Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
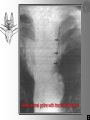
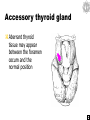
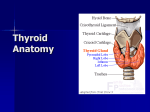
The thyroid gland The thyroid gland Lobes Position Blood supply Development Parathyroid glands Tracheostomy Related topic Plan of the neck The thyroid gland derives its name from the thyroid cartilage which resembles a shield (G. thyreos = shield) Function The thyroid gland is an endocrine gland that is responsible for the secretion of thyroxin and thyrocalcitonin Lobes The thyroid gland consists of two lobes united in front of the second, third and fourth tracheal rings by an isthmus of gland tissue. isthmus Lobes Each lobe is pearshaped consisting of a narrow upper pole and a broader lower pole upper pole lower pole Thyroid scan This nuclear scan uses an injectable radioactive compound. When injected into the bloodstream the compound will be concentrated in the thyroid gland resulting in an image of the gland The test can be useful in diagnosis of thyroid tumor sternothyroid sternohyoid Position It lies under cover of sternothyroid and sternohyoid muscles on the side of the larynx and trachea Position thyrohyoid sternothyroid cricothyroid Thyroid, upper pole The upper pole of the thyroid cannot normally rise above the level of the oblique line of the thyroid cartilage thyrohyoid cricothyroid cricoid The thyroid gland is caught in the pocket of sternothyroid thyroid cartilage Position thyroid sternothyroid Position The lower pole of the thyroid gland extends along the side of the trachea as low as the sixth tracheal ring 1 2 3 4 5 6 esophagus Because of the proximity of the thyroid gland to the trachea and esophagus, goiter causes compression of the trachea and esophagus resulting in dyspnea and dysphagia respectively Retro-sternal goitre with tracheal deviation Retro-sternal goitre with esophageal deviation Pyramidal lobe In about 40% of people, there is a small upwards extension of the isthmus called the pyramidal lobe. Levator glandulae thyroidae The pyramidal lobe may be attached to the hyoid bone by fibrous or muscular tissue (levator glandulae thyroidae). Variations Bifurcation of the lower end of the pyramidal process, one part going to each lateral lobe Variations Pyramidal process attached to the left lobe of the gland, isthmus absent. Variations Both pyramidal process and isthmus are absent. Pre-tracheal fascia The thyroid gland is surrounded by a fibrous capsule and is enclosed in the pretracheal fascia Pre-tracheal fascia The pre-tracheal fascia attaches the thyroid gland to the trachea and larynx thus the thyroid moves upwards on swallowing, an important diagnostic feature for lumps in the neck larynx thyroid Blood supply The thyroid gland is very vascular The vessels lie between the capsule and the pretracheal fascia. In some pathological conditions such as thyrotoxicosis, owing to its high vascularity, the blood flow can be heard with a stethoscope as a bruit Thyroid arteries The main arteries are the superior and inferior thyroid arteries. inferior thyroid a. superior thyroid a. Superior thyroid artery external carotid a. carotid bifurcation Arises from the anterior surface of the external carotid immediately distal to the carotid bifurcation. Superior thyroid artery Arches downwards, giving a sternomastoid branch and a superior laryngeal branch that enters the larynx with the nerve of the same name superior laryngeal a. & n. Superior thyroid artery enters deep to sternothyroid sternothyroid Superior thyroid vessels Superior thyroid artery before reaching the upper pole of the gland, and within the pre-tracheal fascia, it divides into two main branches one for either surface of the gland anterior posterior Superior thyroid artery the posterior branch anastomoses with the inferior thyroid artery posterior br. of superior thyroid a. inferior thyroid a. Inferior thyroid artery Is a branch of the thyrocervical trunk from the subclavian artery. inferior thyroid a. thyrocervical trunk subclavian a. Inferior thyroid artery Ascends and turns medially at the level of the cricoid cartilage to enter the back of the gland some distance above the lower pole. Inferior thyroid artery The tortuous course of the inferior thyroid artery is due to the fact that in every swallow the thyroid gland ascends a few centimeters and must naturally drag its blood supply with it. If this artery has no capability to elongate, it would be traumatized Inferior thyroid artery Divides outside the pre-tracheal fascia into four or five branches that pierce the fascia separately to reach the lower pole of the gland. Remember that the superior thyroid artery divides within the pretracheal fascia The recurrent laryngeal nerve lies normally behind the branches of the inferior thyroid artery The recurrent laryngeal nerve lies normally behind the branches of the inferior thyroid artery but it is common for the nerve to pass between the artery branches before they pass through the fascia. The recurrent laryngeal nerve always lies behind the pretracheal fascia and if this structure remains intact during thyroidectomy the nerve will not have been divided inferior thyroid a. recurrent laryngeal n. Both thyroid arteries are related to nerves which must be avoided when tying the arteries. A little distance behind the superior thyroid artery is the external laryngeal nerve. superior laryngeal n. internal laryngeal n. external laryngeal n. superior thyroid a. external laryngeal n. Superior laryngeal nerve variations vagus internal external To avoid injury to the external laryngeal nerve, the superior thyroid artery is ligated and sectioned near the superior pole of the thyroid gland where it is not so closely related to the nerve as it is at its origin. Section of the external laryngeal nerve produces weakness of voice, since the vocal fold cannot be tensed. The cricothyroid muscle is paralyzed Cricothyroid tenses the vocal cord The recurrent laryngeal nerve has a variable relationship to the inferior thyroid artery because of its proximity to the inferior thyroid artery and the pre-tracheal fascia it may be injured while ligating the artery during thyroidectomy hence the advisability of ligating the inferior thyroid artery well lateral to the gland before it begins to divide into its terminal branches. the inferior thyroid artery gives off esophageal and inferior laryngeal branches before its terminal distribution into the thyroid gland site of superior thyroid a. ligation site of inferior thyroid a. ligation The variable relationship of the inferior thyroid artery to the recurrent laryngeal nerve makes thyroid surgery a potential risk to normal speech The recurrent laryngeal nerve supplies all the intrinsic muscles of the larynx it is advisable that a surgeon about to perform a thyroidectomy examines the vocal cords prior to operation, so that if there is any problem postoperatively one knows at least the origin of the lesion. Recurrent laryngeal nerve damage Is a complication of thyroid surgery that causes paralysis of the vocal cords When bilateral the voice is almost absent as the two vocal folds cannot be adducted. Recurrent laryngeal nerve damage A unilateral recurrent laryngeal nerve injury may not be noticed in normal speech but would be very detrimental to a singers career. The thyroid arteries anastomose freely with each other and with tracheal and esophageal arteries. In operations of partial or sub-total thyroidectomy, all four arteries are tied In operations of partial or subtotal thyroidectomy, all but the posterior part of the gland excised remaining thyroid tissue the dangerous anatomy lies in the posterior lateral lobes (recurrent laryngeal nerve and the parathyroid glands) parathyroid gland Recurrent laryngeal n. The remains of the gland are located alongside the trachea and contain the parathyroid glands, the whole being supplied with blood by the anastomosis Thyroidae ima artery In about 10% of individuals, an unpaired artery, the thyroidae ima (L. ima = lowest) is a small occasional artery from the brachiocephalic trunk, or left common carotid artery, or direct from the arch of the aorta Thyroidae ima artery Ascends anterior to trachea and supplies the isthmus of the thyroid gland. Thyroidae ima artery The possible presence of the thyroid ima artery must be remembered when incising the trachea inferior to the isthmus. As the thyroidae ima runs anterior to the trachea, it is a potential source of serious bleeding Internal jugular v. Thyroid veins The veins are three in number on each side the superior thyroid vein from the upper pole follows the artery and enters the internal jugular vein or the common facial vein Superior thyroid v. Internal jugular v. Thyroid veins The middle thyroid vein is short and wide, it enters the internal jugular vein middle thyroid v. Thyroid veins From the isthmus and lower pole of the gland the inferior thyroid veins form a plexus within the pretracheal fascia that descends in front of the trachea to reach the left brachiocephalic vein inferior thyroid vv. brachiocephalic v. Inferior thyroid veins As the inferior thyroid veins cover the anterior surface of the trachea inferior to isthmus, they are potential sources of bleeding during tracheotomy (also remember the situation of the thyroidae ima artery). Development of the thyroid gland The gland begins as a diverticulum from the floor of the embryonic pharynx Development of the thyroid gland The diverticulum grows caudally superficial to the hyoid before dividing into two lobes The stem of the diverticulum, the thyroglossal duct, normally disappears hyoid Thyroglossal duct Development of the thyroid gland After the tongue has developed, it can be seen that the point of outgrowth of the thyroglossal duct is the foramen cecum (of Morgagni) [Morgagni, Giovanni Battista, 1682-1771, a Padua anatomist and pathologist, also known for hydatid of Morgagni (appendix testis) and anal columns (of Morgagni)]. Thyroglossal cyst cysts derived from the duct may also appear anywhere between the foramen cecum and the normal position in the midline of the neck 1. 2. 3. 4. 5. 6. Beneath foramen cecum Floor of the mouth Suprahyoid Subhyoid On thyroid cartilage At level of cricoid cartilage Thyroglossal cyst Can be diagnosed because characteristically it moves upwards as the patient puts his tongue out. Infection of a thyroglossal cyst may spread to a persistent thyroglossal duct which must be then excised Although the duct lies ventral to the hyoid bone, it passes up for a short distance behind the body, which therefore has to be excised with the duct Accessory thyroid gland Aberrant thyroid tissue may appear between the foramen cecum and the normal position Lingual thyroid Rarely the thyroid fails to descend during development resulting in the development of a lingual thyroid Ectopic thyroid Failure of descent mar result in a superior cervical thyroid in the region of the hyoid bone the thyroid may sometimes descended too far and be found in the superior mediastinum Parathyroid glands Two on each side They are yellow-brown endocrine glands, about the size of a small pea (about 0.5x0.8 cm ovoids) They are important because of their role in calcium metabolism. They secrete parathormone that mobilizes bone calcium and increases gut and kidney calcium absorption Parathyroid glands Are located posterior to the thyroid gland between its capsule and fascial sheath Superior parathyroid glands more constant in position embedded in the posterior surface of the thyroid gland, a short distance above the entry of inferior thyroid artery (and the level of the cricoid cartilage). Inferior parathyroid glands variable in position usually embedded behind the lower pole but is often found elsewhere (they may even present in the superior mediastinum). Parathyroid development The parathyroids develop from the endoderm of the third (inferior gland) and fourth (superior gland) pharyngeal pouches Parathyroid development The thymus also develops from the third pouch and may therefore carry the inferior parathyroid with it when it descends into the thorax. Parathyroid glands, blood supply The glands are usually supplied by the inferior thyroid arteries but may also be supplied by both superior and inferior thyroid arteries posterior br. of superior thyroid a. inferior thyroid a. Parathyroid glands Awareness of the close relationship between the parathyroid glands and the thyroid gland is essential to prevent removal or damage of the parathyroid glands during thyroidectomy. The parathyroid glands are usually safe during subtotal thyroidectomy because the posterior part of the thyroid gland is preserved The variability in position of the parathyroid glands may create a problem during total thyroidectomy; in this case the parathyroid glands are saved by following their small vessels which are kept intact before the thyroid is removed. Endotracheal tube Tracheostomy When tracheostomy is done electively after establishing an airway with an endotracheal tube, a short transverse incision is made one cm below the cricoid cartilage Tracheostomy The transverse incision is made midway between the cricoid cartilage and the sternal notch Tracheostomy The decussating fibers of platysma are divided. Tracheostomy After elevating platysma, the investing fascia between the strap muscles is incised Tracheostomy The pretracheal (strap) muscles are seperated Tracheostomy The pretracheal fascia is split longitudinally The thyroid isthmus is divided and sutured Tracheostomy The second tracheal ring is precisely identified and divided vertically in the midline, extending the incision through the third ring in most cases The first ring is preserved Tracheostomy A thyroid retractor gently spreads the tracheal opening. The tracheostomy tube with obturator is introduced after withdrawing the endotracheal tube under direct vision to a point just above the stoma Tracheostomy tube retractor Endotracheal tube Tracheostomy tube flange Tracheostomy If more room is needed, the fourth ring may be partially divided A transverse incision is to be avoided. The skin is closed loosely The flange of the tracheostomy tube not only is tied with a tape around the neck but also is sutured to the skin. 4th tracheal ring Tracheostomy The endotracheal tube is removed only when the tracheostomy tube has been shown to provide a satisfactory airway If there is any question about where the tip of the tube lies, a flexible bronchoscope may be used to check the distal position. Tracheostomy The tracheostomy tube should be just large enough to provide an adequate airway for the patient. Larger tubes can only cause damage. It must be remembered that most women, even when obese, have tracheas smaller in diameter than those of men Permanent tracheostomy opening Complications of tracheostomy the anterior jugular veins may be encountered as the superficial fascia is incised They are avoided by maintaining a midline position Complications of tracheostomy Sometimes a large jugular venous arch may be encountered Complications of tracheostomy The inferior thyroid veins are often asymmetric, hence more liable to injury Complications of tracheostomy The branches of the superior and inferior thyroid arteries may anastomose across the midline Complications of tracheostomy A thyroid ima artery is very occasionally present and must be ligated if found Complications of tracheostomy The brachiocephalic artery and vein may be injured if sharp dissection is carried too far downwards The artery may be eroded by a tracheostomy tube, resulting in a tracheoarterial fistula Complications of tracheostomy In children the left brachiocephalic vein and the thymus may extend above the suprasternal notch. Complications of tracheostomy Tube too curved Tube too low The subclavian artery and vein may be compromised by a tracheostomy to that is incorrectly curved or is placed too low Complications of tracheostomy The existence of fascial planes predisposes to surgical emphysema, particularly if the skin is sutured too tightly. Investing fascia Complications of tracheostomy Surgical emphysema may extend into the mediastinum. Investing fascia pretracheal fascia Complications of tracheostomy Beware of overenthusiastic incision into the trachea; the esophagus is immediately posterior. Skin & superficial fascia Investing fascia Thyroid & pretracheal fascia trachea esophagus