Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
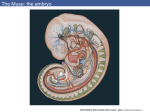
Embryo Embryo Transfer Transfer Advanced assisted reproductive techniques have given birth to thousands of children once considered impossible to conceive. Through remarkable technical innovations such as intracytoplasmic sperm injection (ICSI)—the injection of a single sperm directly into the oocyte—most couples are now able to achieve fertilization. Still, even if fertilization and initial embryonic cleavage proceed normally, the embryo must continue to develop normally. The formulation of new laboratory media—the liquid in which the embryos are grown in vitro--has made it possible to safely grow embryos in vitro beyond the typical 2-3 day stage of development. Promising studies suggest that transfer of the embryo on day 5, at the blastocyst stage of development, yields higher pregnancy rates, even for patients who have previously failed embryo transfer. Embryonic Development On day one, 16 hours after the sperm and egg(s) are combined in vitro, a fertilized egg called a pronuclear embryo is formed. It contains nuclei from the egg and the sperm. During the next 24 hours the two nuclei combine and the embryo divides into two, or sometimes into four cells by day 2. Approximately 72 hours following fertilization, on day 3, the embryo has further divided into 8-12 cells, the point at which most embryo transfers have been traditionally undertaken. Extra embryos not transferred at this time were often cryopreserved, and then thawed for a subsequent future transfer. The average number of embryos transferred was four, and this approach resulted in a historical pregnancy rate of approximately 35-40%. A blastocyst is the final stage of embryonic development before it hatches out of its shell, or zona pellucida, and implants in the uterine wall. Only the most viable embryos reach this stage of development. During the 4th and 5th days following oocyte retrieval the embryo forms a cavitating morula, or early blastocyst, and then continues to grow to approximately 100 cells with distinct inner and outer cell masses. The embryo becomes much larger, while the outer shell begins to thin in preparation for hatching. Day 1 Day 2 Day 4 Day 3 Day 5 Blastocyst An oocyte and early embryo is ~120 micrometers in diameter while a blastocyst is ~200 micrometers. 1 micrometer = 1 millionth of a meter. 1000 micrometers = 1 cm and 2.5cm = 1 inch www.CTfertility.com BRIDGEPORT 4920 Main Street, (203)373.1200 NORWALK 148 East Avenue, (203)855.1200 ORANGE 339 Boston Post Road, (203)799-1200 Embryo Quality Human embryos require different substrates in their culture media after they develop to the 6-8 cell stage (i.e.: day 3). The embryos are closely examined on day 3 of development when they are moved to a specialized blastocyst culture media. At that time we assign a letter grade based upon the rate of cellular division; the lucidity, structure, size and shape of the individual cells; and the percentage of intracellular fragments observed under high magnification. If there are at least five good quality embryos on day 3, the embryo transfer can be delayed until day 5. Delaying transfer of the embryo until day 5 allows longer observation of the embryo’s development in vitro, and the ability to carefully assess embryo quality. This longer observation period allows the most highly developed embryos to be selected for transfer. “Arrested” embryos (i.e.: those with no potential for pregnancy because they have failed to develop) are not considered suitable for embryo transfer or cryopreservation. Pregnancies do occur from embryos that have not reached the blastocyst stage, but data suggest that patients who undergo transfer of embryos that have reached the blastocyst stage have a higher likelihood of achieving pregnancy. On average 30-50% of a patient’s embryos usually develop to the blastocyst stage. If a patient has less than five good quality embryos, there is a statistically smaller chance that the embryos will develop into blastocysts when allowed to remain in the laboratory. When there are fewer than five good quality embryos during the early lab period, we prefer to transfer the embryos on day 3 and return the embryos to a more natural environment. More embryos may be transferred at this time since we have fewer embryos from which to select the best. Decreased Multiple Pregnancy Rate Embryo selection and extended culture to the blastocyst stage help increase implantation rates and allow the transfer of fewer embryos. Therefore, the risk of multiple births and their associated problems is greatly reduced. At CFA we prefer to transfer as few embryos as possible to achieve a healthy pregnancy. Cryopreservation Extra embryos can be safely cryopreserved and stored. At CFA, approximately 99% of cryopreserved embryos survive the thawing process for embryo transfer and result in a >50% pregnancy rate. Vitrification is the process that is utilized for cryopreservation. This is a flash freezing process which prevents ice crystal formation. Ice crystal formation is the main reason embryos don’t survive cryopreservation as they rupture the cell membranes when the embryo is thawed. Only about one third of couples undergoing the IVF process will have enough high quality embryos to cryopreserve. Furthermore, there have been babies born from cryopreserved embryos which were stored over 20 years. Theoretically, because the liquid nitrogen that we store the cryopreserved embryos in is such a low temperature, the embryos can remain viable in storage for up to 2,000 years. In conclusion, studies on human embryos to date have shown no harm to the children born from the extended IVF culture conditions encountered with blastocyst development, transfer, and cryopreservation. Please visit our website: http://www.CTFertility.com to learn more about these techniques and to view our most recent success rates. www.CTfertility.com BRIDGEPORT 4920 Main Street, (203)373.1200 NORWALK 148 East Avenue, (203)855.1200 ORANGE 339 Boston Post Road, (203)799-1200