evaluated in the labo
ratory and the clinics.
O
111
K
DC
O
D
WEEKS
Fig. 6. Effect of the nonestrogenic antiestrogen ICI 164,384 on tamoxifenstimulated growth of endometrial tumor EnCa 101 in the athymic mouse. Animals
were treated with a sustained release preparation of tamoxifen (2-cm Silastic
capsule) (D), a control capsule (O), or ICI 164,384, 1 mg/0.1 ml peanut oil s.c. 3
times weekly (•)or tamoxifen plus ICI 164,384 (•).
Current and Future Uses of Antiestrogens
In the 30 years since the first publication of the pharmaco
logical properties of MER-25, the clinical application of antiestrogens has proved to be a remarkable success. Tamoxifen is
now the antihormonal treatment of choice for advanced breast
cancer (pre- and postmenopausal). As valuable as this applica
tion is as a palliative treatment, the remarkable advances have
undoubtedly been made in the application of antiestrogens to
treat all stages of breast cancer. Tamoxifen is the antihormonal
treatment of choice for the adjuvant therapy of postmenopausal
node-positive women. Two years of treatment is known to
produce a survival advantage, and longer treatment schedules
are being evaluated to exploit the known tumoristatic qualities
of tamoxifen. We already know that long-term adjuvant tamox
ifen therapy (5 years) is beneficial compared to saving tamoxifen
until first recurrence, so 10-year and indefinite schedules are
being evaluated.
The proven efficacy and low incidence of side effects have
encouraged the evaluation of adjuvant tamoxifen therapy in
pre- and postmenopausal women with node-negative disease.
At present the long-term toxicological concerns appear to be
negligible compared to the known course of breast cancer
without treatment. Hundreds of thousands of women could be
being treated indefinitely with tamoxifen by the turn of the
century. Indeed it has even been suggested that antiestrogens
could be used to prevent breast cancer. However, the timing
and cause of the carcinogenic insult are unknown; therefore the
use of antiestrogens as true preventives seems impractical. A
better term, also applicable to adjuvant therapy, is chemosuppressive; i.e., the drug can be used to suppress subclinical disease
and prevent the appearance of a primary tumor (163). In some
adjuvant trials tamoxifen inhibits the development of second
primary breast tumors (114, 139, 164) and an early clinical
evaluation of the toxicology of tamoxifen in normal women has
been reported (165) as a first step in a prevention study.
Nevertheless there is a real concern about being able to target
the right population. We cannot predict who will develop breast
cancer; we can only guess at the probability. Furthermore "high
risk" women are, in fact, only a minority of those who will
develop breast cancer so any success must be balanced against
as yet unknown accumulative toxicities.
Is this the end of the possible applications for antiestrogens?
Certainly not. We have obtained valuable clinical information
4185
Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1990 American Association for Cancer Research.
ANTIESTROGENS AND BREAST CANCER
about this group of drugs that can be applied in other disease
states. Research does not travel in straight lines and observa
tions in one field of science often become major discoveries in
another. Important clues have been garnered about the effects
of tamoxifen on bone and lipids so it is possible that derivatives
could find targeted applications to retard osteoporosis or ath
erosclerosis. The ubiquitous application of novel compounds to
prevent diseases associated with the progressive changes after
menopause may, as a side effect, significantly retard the devel
opment of breast cancer. The target population would be postmenopausal women in general, thereby avoiding the require
ment to select a high risk group to prevent breast cancer.
20.
Acknowledgments
21.
This paper is not intended to be an encyclopedic review article but is
offered only as a personal recounting of research conducted in our
respective laboratories during a period that has spanned almost 40
years. We sincerely acknowledge the support of colleagues, students,
and assistants in our respective laboratories. We also acknowledge the
important additional contributions made to the understanding of an
tiestrogen action by James H. Clark, Kathryn B. Horwitz, Benita and
John Katzenellenbogen, Marc E. Lippman, C. Kent Osborne, Robert
I. Nicholson, Henri Rochefort, Robert L. Sutherland, and Alan E.
Wakeling. The influence of our teachers the late James H. Leatham
and the late James B. Allison (L. J. L.) and Edward R. Clark (V. C. J.)
was important for the direction and development of our investigative
approach. Dr. Lerner is ever grateful for the encouragement he received
as a developing scientist from Roy O. Creep, Roy Hertz, the late Albert
Segaloff, and the late Ralph Dorfman. Dr. Jordan wishes to acknowl
edge William L. McGuire, Jack Gorski, Elwood V. Jensen, the late
Arthur L. Walpole, and colleagues at ICI for their invaluable help and
support and Paul P. Carbone, Richard R. Love, Bernard Fisher, Sydney
E. Salmon, and Douglass C. Tormey for the clinical application of
many of the concepts and results described here. The EnCalOl tumor
was kindly provided by Dr. P. G. Satyaswaroop, Department of Ob
stetrics and Gynecology, Hershey School of Medicine, Hershey, PA,
for the experiment in Fig. 6 performed by Dr. Marco M. Gottardis and
Michelle Ricchio.
22.
15.
16.
17.
18.
19.
23.
24.
25.
26.
27.
28.
29.
30.
31.
References
1. Beatson, G. T. On the treatment of inoperable cases of carcinoma of the
mamma: suggestions for a new method of treatment with illustrative cases.
Lancet, 2: 104-107, 162-167, 1896.
2. Dao, T. L., and Muggins, C. Bilateral adrenalectomy in the treatment of
cancer of the breast. A. M. A. Arch. Surg., 71: 645-657, 1955.
3. Pearson, O. H., and Ray, B. S. Results of treatment of metastatic mammary
carcinoma. Cancer (Phila.), 12: 85-92, 1959.
4. Allen, E., and Doisy, E. A. The induction of a sexual mature condition in
immature females by injection of the ovarian follicular hormone. Am. J.
Physiol., 69: 577-588, 1924.
5. Cook, J. W., Dodds, E. C., and Hewett, C. L. A synthetic oestrus-exciting
compound. Nature (Lond.), 131: 56-57, 1933.
6. Dodds, E. C., Golberg, L., Lawson, W., and Robinson, R. Oestrogenic
activity of certain synthetic compounds. Nature (Lond.), 141: 247-248,
1938.
7. Dodds, E. C., Golberg, L., Lawson, W., and Robinson, R. Oestrogenic
activity of alkalated stilboestrols. Nature (Lond.), ¡42:34, 1938.
8. Robson, J. M., and Schonberg, A. Oestrous reactions, including mating,
produced by triphenylethylene. Nature (Lond.), 140: 196, 1937.
9. Robson, J. M., and Schonberg, A. A new synthetic estrogen with prolonged
action when given orally. Nature (Lond.), 150: 22-23, 1942.
10. Thompson, C. R., and Werner, H. W. Studies on estrogen tri-p-anisylchloroethylene. Proc. Soc. Exp. Biol. Med., 77: 494-497, 1951.
11. Shelton, R. S., VanCampen, M. G., Jr., Meisner, D. F., Parmeter, S. M.,
Andrews, E. R., Allen, R. E., and Wyckoff, K. K. Synthetic estrogens.
Halotriphenyl ethylene derivatives. J. Am. Chem. Soc., 75: 5491-5493,
1953.
12. Robson, J. M. Quantitative data on the inhibition of oestrus by testosterone,
progesterone and certain other compounds. J. Physiol., 92: 371-382, 1938.
13. Szego, C. M., and Roberts, S. Pituitary-adrenal antagonism to estrogenic
stimulation of the uterus of the ovariectomized rat. Am. J. Physiol., 152:
131-140, 1948.
14. Velardo, J. T., Hisaw, F. L., and Bever, A. T. Inhibitory action of cortisone
32.
33.
acetate, desoxycorticosterone acetate and testosterone on estradiol-17 in
duced uterine growth. Endocrinology, 59: 165-169, 1956.
Edgren, R. A., and Calhoun, D. W. Estrogen antagonisms: inhibition of
estrone-induced uterine growth by testosterone propionate, progesterone
and 17-ethyl-19-nortestosterone. Proc. Soc. Exp. Biol. Med., 94: 537-539,
1957.
Lerner, L. J., Holthaus, F. J., Jr., and Thompson, C. R. A myotrophic
agent and gonadotrophin inhibitor, 19-nortestosterone-17-benzoate. Endo
crinology, 64: 1010-1016, 1959.
Hisaw, F. L., Velardo, J. T., and Goolsby, C. M. Interaction of estrogens
on uterine growth. J. Clin. Endocrino!., 14: 1134-1143, 1954.
Velardo, J. T., and Sturgis, S. H. Interaction of 16-epi-estriol and estradiol17 on uterine growth. Proc. Soc. Exp. Biol. Med., 90: 609-610, 1955.
Muggins, C., and Jensen, E. V. The depression of estrone-induced uterine
growth by phenolic estrogens with oxygenated functions at position 6 or 16:
the impeded estrogens. J. Exp. Med., 102: 335-346, 1955.
Edgren, R. A., and Calhoun, D. W. Oestrogen antagonisms: the effects of
oestriol and 16-epioestriol on oestrone-induced uterine growth in spayed
rats. J. Endocrinol., 20: 325-330, 1960.
Edgren, R. A., and Calhoun, D. W. Interaction of estrogens on the vaginal
smear of spayed rats. Am. J. Physiol., 189: 355-357, 1957.
Lerner, L. J. Uterotrophic and antiestrogenic activity of a non-steroidal
compound in mice. In: Conference on Comparison of Biological Properties
of Steroids and Hormones, Detroit 1954, Committee on Research, Council
on Pharmacy and Chemistry, American Medical Association, pp. 115-117.
Jensen, E. V., Jacobson, H. I., Flesher, J. W., Saha, N. N., Gupta, G. N.,
Smith, S., Colucci, V., Shiplacoff, D., Neumann, H. G., DeSombre, E. R.,
and Junglut, P. W. Estrogen receptors in target tissues. In: T. Nakao, G.
Pincus, and J. Tait (eds.), Steroid Dynamics, pp. 133-157. New York:
Academic Press, 1966.
Jensen, E. V., Numata, M., Smith, S., Suuki, T., Brecker, P. I., and
DeSombre, E. R. Estrogen-receptor interaction in target tissues. Dev. Biol.,
Suppl. 3, 151-171, 1969.
Lerner, L. J. Estrogen antagonistic activity of l-(/7-2-diethylaminoethoxyphenyl)-l-phenyl-2-/>-anisylethanol (MER-25). Fed. Proc., 17: 388, 1958.
Lerner, L. J., Holthaus, F. J., Jr., and Thompson, C. R. A non-steroidal
estrogen antagonist l-(/)-2-diethylaminoethoxyphenyl)-l-phenyl-2-^-methoxyphenyl ethanol. Endocrinology, 63: 295-318, 1958.
Lerner, L. J. Hormone antagonists: inhibitor of specific activities of estrogen
and androgen. Recent Prog. Horm. Res., 20: 435-490, 1964.
Lerner, L. J. Steroid hormones and uterine growth. Ann. NY Acad. Sci.,
75:460-462, 1959.
Lerner, L. J., Hilf, R., Turkheimer. A. R., Michel, I., and Engel, S. L.
Effects of hormone antagonists on morphological and biochemical changes
induced by hormonal steroids in the rat uterus. Endocrinology, 78: 111124, 1966.
Lerner, L. J., Harris, D. N., Hilf, R., Bianchi, A., and Raskin, B. K.
Responses of the rat uterus and oviduct to sex steroids as influenced by time
and antagonists. In: Proceedings of the Second International Congress on
Hormonal Steroids, Milan, 1966. Excerpta Medica International Congress
Series No. 132, Amsterdam, pp. 628-638. Amsterdam: Excerpta Medica,
1967.
Harris, D. N., Lerner, L. J., and Hilf, R. The effects of progesterone and
ethamoxytriphetol on estradiol-induced changes in the immature rat uterus.
Trans. NY Acad. Sci., 30: 774-782, 1968.
Lerner, L. J., Hilf, R., and Harris, D. N. The effect of antagonists on
androgen- and estrogen-induced changes in the male accessory sex organs
of the rat. Trans. NY Acad. Sci., 30: 783-793, 1968.
Sutherland, R. L., Mester, J., and Baulieu, E. E. Tamoxifen is a potent
"pure" antioestrogen in the chick oviduct. Nature (Lond.), 267: 434-435,
1977.
34. Sutherland, R. L. Estrogen antagonists in chick oviduct: antagonist activity
of eight synthetic triphenylethylene derivatives and their interactions with
cytoplasmic and nuclear estrogen receptors. Endocrinology, 109: 20612068, 1981.
35. Segal, S. J., and Nelson, W. O. An orally active compound with antifertility
effects in rats. Proc. Soc. Exp. Biol. Med., 98: 431-436, 1958.
36. Chang, M. C. Degeneration of ova in the rat and rabbit following oral
administration of l-(p-2-diethylaminoethoxyphenyl)-l-phenyl-2-/j-anisylethanol. Endocrinology, 65: 339-342, 1959.
37. Emmens, C. W. Compounds exhibiting prolonged antiestrogenic and antifertility activity in mice and rats. J. Reprod. Fértil.,26: 175-182, 1971.
38. Clark, E. R., and Jordan, V. C. Oestrogenic, anti-oestrogenic and fertility
properties of a series of compounds related to ethamoxytriphetol (MER25). Br. J. Pharmacol., 57:487-493, 1976.
39. Morris, J. M., VanWagenen, G., McCann, J., and Jacobs, D. Compounds
interfering with ovum implantation and development. II. Synthetic estrogens
and antiestrogens. Fértil.Steril., 18: 18-34, 1967.
40. Kamboj, V. P., Setty, B. S., Chandra, H., Roy, S. K., and Kar, A. B.
Biological profile of centchroman—a new post-coital contraceptive. Ind. J.
Exp. Biol., /5: 1144-1146, 1977.
41. Lerner, L. J. The first non-steroidal antioestrogen-MER-25. In: R. L.
Sutherland and V. C. Jordan (eds.), Non-steroidal antioestrogens: Molecular
Pharmacology and Antitumor Activity, pp. 1-16. Sydney, Australia: Aca
demic Press, 1981.
42. Adams, W. C., France, E. S., and Leathern, J. H. The influence of an
estrogen antagonist on reproductive physiology in the female rat. Proc. Pa.
Acad. Sci., 34: 155-158, 1960.
4186
Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1990 American Association for Cancer Research.
ANTIESTROGENS AND BREAST CANCER
43. Leathern, J. H., and Adams, W. C. Prevention of ovarian cyst formation by
ethamoxytriphetol (MER-25). Proc. Soe. Exp. Biol. Med., 113: 240-242,
1963.
44. Kistner, R. W., and Smith, O. W. Observations on the use of a non-steroidal
estrogen antagonist: Mer-25. Surg. Forum, 10: 725-729, 1960.
45. Kistner, R. W., and Smith, O. W. Observations on the use of a nonsteroidal
estrogen antagonist: Mer-25. II. Effects in endometrial hyperplasia and
Stein-Leventhal syndrome. Fértil.Steril., 12: 121-141, 1961.
46. Tyler, E. T., Olson, H. J., and Gotlib, M. H. The induction of ovulation
with an anti-estrogen. Int. J. Fértil.,5:429-436, 1960.
47. Holtkamp, D. E., Greslin, J. G., Root, C. A., and Lerner, L. J. Gonadotrophin inhibiting and anti-fecudity effects of chloramiphene. Proc. Soc. Exp.
Biol. Med., 705: 197-201, 1960.
48. Greenblatt, R. B., Barfield, W. E., Jungck, E. C., and Ray, A. W. Induction
of ovulation with MRL-41. Preliminary report. JAMA, 178:101-104,1961.
49. Lerner, L. J., Harris, D. N., Yiacas, E., Hilf, R., and Michel, I. Cholesterol
synthesis inhibitor showing reduction of lipids and hormone antagonism.
Am. J. Clin. Nutr., 23: 1241-1250, 1970.
50. Herbst, A. L., Griffiths, C. T., and Kistner, R. W. Clomiphene citrate (NSC35770) in disseminated mammary carcinoma. Cancer Chemother. Rep., 43:
39-41, 1964.
51. Harper, M. J. K., and Walpole, A. L. Contrasting endocrine activities of m
and trans isomers in a series of substituted triphenylethylenes. Nature
(Lond.), 2/2:87, 1966.
52. Harper, M. J. K., and Walpole, A. L. A new derivative of triphenylethylene:
effect on implantation and mode of action in rats. J. Reprod. Fértil.,13:
101-119, 1967.
53. Harper, M. J. K., and Walpole, A. L. Mode of action of ICI 46,474 in
preventing implantation in rats. J. Endocrinol., 37: 83-92, 1967.
54. Labhsetwar, A. P. Role of estrogens in ovulation. A study using the estrogen
antagonist ICI 46,474. Endocrinology, 87: 542-551, 1970.
55. Jordan, V. C., and Robinson, S. P. Species-specific pharmacology of antiestrogens: role of metabolism. Fed. Proc., 46: 1870-1874, 1987.
56. Terenius, L. Structure-activity relationships of anti-oestrogens with regard
to interaction with 17ß-oestradiolin the mouse uterus and vagina. Acta
Endocrinol. Copenh., 66: 431-447, 1971.
57. Jordan, V. C. Prolonged antioestrogenic activity of ICI 46,474 in the
ovariectomized mouse. J. Reprod. Fértil.,52: 251-258, 1975.
58. Jordan, V. C., Lababidi, M. K., and Mirecki, D. M. Inhibition of mouse
mammary tumorigenesis by the antiestrogen tamoxifen. In: Proceedings of
the British Pharmacological Society, King College, London, Abstract 22,
December 1988.
59. Skidmore, J. R., Walpole, A. L., and Woodburn, J. Effect of some triphen
ylethylenes on oestradiol binding in vitro to macromolecules from uterus
and anterior pituitary. J. Endocrinol., 52: 289-298, 1972.
60. Jordan, V. C., and Prestwich, G. Binding of [3H] tamoxifen in rat uterine
cytosols. A comparison of swinging bucket and vertical tube rotor sucrose
density gradient analysis. Mol. Cell. Endocrinol., 8: 179-188, 1977.
61. Jordan, V. C., and Dowse, L. J. Tamoxifen as an antitumour agent: effect
on oestrogen binding. J. Endocrinol., 68: 297-303, 1976.
62. Jordan, V. C., Dix, C. J., Rowsby, L., and Prestwich, G. Studies on the
mechanisms of action of the non-steroidal antioestrogen (ICI 46,474) in the
rat. Mol. Cell. Endocrinol., 7: 177-192, 1977.
63. Jordan, V. C., Rowsby, L., Dix, C. J., and Prestwich, G. Dose-related effect
of non-steroidal antioestrogens and non-steroidal oestrogens on the meas
urement of cytoplasmic oestrogen receptors in the rat and mouse uterus. J.
Endocrinol., 78: 71-81, 1978.
64. Jordan, V. C., and Naylor, K. E. Binding of [3H]oestradiol in the immature
rat uterus during the sequential administration of antioestrogens. Br. J.
Pharmacol., 65: 167-173, 1979.
65. Berthois, Y., Katzenellenbogen, J. A., and Katzenellenbogen, B. S. Phenol
red in tissue culture media is a weak estrogen: implications concerning the
study of estrogen-responsive cells in culture. Proc. Nati. Acad. Sci, USA,
«5:2496-2500, 1986.
66. Bindal, R. D., Carlson, K. E., Katzenellenbogen, B. S., and Katzenellenbo
gen, J. A. Lipophilic impurities, not phenosulfophthalein, account for the
estrogenic activity in commercial preparations of phenol red. J. Steroid
Biochem., 31: 287-293, 1988.
67. Lippman, M. E., and Bolán,G. Oestrogen-responsive human breast cancer
in long-term tissue culture. Nature (Lond.), 256: 592-595, 1975.
68. Reddel, R. R., Murphy, L. C., and Sutherland, R. L. Effects of biologically
active metabolites of tamoxifen on the proliferation kinetics of MCF-7
human breast cancer cells in vitro. Cancer Res., 43: 4618-4614, 1983.
69. Taylor, C. M., Blanchard, B., and Zava, D. T. Estrogen receptor mediated
and cytotoxic effects of the antiestrogens tamoxifen and 4-hydroxytamoxifen. Cancer Res., 44: 1409-1414,1984.
70. Sutherland, R. L., Murphy, L. C., Foo, M. S., Green, M. D., Wybourne, A.
M., and Krozowski, Z. S. High affinity antioestrogen binding site distinct
from the oestrogen receptor. Nature (Lond.), 288: 273-275, 1980.
71. Sutherland, R. L., Green, M. D., Hall, R. E., Reddel, R. R., and Taylor, I.
W. Tamoxifen induces accumulation of MCF-7 human mammary carci
noma cells in the Go/G] phase of the cell cycle. Eur. J. Cancer Clin. OncoL,
19: 615-621, 1983.
72. Osborne, C. K., Boldt, D. H., Clark, G. M., and Trent, J. M. Effect of
tamoxifen on human breast cancer cell cycle kinetics: accumulation of cells
in early G, phase. Cancer Res., 43: 3583-3586, 1983.
73. Bates, S. E., Davidson, N. E., Vilverius, E. M., Fréter,C. E., Dickson, R.
B., Tarn, J. P., Kudlow, J. E., Lippman, M. E., and Salomon, D. S.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
86.
87.
88.
89.
90.
91.
92.
93.
94.
95.
96.
97.
98.
99.
100.
101.
102.
103.
104.
Expression of transforming growth factor a and its messenger ribonucleic
acid in human breast cancer: its regulation by estrogen and its possible
functional significance. Mol. Endocrino!., 2: 543-555, 1988.
Knabbe, C., Lippman, M. E., Wakefield, L. M., Flanders, K. C., Kasid, A.,
Derynck, R., and Dickson, R. B. Evidence that transforming growth factor
ßis a hormonally regulated negative growth factor in human breast cancer
cells. Cell, 48: 417-428, 1987.
Cole, M. P., Jones, C. T. A., and Todd, I. D. H. A new antioestrogenic
agent in late breast cancer: an early clinical appraisal of ICI 46,474, Br. J.
Cancer, 25: 270-275, 1971.
Ward, H. W. C. Antioestrogen therapy for breast cancer: a trial of tamoxifen
at two dose levels. Br. Med. J., /: 13-14, 1973.
O'Halloran, M. J., and Maddock, P. G. ICI 46,474 in breast cancer. J. Ir.
Med. Assoc., 67: 38-39, 1974.
Klopper, A., and Hall, M. New synthetic agent for the induction of ovula
tion. Preliminary trial in women. Br. Med. J., /: 152-154, 1971.
El-Sheikha, Z., Klopper, A., and Beck, J. S. Treatment of menometrorrhagia
with antioestrogen. Clin. Endocrinol., /: 275-282, 1972.
Williamson, J. G., and Ellis, J. D. The induction of ovulation by tamoxifen.
J. Obstet. Gynaecol. Br. Commonw., 80: 844-847, 1973.
Jensen, E. V., Block, G. E., Smith, S., Kyser, K., and DeSombre, E. R.
Estrogen receptors and breast cancer response to adrenalectomy. Nati.
Cancer Inst. Monogr., 34: 55-70, 1971.
Jordan, V. C., and Koerner, S. Tamoxifen (ICI 46,474) and the human
carcinoma 8S estrogen receptor. Eur. J. Cancer, 11: 205-206, 1975.
Jordan, V. C. The development of tamoxifen for breast cancer therapy: a
tribute to the late Arthur L. Walpole. Breast Cancer Res. Treat., 11: 197209, 1988.
Investigational Drug Brochure for ICI 46,474. Clinical Research Depart
ment, ICI Americas Inc., Wilmington, DE, March 1974.
Jordan, V. C. Antitumour activity of the antioestrogen ICI 46,474 (tamox
ifen) in the dimethylbenzanthracene (DMBA)-induced rat mammary carci
noma model. J. Steroid. Biochem., 5: 354, 1974.
Jordan, V. C., Koerner, S., and Robison, C. Inhibition of oestrogen-stimu
lated prolactin release by antioestrogens. J. Endocrinol., 65:151-152,1975.
Jordan, V. C. Effect of tamoxifen (ICI 46,474) on initiation and growth of
DMBA-induced rat mammary carcinomata. Eur. J. Cancer, 12: 419-424,
1976.
Jordan, V. C., and Koerner, S. Tamoxifen as an antitumour agent: role of
oestradiol and prolactin. J. Endocrinol., 68: 305-310, 1976.
Jordan, V. C. The antiestrogen tamoxifen (ICI 46,474) as an antitumor
agent. Proceedings of the Eastern Cooperative Oncology Group, Miami,
FL, February 11-12, 1974.
Jordan, V. C. Tamoxifen: mechanism of antitumor activity in animals and
man. Proceedings of the Eastern Cooperative Oncology Group, Jaspar,
Alberta, Canada, June 22-25, 1974.
Osborne, C. K., Hobbs, K., and Clark, G. M. Effect of estrogens and
antiestrogens on growth of human breast cancer cells in athymic mice.
Cancer Res., 45: 584-590, 1985.
Gottardis, M. M., Robinson, S. P., and Jordan, V. C. Estradiol-stimulated
growth of MCF-7 tumors implanted in athymic mice: a model to study the
tumoristatic action of tamoxifen. J. Steroid. Biochem., 30: 311-314, 1988.
Gottardis, M. M., and Jordan, V. C. Development of tamoxifen-stimulated
growth of MCF-7 tumors in athymic mice after long-term antiestrogen
administration. Cancer Res., 48: 5183-5187, 1988.
Gottardis, M. M., Jiang, S. Y., Jeng, M. H., and Jordan, V. C. Inhibition
of tamoxifen-stimulated growth of an MCF-7 tumor variant in athymic
mice by novel steroidal antiestrogens. Cancer Res., 49:4090-4093, 1989.
Jordan, V. C., Gottardis, M. M., Robinson, S. P., and Friedl, A. Immunedeficient animals to study "hormone-dependent" breast and endometrial
cancer. J. Steroid. Biochem., 34: 169-176, 1989.
Jordan, V. C. The antitumour affect of tamoxifen in the dimethylbenzanthracene-induced mammary carcinoma model. Proceedings of a Symposium
on the Hormonal Control of Breast Cancer, Alderley Park, pp. 11-17.
Macclesfield, United Kingdom: ICI Pharmaceuticals Division PLC, 1975.
Nicholson, R. I., and Golder, M. P. Effect of synthetic antioestrogens on
the growth and biochemistry of rat mammary tumours. Eur. J. Cancer, //:
571-579, 1975.
Jordan, V. C., and Jaspan, T. Tamoxifen as an antitumour agent: oestrogen
binding as a predictive test for tumour response. J. Endocrinol., 68: 453460, 1976.
Jordan, V. C., Dix, C. J., and Allen, K. E. The effectiveness of long-term
treatment in a laboratory model for adjuvant hormone therapy of breast
cancer. In: S. E. Salmon and S. E. Jones (eds.), Adjuvant Therapy for Cancer
II, pp. 19-26. New York: Gruñeand Stratton, 1979.
Jordan, V. C., and Allen, K. E. Evaluation of the antitumor activity of the
nonsteroidal antioestrogen monohydroxytamoxifen in the DMBA-induced
rat mammary carcinoma model. Eur. J. Cancer, 16: 239-251, 1980.
Jordan, V. C. Use of the DMBA-induced rat mammary carcinoma system
for the evaluation of tamoxifen treatment as a potential adjuvant therapy.
Rev. Endocrinol. Rei. Cancer, October Suppl., 49-55, 1978.
Jordan, V. C., Allen, K. E., and Dix, C. J. The pharmacology of tamoxifen
in laboratory animals. Cancer Treat. Rep., 64: 745-759, 1980.
Robinson, S. P., and Jordan, V. C. Reversal of the antitumor effect of
tamoxifen by progesterone in the 7,12-dimethylbenzanthracene-induced
rat
mammary carcinoma model. Cancer Res., 47: 5386-5390, 1987.
Robinson, S. P., Mauel, D. A., and Jordan, V. C. Antitumor actions of
toremifene in the 7,12-dimethylbenzanthracene (DMBA)-induced rat mam-
4187
Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1990 American Association for Cancer Research.
ANTIESTROGENS AND BREAST CANCER
mary tumor model. Eur. J. Cancer Clin. Oncol., 24: 1817-1821, 1988.
105. Wilson, A. J., Tehrani, F., and Baum, M. Adjuvant tamoxifen therapy for
early breast cancer: an experimental study with reference to oestrogen and
progesterone receptors. Br. J. Surg., 69: 121-125, 1982.
106. Gottardis, M. M, and Jordan, V. C. The antitumor actions of keoxifene
and tamoxifen in the A'-nitrosomethylurea-induced rat mammary carcinoma
model. Cancer Res., 47: 4020-4024, 1987.
107. Early Breast Cancer Trialists' Collaborative Group. Effect of adjuvant
tamoxifen and of cytotoxic therapy on mortality in early breast cancer. N.
Engl. J. Med., 319: 1681-1692, 1988.
108. Tormey, D. C., and Jordan, V. C. Long-term tamoxifen adjuvant therapy
in node positive breast cancer: a metabolic and pilot clinical study. Breast
Cancer Res. Treat., 4: 297-302, 1984.
109. Falkson, H. C., Gray, R., and Wolberg, W. M. Adjuvant therapy of postmenopausa! women with breast cancer—an ECOG phase III study. Abstract
67. Proc. ASCO San Francisco May, 1989.
110. Fisher, B., Redmond, C., Brown, A., Fisher, E. R., Wolmark, N., Bowman,
D., Plotkin, D., Wolter, J., Bornstein, R., Legault-Poisson, S., Saffer, E.
A., and Other NSABP Investigators. Adjuvant chemotherapy with and
without tamoxifen in the treatment of primary breast cancer: 5 year results
from the National Surgical Adjuvant Breast and Bowel Project Trial. J.
Clin. Oncol., 4: 459-471, 1986.
111. Fisher, B., Brown, A., Wolmark, N., Redmond, C, Wickerham, L., Wittliff,
J., Dimitrov, N., Legault-Poisson, S., Schipper, H., Prager, D., and Other
NSABP Investigators. Prolonging tamoxifen therapy for primary breast
cancer. Ann. Intern. Med., ¡06:649-654, 1987.
112. Delozier, T., Julien, J-P., Juret, P., Veyret, C., Couette, J-E., Grai, Y.,
Olliver, J-.M.. and de Ranier, E. Adjuvant tamoxifen in postmenopausal
breast cancer: preliminary results of a randomized trial. Breast Cancer Res.
Treat., 7: 105-110, 1986.
113. Breast Cancer Trials Committee, Scottish Cancer Trials Office (MRC).
Adjuvant tamoxifen in the management of operable breast cancer: the
Scottish Trial. Lancet, 2: 171-175, 1987.
114. Fisher, B., Constantino, J., Redmond, C., and Other Members of the
NSABP. A randomized clinical trial evaluating tamoxifen in the treatment
of patients with node-negative breast cancer who have estrogen receptorpositive tumors. N. Engl. J. Med., 320: 479-484, 1989.
115. Fromson, J. M., Pearson, S., and Bramali. S. The metabolism of tamoxifen
(ICI 46,474) Part II in female patients. Xenobiotica, 3: 711-713, 1973.
116. Fabian, C., Sternson, L., and Barrett, M. Clinical pharmacology of tamoxifen in patients with breast cancer: comparison of traditional and loading
dose schedules. Cancer Treat. Rep., 64: 765-773, 1980.
117. Adam, H. K., Gay, M. A., and Moore, R. H. Measurement of tamoxifen in
serum by thin layer densitometry. J. Endocrinol., 84: 35-42, 1982.
118. Daniel, C. P., Gaskell, S. J., Bishop, H., and Nicholson, R. I. Determination
of tamoxifen and a hydroxylated metabolite in plasma from patients with
advanced breast cancer using gas chromatography-mass spectrometry. J.
Endocrinol., 83: 401 -408, 1979.
119. Bratherton, D. G., Brown, C. H., Buchanan, R., Hall, V., Kinglsey Pillers,
E. M., Wheeler, T. K., and Williams, C. J. A comparison of two doses of
tamoxifen (Nolvadex) in postmenopausal women with advanced breast
cancer: 10 mg bd versus 20 mg bd. Br. J. Cancer, 50: 199-205, 1984.
120. Patterson, J. S., Settatree, R. S., Adam, H. K., and Kemp, J. V. Serum
concentrations of tamoxifen and major metabolites during long-term Nol
vadex therapy, correlated with clinical response. In: H. T. Mouridsen and
T. Palshoff (eds.). Breast Cancer—Experimental and Clinical Aspects, pp.
89-92. Oxford, United Kingdom: Pergamon Press, 1980.
121. Furr, B. J. A., and Jordan, V. C. The pharmacology and clinical uses of
tamoxifen. Pharmacol. Ther., 25: 127-205, 1984.
122. Robinson, S. P., and Jordan, V. C. The metabolism of steroid modifying
anticancer agents. Pharmacol. Ther., 36: 41-103, 1988.
123. Jordan, V. C., Bain, R. R., Brown, R. R., Gosden, B., and Santos, M. A.
Determination and pharmacology of a new hydroxylated metabolite of
tamoxifen observed in patient sera during therapy for advanced breast
cancer. Cancer Res., 43: 1446-1450, 1983.
124. Kemp, J. V., Adam, H. K., Wakeling, A. E., and Slater, R. Identification
and biological activity of tamoxifen metabolites in human serum. Biochem.
Pharmacol., 32: 2045-2052, 1983.
125. Jordan, V. C., Collins, M. M., Rowsby, L., and Prestwich, G. A monohydroxylated metabolite of tamoxifen with potent antioestrogenic activity. J.
Endocrinol., 75: 305-316, 1977.
126. Lein, E. A., Solheim, E., Kvinnsland, S., and Veland, P. M. Identification
of 4-hydroxy W-desmethyltamoxifen as a metabolite of tamoxifen in human
bile. Cancer Res., 48: 2304-2308, 1988.
127. Robinson, S. P., Langan-Fahey, S. M., and Jordan, V. C. Implications of
tamoxifen metabolism in the athymic mouse for the study of antitumor
effects upon human breast cancer xenografts. Eur. J. Cancer Clin. Oncol.,
25: 1769-1776, 1989.
128. Jordan, V. C., Phelps, E., and Lingren, J. U. Effects of antiestrogens on
bone in castrated and intact female rats. Breast Cancer Res. Treat., 10: 3135, 1987.
129. Turner, R. T., Wakely, G. K., Hannon, K. S., and Bell, N. H. Tamoxifen
prevents the skeletal effects of ovarian deficiency in rats. J. Bone Miner.
Res., 2:449-456, 1987.
130. Love, R. R., Mazess, R. B., Tormey, D. C., Barden, H. S., Newcomb, P.
A., and Jordan, V. C. Bone mineral density in women with breast cancer
treated for at least two years with tamoxifen. Breast Cancer Res. Treat., 12:
297-301, 1988.
131. Türken,S., Siris, E., Seidin, E., Seidin, D., Plaster, E., Hyman, G., and
Lindsay, R. Effects of tamoxifen on spinal bone density in women with
breast cancer. J. Nati. Cancer Inst., */: 1086-1088, 1989.
132. Bertelli, G., Pronzoto, P., and Amoroso, D. Adjuvant tamoxifen in primary
breast cancer: influence on plasma lipids and antithrombin III. Breast Cancer
Res. Treat., 12: 307-310, 1988.
133. Love, R. R., Newcomb, P. A., Wiebe, D. A., Surawicz, T. S., Jordan, V. C.,
Carbone, P. P., and DeMets, D. C. Lipids and lipoprotein effects of
tamoxifen therapy in postmenopausal women with node negative breast
cancer. Breast Cancer Res. Treat., 13: Abstract 204, 1989.
134. Jordan, V. C., Fritz, N. F., and Tormey, D. C. Long-term adjuvant therapy
with tamoxifen effects on sex hormone binding globulin and antithrombin
III. Cancer Res., 47: 4517-4519, 1987.
135. Swenerton, K. D. Treatment of advanced endometrial adenocarcinoma with
tamoxifen. Cancer Treat. Rep., 64: 805-811, 1980.
136. Killackey, M. A., Hakes, T. B., and Pierce, V. K. Endometrial adenocarci
noma in breast cancer patients receiving tamoxifen. Cancer Treat. Rep., 69:
237-238, 1985.
137. Satyaswaroop, P. G., Zaino, R. J., and Mortel, R. Estrogen-like effects of
tamoxifen on human endometrial carcinoma transplanted into nude mice.
Cancer Res., 44: 4006-4010, 1984.
138. Gottardis, M. M., Robinson, S. P., Satyaswaroop, P. G., and Jordan, V. C.
Contrasting actions of tamoxifen on endometrial and breast tumor growth
in the athymic mouse. Cancer Res., 48: 812-815, 1988.
139. Fornander, T., Rutquist, L. E., Cedermark, B., Glas, U., Mattson, A.,
Siljversward, J. D., Skoog, L., Somell, A., Theve, T., Wilking, N., Askergren, J., and Hjolmar, M. L. Adjuvant tamoxifen in early breast cancer:
occurrence of new primary cancers. Lancet, 1: 117-120, 1989.
140. Groom, G. V., and Griffiths, K. Effect of the antioestrogen tamoxifen on
plasma levels of luteinizing hormone, follicle-stimulating hormone, prolactin, oestradiol and progesterone in normal premenopausal women. J. En
docrinol., 70:421-428, 1976.
141. Jordan, V. C., Fritz, N. F., and Tormey, D. C. Endocrine effects of adjuvant
chemotherapy and long-term tamoxifen administration on node positive
patients with breast cancer. Cancer Res., 47: 624-630, 1987.
142. Ravdin, P. M., Fritz, N. F., Tormey, D. C., and Jordan, V. C. Endocrine
status of premenopausal node positive breast cancer patients following
adjuvant chemotherapy and long-term tamoxifen. Cancer Res., 48: 10261029, 1988.
143. Korenman, S. G. Relation between estrogen inhibiting activity and binding
to cytosol of rabbit and human uterus. Endocrinology, 87:1119-1123,1970.
144. Bouton, M. M., and Raynaud, J. P. The relevance of interaction kinetics in
determining biological response to estrogens. Endocrinology, 705:509-575,
1979.
145. Jordan, V. C., Dix, C. J., Naylor, K. E., Prestwich, G., and Rowsby, L.
Nonsteroidal antiestrogens: their biological effects and potential mecha
nisms of action. J. Toxicol. Environ. Health, 4: 364-390, 1978.
146. Binan. N., Catelli, M. H., Geynet, Puri, V., Hahnel, R., Mester, J., and
Baulieu, E. E. Monohydroxytamoxifen: an antiestrogen with high affinity
for the chick oviduct oestrogen receptor. Biochem. Biophys. Res. Commun.,
91: 812-818, 1979.
147. Borgna, J. L., and Rochefort, H. High affinity binding to the estrogen
receptor of [3H] 4-hydroxytamoxifen, an active antiestrogen metabolite.
Mol. Cell. Endocrinol., 20: 71-85, 1980.
148. Rochefort, H., and Borgna, J. L. Differences between oestrogen receptor
activated by oestrogen and antioestrogen. Nature (Lond.), 292: 257-259,
1981.
149. Jordan, V. C., and Bowser-Finn, R. A. Binding of [3H] monohydroxytamoxifen by immature rat tissues in vivo. Endocrinology, 110: 1281-1291,
1982.
150. Tate, A. C., Greene, G. L., DeSombre, E. R., Jensen, E. V., and Jordan, V.
C. Differences between estrogen and antiestrogen-estrogen receptor com
plexes from human breast tumors identified with an antibody raised against
the estrogen receptor. Cancer Res., 44: 1012-1018, 1984.
151. Lieberman, M. E., Gorski, J., and Jordan, V. C. An estrogen receptor model
to describe the regulation of prolactin synthesis by antiestrogens in vitro. J.
Biol. Chem., 258: 4741-4745, 1983.
152. Jordan, V. C., Lieberman, M. E., Cormier, E., Bagely, J., and Ruenitz, P.
Structural requirements for the pharmacological activity of non-steroidal
antiestrogens in vitro. Mol. Pharmacol., 26: 272-278, 1984.
153. Jordan, V. C., and Lieberman, M. E. Estrogen-stimulated prolactin synthe
sis /'/; vitro: classification of agonist, partial agonist and antagonist actions
based on structure. Mol. Pharmacol., 26: 279-285, 1984.
154. Jordan, V. C., Koch, R., Mittal, S., and Schneider, M. R. Oestrogenic and
antioestrogenic actions in a series of triphenylbut-1-enes: modulation of
prolactin synthesis in vitro. Br. J. Pharmacol., 87: 217-220, 1986.
155. Jordan, V. C., Koch, R., Langan, S., and McCague, R. Ligand interaction
at the estrogen receptor to program antiestrogen action: a study with
nonsteroidal compounds in vitro. Endocrinology, 122: 1449-1454, 1988.
156. Bignon, E., Pons, M., Crastes de Paulet, A., Dore, J. C., Gilbert, J.,
Abecassis, J., Miquel, J. F., Ojasoo, T., and Raynaud, J. P. Effect of
triphenylacrylonitrile derivatives on estradiol-receptor binding and on hu
man breast cancer cell growth. J. Med. Chem., 32: 2092-2103, 1989.
157. Murphy, C. S., and Jordan, V. C. Structural components necessary for the
antiestrogenic activity of tamoxifen. J. Steroid Biochem., 34: 407-411,
1989.
158. Jordan, V. C. Biochemical pharmacology of antiestrogen action. Pharmacol.
Rev., 36: 245-276, 1984.
4188
Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1990 American Association for Cancer Research.
ANTIESTROGENS AND BREAST CANCER
159. Wakeling, A. E., and Bowler, J. Steroidal pure antioestrogens. J. Endocrinoi //2-R7-R10
1987
160. Cormier, E. M., and Jordan, V. C. Contrasting ability of antiestrogens to
inhibit MCF-7 growth stimulated by estradiol or epidermal growth factor.
,?-,•r.
ir 57-63,
t--, f-, ,oon
Eur. J., ^Cancer Clin.
Oncol.,i 25:
1989.
161. Jordan, V. C., and Koch, R. Regulation of prolactin synthesis in vitro by
estrogenic and antiestrogemc derivatives of estradici and estrone. Endocrinology, 124: 1717-1726, 1989.
162. Robinson, S. P., and Jordan, V. C. The paracrine stimulation of MCF-7
cells by MDA-MB-231 cells: possible role in antiestrogen failure. Eur. J.
Cancer Clin. Oncol., 25:493-497, 1989.
'63. Jordan, V. C. Chemosuppression of breast cancer with tamoxifen: laboratoI7 evidence and future clinical investigations. Cancer Invest., 6: 5-11,
Ì?••'
i
, •
-•<•,
,
,,
164. ¿.
Cuzik,
and Baum, M. Tamoxifen and contralateral breast cancer. Lancet,
282 J.,
1985
,65 Powle's T ¿ Hardy j R Ash,ey s E Farringtoni G. H., Cosgrove, D.,
Davey, J. B., Dowsett, M., McKinna, J. A., Wash, A. G., Sinnett, H. p.,
Tillyer, C. R., and Treleaven, J. G. A pilot trial to evaluate the acute toxicity
and feasibility of tamoxifen for prevention of breast cancer. Br. J. Cancer,
60: 126-131, 1989.
4189
Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1990 American Association for Cancer Research.
Development of Antiestrogens and Their Use in Breast Cancer:
Eighth Cain Memorial Award Lecture
Leonard J. Lerner and V. Craig Jordan
Cancer Res 1990;50:4177-4189.
Updated version
E-mail alerts
Reprints and
Subscriptions
Permissions
Access the most recent version of this article at:
http://cancerres.aacrjournals.org/content/50/14/4177
Sign up to receive free email-alerts related to this article or journal.
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Department at [email protected].
To request permission to re-use all or part of this article, contact the AACR Publications
Department at [email protected].
Downloaded from cancerres.aacrjournals.org on April 28, 2017. © 1990 American Association for Cancer Research.