Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
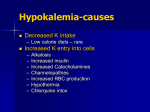
Nephrology Dialysis Transplantation 29 (Supplement 3): iii69–iii72, 2014 doi:10.1093/ndt/gfu140 CELL PHYSIOLOGY AND ELECTROLYTES SP001 OPTIMIZING THE ZS-9 POTASSIUM ION TRAP: PORE SIZE AND THERMODYNAMICS Alex Yang1, John J. Low2, Alejandro Leon3 and Henrik S. Rasmussen3 1 Xelay Acumen, Belmont, CA, 2Consultant, Schaumburg, IL, 3ZS Pharma, Inc., Coppell, TX Introduction and Aims: Physiologic ion channels take advantage of the different ionic diameters to selectively filter the requisite ion. For example, although potassium (K+) and sodium (Na+) ions are similar in size (3.0 Å and 2.3 Å, respectively [Volkov 1997]), K+ channels discriminate between K+ and Na+ by a factor of 10,000 (Doyle 1998) using a selectivity filter. To pass through the selectivity filter, an ion must first shed its coat of water and interact with the carbonyl oxygens. Although the K+ channel filter can accommodate both K+ and Na+ ions, only K+ ions are large enough to interact with the carbonyl oxygens after dehydration. Zirconium silicates have been known to extract ammonium ions from streams (Bem 1999). Since ammonium and K+ cations have similar radii, it suggests that zirconium silicates may be effective in capturing K+. An optimization process was undertaken to find a zirconium silicate drug candidate to capture K+ cations in a specific manner. Several lattice structures of zirconium silicates were tested to find one that mimicked the action of physiologic K+ channels. The result of this optimization process was ZS-9, a material designed and engineered to preferentially entrap K+ ions after oral administration. Results from a structural study to determine the pore size of ZS-9 and thermodynamic stability modeling for various cations (Na+, K+, calcium [Ca2+], and magnesium [Mg2+]) within the ZS-9 lattice structure are reported here. Methods: In the structural study, ZS-9 was dried and ground in an agate mortar, then placed into a powder diffractometer. Data were collected at room temperature with monochromated Cu α1 radiation (λ=1.5406 Å). Rietveld least squares structural refinements were performed, and the interatomic distances were calculated from the resulting atom positions. The size of the pore opening was calculated by subtracting twice the atomic radius of oxygen (van der Waals radius, r=1.52 Å) from center-center interatomic distances. For the thermodynamic stability modeling, the predicted energies for different cation forms of ZS-9 (ie, Na-ZS-9, K-ZS-9, Ca-ZS-9 and Mg-ZS-9) and alkali and alkaline earth oxides from models were used to estimate the cation exchange energies in ZS-9. All energies were computed relative to the Na+ form of ZS-9, defined as the reference state. Results: The structure of ZS-9 consists of units of octahedrally and tetrahedrally coordinated zirconium and silicon atoms with oxygen atoms acting as bridges between the units, forming an ordered cubic lattice structure. The framework is negatively charged due to the octahedral [ZrO6]-2 units. The pore opening of ZS-9 is composed of an asymmetrical seven-member ring (Figure) with an average size of ~3 Å. Thermodynamically, ZS-9 with K+ was calculated to be more stable than ZS-9 with Na+, Ca2+, or Mg2+. For example, the K+ form of ZS-9 was 20 kcal/mol more stable than the Na+ form. Conclusions: The diameter of the unhydrated K+ ion is similar to that of the ZS-9 pore opening, indicating the K+ cations can fit within the lattice structure of ZS-9 after they shed their hydration shell, which confers ZS-9 high specificity for K+ ions. This SP001 hypothesized mechanism of action is supported by results from the thermodynamic study, which demonstrates the selectivity of ZS-9 for K+ over other ions. SP002 EFFECT OF VASOPRESSIN ANTAGONISM ON RENAL HANDLING OF SODIUM AND WATER AND CENTRAL AND BRACHIAL BLOOD PRESSURE DURING INHIBITION OF THE NITRIC OXIDE SYSTEM IN HEALTHY SUBJECTS Safa Al Therwani1 University Clinic In Nephrology and Hypertension and Aarhus University, Holstebro, Denmark 1 Introduction and Aims: Tolvaptan is a selective vasopressin receptor antagonist (V2R) that increases free water excretion. We wanted to test the hypotheses that tolvaptan changes both renal handling of water and sodium and systemic hemodynamics during basal conditions and during nitric oxide (NO)-inhibition with L-NG-monomethyl-arginine (L-NMMA). Methods: Nineteen healthy subjects were enrolled in a randomized, placebo-controlled, double-blind, crossover study of two examination days. Tolvaptan 15 mg or placebo was given in the morning . L-NMMA was given as a bolus followed by continuous infusion during 60 minutes. We measured urine output(OU), free water clearance (CH2O), fractional excretion of sodium (FENa), urinary aquaporin-2 channels (u-AQP2) and epithelial sodium channels (u-ENaCγ), plasma vasopressin ( p-AVP), central and brachial blood pressure(cBP, bBP). Results: During baseline conditions, tolvaptan caused a significant increase in UO, CH2O and p-AVP, and FENa was unchanged. During L-NMMA infusion, UO and CH2O decreased more pronounced after tolvaptan than after placebo (-54 vs.-42% and -34 vs.-9% respectively). U-AQP2 decreased during both treatments, whereas u-ENaCγ decreased after placebo and increased after tolvaptan. CBP and bBP were unchanged. Conclusions: During baseline conditions, tolvaptan increased renal water excretion. During NO-inhibition, the more pronounced reduction in renal water excretion after tolvaptan indicates that NO promotes water excretion in the principal cells, at least partly, via an AVP-dependent mechanism. The lack of decrease in u-AQP2 by tolvaptan could be explained by a counteracting effect of increased plasma vasopressin. The antagonizing effect of NO-inhibition on u-ENaC suggests that NO interferes with the transport via ENaC by an AVP-dependent mechanism. SP003 THE HIDDEN MESSAGE OF URINE: IN-DEPTH CHARACTERIZATION OF THE HEALTHY URINARY PROTEOME Maurizio Bruschi1, Laura Santucci1, Marco Bonsano1, Giovanni Candiano1, Gian Marco Ghiggeri1 and Enrico Verrina1 1 Istituto Giannina Gaslini, Genova, Italy Introduction and Aims: Urine is a biological fluid resulting from the filtration of blood, is in close proximity to several organs and tissues, and its collection is non invasive and readily available. In this context, this body fluid has historically represented a particularly interesting source of kidney disease biomarkers.However, as in the case of other biological fluids, one of the main analytical challenges in the characterization of urinary proteome is the very wide concentration range of proteins, largely exceeding the dynamic range of current analytical approaches. Methods: Here, we described an extensive sub-fractionation method to investigate the characterization of the healthy urinary proteome. After the collection, urine samples are centrifuged to remove cells and debris and then are ultra-centrifuged in order to pellet the micro-vesicles. The supernatant is treated with a mixture of organic solvents to pellet the highly hydrophobic proteins and remove the interference of pigments. This supernatant is dialysed and loaded on Combinatorial Peptides Ligand Library (CPLL) to reduce the dynamic range of protein concentration in urine and at the same time unmask previously undetected proteins. Finally, each urinary fraction is processed using two-dimensional electrophoresis and mass spectrometry techniques, and the qualitative and quantitative data are analyzed using the hierarchical clustering analysis. Results: The combined use of this proteomic approach has allowed us to create a “complete” virtual map of the healthy urinary proteome, identifying a total of 3429 proteins. In addition, the particular chemical and physical characteristics of this sub-fractionation method allowed to highlight: 744 proteins in micro-vesicles, 85 proteins in the extraction with organic solvents, and 695 proteins in CPLL, all unique to each fraction. Conclusions: These proteins may represent new potential biomarkers of organ function and/or disease. © The Author 2014. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved. Abstracts Nephrology Dialysis Transplantation The next step of this study will consist in applying this sub-fractionation method to the characterization of urinary proteome of patients affected by different kidney diseases in order to identify new disease biomarkers of potential diagnostic and prognostic value. SP004 ACQUIRED BARTTER SYNDROME DUE TO STREPTOMYCIN Shankar Prasad Nagaraju1, Dilip Ashok Kirpalani2, Gaurav Daga2, Hardik Shah2, Aditya S Bhabhe2 and Ashok L Kirpalani2 1 Kasturba Medical College, Manipal University, Manipal, India, 2Bombay Hospital and Medical Research Centre, Mumbai, India specificity was 39%. The positive predictive value (PPV) and negative predictive value (NPV) were 42% and 96%, respectively (Table 1). The sensitivity of SID for metabolic alkalosis was 45% and specificity was 56%. The PPV and NPV were 89% and 69%, respectively (Table 2). Conclusions: Finally, [SID] and [HCO3-] centered models investigated with respect to their consistency with each other in this study. It seems that SID values of less than 38 mmol/L is not reliable for detecting metabolic acidosis, based upon PPV. However, SID values of more than 40 mmol/L may be used for diagnosing metabolic alkalosis cases, considering PPV obtained in the study. SP005 Introduction and Aims: Bartter syndrome is an autosomal recessive renal tubular disorder characterized by hypokalemia, metabolic alkalosis, hypocalcaemia, hypomagnesaemia and hypercalciuria. Pseudo- Bartters/acquired Bartters syndrome has been commonly reported with diuretic abuse and laxative abuse. Among aminoglycosides, it has been described with gentamycin in few case reports. We report a case with similar conglomeration of electrolyte imbalance, but in an unusual setting with streptomycin. Methods: Case report Results: A 74 year old lady who is a known case of diabetes mellitus, hypertension, and hypothyroidism was recently found to have tubercular pleural effusion. She was started on antituberculous treatment which included streptomycin. Two weeks later, she developed convulsions and involuntary movements. On evaluation, she had hypokalemia, hypomagnesemia, hypocalcemia and metabolic alkalosis which persisted even after replacement therapy(Table 1). Urine analysis showed TTKG > 20 and 24 hour urine analysis confirmed the loss of potassium, magnesium and calcium in urine.After discontinuing streptomycin, she showed marked recovery over a week in her electrolyte abnormalities and alkalosis(Table 2). Conclusions: Ours is a rare case report of renal electrolyte wasting that mimicked Bartter syndrome and was induced by streptomycin.Thus while using aminoglycosides it should be kept in mind that they not only cause acute kidney injury but also can cause serious electrolyte disturbances in the form of pseudobartter’s syndrome. SP005 SENSITIVITY AND SPECIFICITY OF STRONG ION DIFFERENCE IN DETECTING METABOLIC ACIDOSIS AND ALKALOSIS CASES DETERMINED BY BICARBONATE BASED MODEL SP005 Hakan Sarlak1, Fatih Bulucu1, Muharrem Akhan1, Seref Demirbas1, Mustafa Cakar2 and Levent Yamanel1 1 Gulhane Military Medical Academy, Ankara, Turkey, 2Eskisehir Military Hospital, Eskisehir, Turkey Introduction and Aims: The Strong Ion Difference (SID) is the difference between the sums of concentrations of the strong cations and strong ions ([SID] = [Na+] + [K +] + [Ca+2] + [Mg+2] - [Cl-] - [Other Strong Anions]). With normal protein levels, [SID] is about 38-40 mmol/L. The traditional approach to acid-base balance is based on bicarbonate [HCO3-] levels. In this study, we aimed to investigate the sensitivity and specificity of SID in detecting metabolic acidosis and alkalosis cases diagnosed by traditional model. Methods: A total of 493 blood gas measurements included into the study. The measurements were obtained retrospectively from subjects monitored in intensive care unit and internal medicine clinics. If the SID < 38 mmol/L and SID > 40 mmol/L were considered as metabolic acidosis and alkalosis, respectively. Results: Hundred fifty-six of the measurements were metabolic acidosis and 218 metabolic alkalosis. The sensitivity of SID for metabolic acidosis was 96% and SP004 Table 1. Persistent electrolyte disturbances on streptomycin Metabolic parameters Na+(m eq/L) K+(m eq/L) Cl-(m eq/L) HCO3-(m eq/L) Ca++( mg/dl) PO4( mg/dl) Mg++( mg/dl) Day 1 138 2.1 88 38 5 0.8 0.3 Day 2 131 2.9 93 35 5.3 0.7 0.5 Day 3 134 3.1 96 32 6.3 1 1 Day 4 137 2.6 100 33 6.04 1.2 1 Day 5 142 3.4 106 33 5.7 1 1.2 Day 6 140 2.7 109 34 4.5 1 1.3 Day 7 142 2.9 106 38 5.1 1.2 1.1 SP006 ACID-BACE DISORDER AFTER ORTHOTOPIC BLADDER REPLACEMENT: ILEAL NEOBALDDER COMPARED WITH ILEAL CONDUIT Younhg-Ki Lee1, Seung Min Lee1, Ajin Cho1, Jwa-Kyung Kim1, Myung-Jin Choi1, Dong-Ho Shin1, Jong-Woo Yoon1, Ja-Ryong Koo1, Hyung Jik Kim1, Jung-Woo Noh1 and Young Goo Lee1 1 Hallym University College of Medicine, Seoul, Republic of Korea Introduction and Aims: Radical cystectomy with urinary tract reconstruction is the standard treatment for invasive bladder cancer. Several investigators have reported the frequent incidence of normal anion gap metabolic acidosis and electrolyte disturbance in those patients. We analyzed the pattern of metabolic acidosis and hypokalemia in SP004 Table 2. Improvement of electrolyte disturbances after stopping Streptomycin Metabolic parameter Na+(meq/L) K+(meq/L) Cl- (meq/L) HCO3-(meq/L) Ca++(mg/dl) PO4(mg/dl) Mg++ (mg/dl) iii | Abstracts Day 8 137 2.5 102 39 4.3 1.6 1.1 Day9 144 2.7 101 46 5.6 1.7 1 Day 10 143 3.6 103 33 7.1 3 1.6 Day 11 139 3.3 102 34 7.8 3.3 1.8 Day 12 134 4 100 28 7.7 3.6 1.9 Day 13 135 4 98 25 7.2 3.2 2 Day14 137 3.7 102 26 7.3 4 2 Volume 29 | Supplement 3 | May 2014 Abstracts Nephrology Dialysis Transplantation patients following the construction of an ileal neobladder compared with ileal conduit method, and searched for the risk factors affecting metabolic acidosis. Methods: Sixty-seven patients who underwent radical cystectomy and urinary diversions for invasive bladder cancer were analyzed. Patients with any illness such as severe pulmonary disorder or taking any medication that could lead to metabolic acidosis were excluded. Acid-base balance, serum electrolytes, renal function and effects of renal function on acid-base metabolism were compared in patients with ileal neobladder and ileal conduit. Results: The urinary diversions were performed using ileal neobladder for 41 patients or ileal conduit for 26 patients. No significant differences were observed in their baseline characteristics and preoperative variables examined between the ileal neobladder and ileal conduit groups, except for age. Metabolic acidosis was detected in 16 patients (39.0%) with ileal neobladder and in 6 patients (23.1%) with ileal conduit. Metabolic acidosis with normal anion gap occurred more often in ileal neobladder group (9 patients, 22.0%) than ileal conduit group (1 patient, 3.8%), however the differences were not statistically significant. The close association between the serum creatinine level and total CO2 (P<0.01, r=-0.249) were demonstrated. Acute kidney injury and all-cause mortality were frequent in patients with metabolic acidosis, especially ileal neobladder group. Postoperative hypokalemia in both groups showed no differences in statistically significance. Conclusions: Patients with ileal neobladder tended to develop metabolic acidosis with normal anion gap more frequently than those with ileal conduit, but there was no statistical significance. The degree of metabolic acidosis was closely associated with the renal function. SP007 SP007 Figure 2: Rapidly normalized serum Na despite fluid liberalization and a single oral dose of 15 mg Tolvaptan. SEVERE SYMPTOMATIC ACUTE HYPONATREMIA IN TRAUMATIC BRAIN INJURY RESPONDS VERY RAPIDLY TO A SINGLE 15 MG DOSE OF ORAL TOLVAPTAN: A MAYO CLINIC HEALTH SYSTEM HOSPITAL EXPERIENCE - NEED FOR CAUTION WITH TOLVAPTAN IN YOUNGER PATIENTS WITH PRESERVED RENAL FUNCTION Macaulay Onuigbo1 and Nneoma Agbasi2 1 Mayo Clinic, Rochester, MN, USA & Mayo Clinic Health System, Eau Claire, WI, USA, Eau Claire, WI, 2North East London NHS Foundation Trust, United Kingdom, London, United Kingdom Introduction and Aims: Hyponatremia is common and affects up to 30% of hospitalized patients. In traumatic brain injury, it results from either SIADH or from cerebral salt wasting. Tolvaptan is now well established as a potent pharmaceutical agent to treat symptomatic hyponatremia from SIADH. Over rapid correction is dangerous. We describe the dramatic correction of serum Na by 18 mEq/L over 18 hours after a single 15 mg dose in a young man with normal kidney function (eGFR of 126). Methods: Case report. Results: A 32-year old Caucasian male was admitted to the Trauma Service after a motor vehicle accident. He had altered level of consciousness, acute right posterior 11th and 12th rib fractures, large scalp hematoma, and a small subarachnoid hemorrhage. His serum Na quickly fell from 141 mEq/dL to 121 mEq/dL over several days. despite corrective measures (Figure 1). Nephrology was consulted. Symptoms included blurred vision, poor memory and cognitive impairment. Tolvaptan 15 mg single dose was administered. Fluid intake was liberalized. Soon after, he noticed increased urination, increased thirst and he was soon drinking “tons of water”. Serum Na rapidly increased to 139 mEq/dL over 18 hours (Figure 2). His urine output more than quintrupled (Figure 3). AVP level was 1.4 pg/mL, consistent with SIADH. Two days later, the symptoms had fully resolved. At post-hospitalization, serum Na was 139 mEq/dL (Figure 4). Conclusions: Previous studies on Tolvaptan recruited older patients, 64-67 years, with some renal impairment. Tolvaptan doses were 30 mg daily dose or higher. The very rapid correction in our 32-year old male patient, the first such report in the literature, is SP007 Figure 3: Quintrupling of urine output following a single oral dose of 15 mg Tolvaptan. SP007 Figure 4: Normalized serum Na 11 days following a single oral dose of 15 mg Tolvaptan. the result of young age and normal kidney function. We suggest the use of lower doses of Tolvaptan (15 mg or lower) in younger patients with preserved kidney function. SP008 PLASMAPHERESIS IMPROVES THE OUTCOME OF OSMOTIC DEMYELINATING SYNDROME Koike Minako1, Kumon Saeko1, Usui Ryosuke1, Kuzuhara Shinzo1 and Onitsuka Sirou1 1 Japan, Chiba, Japan SP007 Figure 1: Falling Serum Na despite fluid restriction, oral Na tablets and reported infusions of 30% sailing boluses. Volume 29 | Supplement 3 | May 2014 Introduction and Aims: Rapid correction of serum sodium is known to be associated with central pontine myelinolysis(CPM). Currently, there is no standard therapy for CPM other than supportive therapy. Other therapy includes steroid, plasmapheresis and IVIG, but these therapies have not been shown to be particularly effective. doi:10.1093/ndt/gfu140 | iii Abstracts Methods: A 71-year-old woman became lethargic and was admitted to hospital. Blood tests revealed severe hyponatremia(101mEq/l) that was adjusted over three days to 120mEq/l by infusing saline. Then the patient’s consciousness rapidly deteriorated again. Neurological examination disclosed palsy with tetraplegia associated with deep-tendon hyperreflexia. Magnetic resonance imaging(MRI)performed an area of hyperintensity in the central pons on T2-weighted images suggestive of CPM. Results: Six consecutive therapeutic plasmapheresis sessions were started with two to three sessions a week. Significant clinical improvement began after plasmapheresis. Two months later, she became remarkably better, started to speak, and moved her extremities upon request. Conclusions: We successfully treated patients with extensive therapeutic plasmapheresis soon after the diagnostic confirmation of CPM. SP009 URINARY EXCRETION OF AQP2 AND ENAC DURING AMILORIDE AND THIAZIDE TREATMENT IN HEALTHY HUMANS. A RANDOMIZED, PLACEBO-CONTROLLED TRIAL Janni Jensen1,2, Frank H Mose1, Anna-Ewa O Kulik1, Jesper N Bech1 and Erling B Pedersen1,2 1 Regional Hospital Jutland West, Holstebro, Denmark, 2Aarhus University, Aarhus, Denmark Introduction and Aims: Urinary excretion of aquaporin2 (u-AQP2) and the γ-fraction of epithelial sodium channels (u-ENaCγ) are used to evaluate the water transport via aquaporin-2 water channels (AQP2) and sodium transport via epithelial sodium channels (ENaC) in the principal cells in the distal nephron. We wanted to test the hypothesis that the functional state of AQP2 and ENaC in healthy humans change, iii | Abstracts Nephrology Dialysis Transplantation both at baseline and after 3 % hypertonic saline, while inhibiting the sodium chloride cotransporter (NCC) with thiazide or ENaC with amiloride. Methods: In a randomized, double-blinded, placebo-controlled, crossover study, 23 healthy subjects on a standardized diet, regarding calories, sodium and fluid, were studied. The subjects recieved amiloride 5 mg, thiazide 1.25 mg or placebo twice a day for 5 days before each examination day. At baseline and after an infusion with 3% hypertonic saline, we measured urinary concentrations of u-AQP2, u-ENaCγ, glomerular filtration rate (GFR) estimated by 51Cr-EDTA clearance, free water clearance (CH2O), fractional excretion of sodium (FENa) and potassium (FEK), plasma concentrations of sodium ( pNa) and potassium ( pK), vasopressin ( pAVP), renin (PRC), Angiotensin II ( pANG II), Aldosterone ( pAldo), brachial blood pressure (bBP) and central blood pressure (cBP) estimated by applanation tonometry and extracellular volume (ECV) using bioimpedance spectroscopy technique. Results: At baseline, there were no differences in u-AQP2, u-ENaCγ or 24-h bBP. Both thiazide and amilorid increased PRC, pAng II and pAldo and decreased ECV. Amiloride increased FENa and pK, while pNa decreased. Thiazide decreased CH2O, pNa and pK. After hypertonic saline, u-AQP2 increased during placebo and amilorid, but not during thiazide. In addition, CH2O decreased less during thiazide compared to amilorid and placebo. U-ENaC and FENa increased in all three groups. PRC, AngII and p-Aldo decreased to the same extent, while AVP increased, but to a significant smaller degree during thiazide. ECV and bSBP increased slightly in all three groups, while thiazide decreased bDBP and cDBP. Conclusions: The study documents that in healthy humans, volume expansion with 3% hypertonic saline, result in a lower reabsorption of water via AQP2 during thiazide compared to amilorid and placebo. This might be due to a reduced stimulation of AVP on receptors located in the basolateral membrane of the principal cell. The increase in u-ENaCγ might be compensatory phenomena to counteract a decreased reabsorption of sodium in proximal tubules. Volume 29 | Supplement 3 | May 2014








![CLIP-inzerat postdoc [režim kompatibility]](http://s1.studyres.com/store/data/007845286_1-26854e59878f2a32ec3dd4eec6639128-150x150.png)