Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
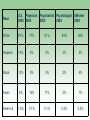
Psychiatric Illnesses and Ethnic Minorities Jeanne Miranda, Ph.D. UCLA Neuropsychiatric Institute Foster Care Assessment Program, University of Washington, School of Social Work January 28, 2009 Disclosure At this time, I have no actual or potential conflict of interest in relation to this program. We will cover: Minorities in the U.S. Rates of mental disorders of minorities Disparities in mental health care of minorities Response to evidence-based care Bringing care to ethnic minority communities Minorities in the U.S. 1924 Immigration Act - national origins system - 2% of foreign-born in 1890. Until 1960, majority of all legal immigrants were from Europe and Canada. 1965 Immigration Act - 20,000 from each country in Eastern Hemisphere. Minorities in U.S. 14% Hispanic American 13% African American 5% Asian American 1.5% American Indian/Alaskan Native Minorities in the U.S. 30% of population. In 50 years - 57% of under 18. Immigration now worldwide. Growing percentage of population and growing more diverse Minorities in the U.S. • Racism and Race Indirect effects through stress, segregation, poorer education. Direct effects through inequitable distribution of medical resources Minorities in the U.S. Historical perspective essential Legally sanctioned discrimination and exclusion of ethnic minorities is the rule, rather than the exception, for much of the history of this country. Minorities in the U.S. POVERTY 8.7% of White Americans 9.8% of Asian/Pacific Islanders 21.9% of Hispanic Americans 24.5% of Am Indians/Alaskans 24.7% of African Americans Rates of Mental Disorders Income is not monotonically related to mental disorders. – more common among the impoverished. – serious and persistent disorders frequently result in poverty. Symptoms are monotonically related to SES. Rates of Mental Disorders Lifetime Past Year Latino American % % Puerto Rican 38.98 22.88 Cuban 28.38 15.91 Mexican 28.42 14.48 Other Latino 27.29 14.42 Asian American % % Chinese 18.00 10.00 Filipino 16.74 8.99 Vietnamese 13.95 6.69 Other Asian 18.29 9.55 Black American % % African American 30.54 14.79 Caribbean Black 27.87 16.38 37.37 19.00 White American Rates of Mental Disorders Disorders are not higher in minorities. – Rates of disorders – Rates of depression* 25% of Mexican immigrants 48% of U.S.- born Mexicans U.S.-born black women – 10.5 African-born black women – 3.9 Caribbean-born black women – 4.8 Symptoms are higher in minorities Minorities recover less Rates of Mental Disorders Some evidence African Americans have increased rates of schizophrenia. American Indians have higher rates of PTSD and alcoholism and lower rates of depression. Southeast Asian refugees have extremely high rates of PTSD and depression Disparities do exist in care Minorities in need of care are less likely to get care than are white Americans. Minorities getting care are less likely to get quality care than are white Americans. Any depression treatment Psychiatric Visits Psychiatry Visits 100% 92.9% 92.5% 90% 85.0% 87.8% 91.5% 86.4% 80% 70% 91.4% 91.1% 91.1% 83.8% 69.5% Percent 66.0% 60% 50% 40% 30% 20% White Black Hispanic 10% 0% 1995 - 1996 1997 - 1999 2000 - 2002 Time period 2003 - 2005 Any depression treatment Primary Care Visits Primary Care Visits 20% 18% 16% Percent 14% 12.4% 12% 8% 6% 10.8% 10.4% 9.5% 10% 7.6% 6.6% 6.1% 8.5% 7.7% 9.8% 9.0% 7.1% White Black 4% Hispanic 2% 0% 1995 - 1996 1997 - 1999 2000 - 2002 Time Period 2003 - 2005 Disparities in Mental Health Care Logistic barriers – – – Insurance Providers who speak language Child care/work/life demands Stigma Somatization U.S. Department of Health and Human Services. (2001). Mental Health: Culture, Race, and Ethnicity—A Supplement to Mental Health: A Report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Office of the Surgeon General. People without Health Insurance Coverage by Race using 3-yr Average: 2003 to 2005 White Asian Black American Indian Hispanic 11.2% 17.7% 19.5% 29.9% 32.6% Source: U.S Census Bureau, Central Population Report, Income, Poverty, and Health Insurance Coverage in the United States: 2005 Race U.S. Physician 2005 2005 White 67% 77% 81% 93% 92% Hispanic 14% 4% 5% 3% 3% Black 13% 5% 3% 2% 4% Asian 5% 14% 11% 2% 1% 1.5% 0.1% 0.1% 0.3% 0.2% Amer.Ind Psychiatrist Psychologist SWorker 2002 2004 2004 Stigma Concerns Nationally representative insured HCC sample Friends Employers Insurers n=5,930 N=5,589 N=5,589 Little/no concern 72% 26% 25% Some/a lot of concern 28% 73% 76% Response to Evidence-based Care Culturally competent care – Evidence being culturally competent doesn’t improve outcomes – Definitely not memorizing facts about culture, which continually shifts, but awareness of important issues – Being sensitive to historical perspectives and power differences – Being aware of the context of an individual’s life Response to Evidence-based Care African Americans and Latinos appear to respond similarly or better than do white Americans. The few trials of Asians are promising. American Indians/Alaskan Natives haven’t been studied. Promise of Quality Improvement Partner’s in Care – QI Study – 46 practices across U.S.* Randomized resources to improve medication management or psychotherapy for depression Latinos and African Americans – Less quality care at baseline Miranda J, Duan N, Sherbourne C, Schoenbaum M, Lagomasino I,Jackson-Triche M, Wells KB. Can Quality Improvement Interventions Improve Care and Outcomes for Depressed Minorities? Results of a Randomized Controlled Trial. Health Services Research, 38(2):613-630. 2003. Clinics Were Randomized Usual Care (UC) QI-THERAPY QI-MEDS support for psychotherapy support for medication management Interventions • “Depression nurse” supported patient education, assessment, and getting started on treatment • Primary care clinicians were taught about depression • Patients and doctors could choose any treatment, or no treatment • Provider networks were taught CBT Interventions Increased Appropriate Care for All QI programs Usual care African American Latino White 0 10 20 30 40 50 % receiving appropriate care at 1 year 60 70 80 Percentage with Probable Depression 6 Mo. Response to QI Resources 70 60 % Depressed 50 40 QI 30 Control 20 10 0 Latina Black White Implications How we manage depressed patients for even one episode (information and treatment) can have long-term consequences over many years – Patients may not need prolonged management by providers to reap some long-term gains The most vulnerable depressed populations may have the most to gain from efforts to improve care Similar Interventions Help: Youth Partners in Care QI intervention for depressed youth in primary care increased rates of specialty care and counseling, improved depressive symptoms at 6 month followup - similar to PIC Minorities benefited more than did white youth WE Care for Impoverished Women Randomized trial of 267 women screened in county entitlement clinics – – – CBT Guideline concordant medication (Paroxetine) Referral to community care 9-11 telephone outreach calls necessary to engage women in care Flexibility of care Babysitting and transportation provided Miranda J, Chung JY, Green BL, Krupnick J, Siddique J, Revicki DA, Belin T. Treating Depression in Predominantly Low-Income Young Minority Women: A Randomized Controlled Trial. JAMA, 290(1):57-65. 2003. Treatment Received 88 medication – 90 CBT – 67 (76%) received appropriate care 32 (35.5%) received appropriate care 89 referred – – 15 (16.9%) received at least one session 74 (83.1) did not attend care Response to Care 6-month outcomes – asymptomatic – 44.4% medication – 32.2% CBT – 28.1% referred Response to Care 12-month outcomes – asymptomatic – – – 41.6% medication 48.9% CBT 30.3% referred Cost-effectiveness ratios similar to those in advantaged populations Public Sector Challenges for Young Mothers Mental health departments prioritize severe mental illness Primary care has limited resources “Depression is everyone’s problem…but nobody’s business” Lack of insurance is a huge barrier to care Public sector services may not be places of trust Conclusions Understanding context of minorities lives are important to treatment. For the most part, minorities do not have higher rates of disorders. For the most part, evidence-based care works for African Americans and Hispanics and is promising for minorities. Conclusions Minorities with disorders are particularly unlikely to get care. – – – – – Treating minorities in settings the trust and frequent. Engaging in outreach to minorities. Improving overall quality of care Overcoming barriers, such as transportation, babysitting, time of care, etc. Increasing rates of minority providers.