Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
بسم هللا الرحمن الرحيم
﴿و ما أوتيتم من العلم إال قليال﴾
صدق هللا العظيم
االسراء اية 58
By
Dr. Abdel Aziz M. Hussein
Lecturer of Medical Physiology
•
•
•
•
•
•
•
•
•
•
Given these structures:
1. basement membrane
2. fenestra
3. filtration slit
Choose the arrangement that lists the structures in the
order a molecule of glucose encounters them as the
glucose passes through the filtration membrane to
enter Bowman’s capsule.
a. 1,2,3
b. 2,1,3
c. 2,3,1
d. 3,1,2
e. 3,2,1
Def.,
• Means the bulk flow of a solvent through a filter
carrying with it the solutes that are small enough to
pass through the filter.
Blood
Capillary
endothelium
Basement
Membrane
Podocytes
slits
Bowman
Capsule
Def.,
• It is an ultrafiltration since it is plasma minus
plasma protein and cellular elements while simple
filtration excludes only cellular elements.
Blood
Capillary
endothelium
Basement
Membrane
Podocytes
slits
Bowman
Capsule
Blood Cells
Plasma proteins
Plasma solutes
Dynamics:
• Glomerular Filtration is formed by the forces of
filtration as many capillary filtrate in the body
(Starling's forces of filtration).
• They are 4 forces;
2 Hydrostatic pressures
2 Oncotic pressures
Glomerular
capillary
Glomerular
Hydrostatic
Pressure (Gp)
Glomerular
Oncotic Pressure
(Gπ)
Capillary
endothelium
Basement
Membrane
Podocytes
slits
Bowman
Capsule
Bowman oncotic
Pressure (B π)
Bowman
Hydrostatic
Pressure (Bp)
Gp = 60
mmHg
Bπ = 0
mmHg
Gπ = 32
mmHg
Gp = 18
mmHg
• GFR is determined by Starling's principle;
″The rate & direction of fluid movement is proportional
to the algebraic sum of hydrostatic & oncotic
pressures″
• So, GFR α (hydrostatic pressure – oncotic pressure)
GFR α { (Gp- Bp) – (Gπ – Bπ)}
• KF = filtration coefficient
•Net filtering force {60-(32+18)} = 10 mmHg and
GFR = 120 mL/ min
Glomerular
filtration
Systemic capillary
filtration
Exchange 1.6 m2 – of which only 1000 m2 of systemic
2-3% are available for capillary 25%- 35% are
filtration (320-480 cm2) opened 250- 350 m2
Pulmonary capillary Surface
area is 60 m2.
Filtration Rate
180 L/day
20 L/day are filtered at
arterial end, of which 18L are
reabsorbed at venous end &
2L by lymphatic.
Capillary Hydrostatic 45-60 mmHg
32 mmHg at art. end &
Pressure
decrease to 15 mmHg at
venous end
Osmotic Pressure of 25 mmHg at afferent 25 mmHg along the whole
Plasma Protein
end of capillary & rises length
to 37 mmHg at efferent
end of capillary.
Filtration Coefficient 4mL/min/1 mmHg/100 0.01mL/min/1mmHg/100
gm
gm.
Capillary
Area
Gπ = 25
mmHg
Gp = 60
mmHg
Gπ = 37
mmHg
Def.,
• Volume of plasma filtered by both kidney per unit time
Value:
– 125 ml/min
– 180 L/day or
– 60 nl/min for single nephron (SNGFR).
Filtration fraction: is part of RPF filtered in Glomeruli
GFR
=
125 ml/min
=
RPF
= 1/5 or 20%
650 ml/min
RPF
650 ml/min
FF= 120/ 650 = 20%
GFR
120 ml/min
RPF
649 ml/min
Urine flow rate
1 ml/min
Significance of High GFR:
• To ensure processing of plasma (3L) about 60
times/day (since daily GFR = 180L/day prevents
accumulation of metabolites.
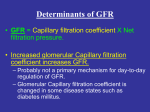
Causes of high GFR:
1) High filtration coefficient:
• KF is volume of fluid filtered /min/ mmHg
pressure difference across the membrane
Causes of high GFR:
1) High filtration coefficient:
• For the kidney 4 ml/ min/ mmHg/ 100 gm
tissue or 12 ml/ min/ mmHg/ 300gm (both
kidneys).
• For systemic capillary 0.01 ml/ min/ mmHg/
100gm tissue.
• This is due to high permeability of the glomerular
membrane for same hydrostatic pressure
gradient.
Causes of high GFR:
2) High capillary hydrostatic P.:
• It is about 45- 60 mmHg in glomerular capillary
• In systemic capillary 32 mmHg at arterial end and 15
mmHg at venous end
Causes of high GP:
1. Renal artery → short, wide, direct branch from aorta.
2. Afferent arteriole → straight branch of interlobular
artery
3. Efferent arteriole → narrower than afferent arteriole
4. Glomerular capillaries →present between two arteries
Causes of high GFR:
3) High RPF.:
• It is about 600ml/ min.
• This high RBF eventually leads to high GFR.
RBF
Factors Affecting GFR:
Glomerular
hydrostatic pressure
• About 45 – 60 mmHg
• Help GFR
Bowman’s capsular
hydrostatic pressure
• About 18 mmHg
• Oppose GFR
Oncotic pressure of
plasma protein
• About 32 mmHg
• Oppose GFR
Renal plasma flow
(RPF)
Filtration coefficient
• About 650 ml/min
• Help GFR
• About 4 ml/min/ 1mmHg/ 100 gm
• Help GFR
• It is high compared to systemic capillary
Causes of high GP
Factors affecting:
A) Systemic ABP:
• Between 80- 180 mmHg ( no change)
• Less than 80 mmHg → ↓ Gp
• More than 180 mmHg →↑ Gp
B) Balance between afferent and efferent arterioles
resistance
• It is about 18 mmHg helps to maintain renal
tubules patent.
• Acts as a driving force to propel glomerular
filtrate along whole length of renal tubules.
• If increased e.g. in ureteric obstruction
decrease GFR.
Bp
Increased Bp
• Normally 32 mmHg.
• If changed marked effect on GFR.
• Increase plasma oncotic pressure decrease
GFR.
• As in:
1. Marked hyperproteinemia as in multiple
myeloma.
2. Dehydration, hemorrhage, sever burns &
chronic diarrhea.
Gπ
• Leakage of plasma albumin from glomerular
membrane in some pathological conditions
decrease plasma oncotic pressure &
increase Bowman’s oncotic pressure
increase GFR.
• RPF affect indirectly the plasma oncotic
pressure
• Increase RPF maintain normal plasma
oncotic pressure and filtration equilibrium is
achieved too late helps GFR.
• Decrease RPF elevates plasma oncotic
pressure decrease GFR.
High RPF
• It is the effectiveness of the permeability of the
barrier.
• It depends on:
1. Hydraulic conductivity (water permeability of the
barrier).
2. Effective filtration surface area
2. Effective filtration surface area is affected by:
a. Total number of functioning glomeruli.
b. State of intraglomerular mesangium.
• Their contraction (e.g. by AII) decrease effective
filtration area & their relaxation (e.g. by dopamine)
increase effective surface area.
V.D. of afferent arterioles
↑ Gp
↑ RPF
FF = no change
↑ GFR
V.C. of afferent arterioles
↓ Gp
↓ RPF
FF = no change
↓ GFR
V.D. of efferent arterioles
↓ Gp
↑ RPF
FF = decrease
↓ GFR
V.C. of efferent arterioles
↑ Gp
↓ RPF
FF = Increase
↑ GFR
Afferent
Efferent
RPF GFR
(Preglomerular (Postglomerular
resistance)
resistance
VC
VD
---
--VC
VD
FF
(GFR /
RBF)
constant
constant
إيمحتب
THANKS