Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
History of invasive and interventional cardiology wikipedia , lookup
Coronary artery disease wikipedia , lookup
Marfan syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Turner syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Aortic stenosis wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
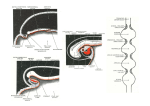
Vascular Ring Due to Left Aortic Arch and Right Descending Aorta WILLIAM BERMAN, JR., M.D., STEVEN M. YABEK, M.D., TERRENCE DILLON, M.D., JOE F. NEAL, M.D., BECHARA AKL, M.D., AND JEROME BURSTEIN, M.D. SUMMARY Two children presented with symptoms suggestive of a vascular ring. Barium esophagrams in each case showed a posterior impression caused by a retroesophageal aortic arch. Angiographic studies defined a rare form of vascular ring resulting from an ascending left-sided aorta, a descending right-sided aorta and a right-sided ligamentum arteriosum. At surgery, the diagnosis was confirmed and the anomaly was corrected in each patient. Left pulmonary anomalies were present in each patient. Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 A vascular anomaly of the great vessels was suspected, so cardiac catheterization was performed. There was mild right ventricular and pulmonary artery hypertension (40-mm Hg systolic pressure). No intra- or extracardiac shunts were detected. Angiography revealed no anatomic intracardiac defects. Left ventriculograms showed that the aorta arose normally from the left ventricle and ascended anteriorly and to the left in a normal fashion. In its terminal portion, the aortic arch turned medially, crossed the midline behind the esophagus, which it compressed, and descended to the right of the thoracic spine (fig. 2). There was an aberrant right subclavian artery arising from the descending thoracic aorta (fig. 3). The left pulmonary artery was smaller in caliber than the right. Surgery was performed 2 days later through a right lateral thoracotomy. The surgical findings confirmed the presence of a vascular ring. A ligamentum arteriosum, which originated from the descending aortic arch together with the anomolous right subclavian artery and inserted into the right pulmonary artery, completed the vascular ring and tethered the distal aortic arch anteriorly against the esophagus. The ligamentum was divided, and the esophagus was dissected and mobilized. Since surgery, the infant has been free of feeding difficulties or other symptoms and has gained weight appropriately. VASCULAR RINGS surrounding the trachea and esophagus are a cause of dysphagia and respiratory distress during infancy. Most symptomatic vascular rings result from a double aortic arch system or the coexistence of a right-sided aortic arch with a leftsided patent ductus arteriosus or ligamentum arteriosum. 1 2 We report the cases of two infants with marked dysphagia associated with an extremely unusual form of vascular ring. Feeding problems were managed successfully by surgery. Case Reports Case 1 This 1-month-old male infant was born after an uneventful, full-term gestation. Birth weight was 6 pounds, 3 ounces. He presented with a 2-week history of regurgitation, choking and nasopharyngeal reflux after all bottle feedings. He had no history of respiratory distress or cyanosis. On physical examination, vital signs were normal and weight was 8 pounds. The patient was acyanotic and the lungs were clear. Cardiac examination revealed normal pulses, a quiet precordium, a normal liver size and a grade 1I/VI high-pitched systolic murmur along the upper right and left sternal borders. The infant choked and regurgitated formula repeatedly through the nose and mouth during feeding. Laboratory evaluation showed normal electrolytes, blood count and urinalysis. A chest x-ray showed a normal heart size, normal pulmonary vascular markings, and scant right perihilar and right upper lobe infiltrates. An ECG was normal. A barium esophagram showed marked reflux of contrast material into the nasopharynx and extrinsic, posterior compression of the proximal esophagus (fig. 1). Case 2 This 3½/2-year-old female had a history of chronic dysphagia, recurrent lower respiratory infections and easy fatiguability. Physical examination showed normal peripheral pulses and blood pressures, a right ventricular lift, an increased intensity of the pulmonic component of the second heart sound and a grade 1I/VI systolic ejection murmur. A chest x-ray showed right ventricular enlargement and pulmonary venous congestion. The ECG showed right atrial and right ventricular hypertrophy. A barium esophagram showed a posterior impression on the esophagus. Cardiac catheterization revealed no intracardiac shunts; the pulmonary artery pressure was 72/25 mm Hg. The left pulmonary artery was not seen (fig. 4). The aortic arch ascended to the left, but descended on the right; the right subclavian artery arose from a diverticulum on the descending aorta. Through a right thoracotomy, a right-sided liga- From the Departments of Pediatrics, Surgery and Radiology, University of New Mexico School of Medicine, Albuquerque, New Mexico. Address for correspondence: William Berman, Jr., M.D., University of New Mexico School of Medicine, Department of Pediatrics, Albuquerque, New Mexico 87131. Received April 23, 1980; accepted June 4, 1980. Circulation 63, No. 2, 1981. 458 RETROESOPHAGEAL AORTIC ARCH/Bernan et al. 459 Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 PiGURE[ 3. Left ventricular angiogran JrtoI case 1, in lateral projectionshow ing anomalous origin of right suhclavian arter /rofnt7i des cending aorta. FIGURE 1. Barium esophagram from case 1, in anteroposterior and lateral projections showing posterior impression from retroesophageal aortic arch. FiG URi. 4. Puilmzonary arteriogram from case 2, showing ahs ence o/ the leJt pulmlionaryi, arteryv. Dots outline the courve of a retrograde catheter traversing the anomalous aortic arch into the left ventricle. mentum arteriosum was divided and the esophagus was mobilized. The patient recovered from surgery uneventfully and no longer complains of dysphagia. Discussion FIGURI. 2. Left ventricular angiograni fJrom anteropo.vlerior projection defining the course trathoracic aorta. 1, in the in- case oJ In 1948, Edwards hypothesized that a left-sided aortic arch with a retroesophageal component and a right-sided descending aorta, in conjunction with an CIRCULATION 460 ANOMALOUS RIGHT SUBCLAVIAN ARTERY RETROESOPHAGEAL ARCH IAORTIC 1 . /: - Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 DESCENDING AORTA PULMONARY ARTERY A.SCENDING AORTA FIGURE 5. Illustration of arterial anomaly. anomalous right subclavian artery and a ligamentum arteriosum joining the origin of the right subclavian artery to the right pulmonary artery, could form a vascular ring about the trachea and esophagus3 (fig. 5). Later that year, Paul4 reported two children (ages 7 and 111/2 years) in whom a left-sided aortic arch and descending right-sided aorta were documented for the first time; however, normal origin of the right subclavian artery was present in each case and a complete vascular ring was not present. In 1948, Edwards also reported the autopsy findings from a 17-month-old male who died from small bowel obstruction after abdominal surgery.5 Although that infant had no dysphagia or respiratory distress during life, pathologic examination of the heart and great vessels revealed a left-sided aortic arch with a retroesophageal component, a right-sided descending aorta, anomalous origin of the right subclavian artery and a right-sided ligamentum arteriosum. Since 1948, nine additional cases have been reported in which a leftsided aortic arch has coexisted with a right-sided descending aorta.6"10 Four of the patients were adults, in whom the aortic anomaly was suspected from fluoroscopic examination. Five of these patients were children. Although each had a left-sided aortic arch and a right-sided descending aorta, a symptomatic vascular ring of the type described by Edwards was present in only one of the cases.10 Our cases had a true vascular ring about the trachea and esophagus. The aortic arch arose from the left ventricular outflow tract and coursed leftward, anterior to the trachea, in the normal fashion. Follow- VOL 63, No 2, FEBRUARY 1981 ing a course that was somewhat higher than normal into the upper thoracic cavity, the aorta then coursed posteriorly and to the right behind the esophagus. The esophageal impression from the descending portion of the aortic arch was evident on the barium esophagram. The aorta then coursed inferiorly, descending on the right side of the spine. The great vessel branching pattern was abnormal. The first branch of the ascending aorta was the right common carotid artery, followed by the left common carotid and the left subclavian arteries. The right subclavian artery arose from the descending, right-sided portion of the thoracic aorta. It appeared to arise from a diverticulum-like outpouching of the anterior aortic wall, from which the ligamentum arteriosum also arose. The ligamentum arteriosum attached to the right pulmonary artery and completed the vascular ring about the trachea and esophagus (fig. 5). The left pulmonary artery was hypoplastic in case 1 and absent in case 2. Left pulmonary artery anomalies have not been reported in association with this pattern of aortic arch malformation. The clinical findings in these two cases were suggestive of a vascular ring. The catheterization and angiographic findings detailed the anomalous course of the aortic arch. Because the ductus arteriosus was not patent, all the structures that contributed to the vascular ring could not be visualized angiographically. Hypothetical and autopsy reports by Edwards, however, alerted us to the possibility that these infants' symptoms were caused by this extraordinarily rare condition. These case reports emphasize the complexity and diversity of vascular malformations that may constrict the trachea and esophagus. They also point out the contributions made to clinical medicine by detailed and meticulous studies of the embryology and pathology of congenital malformations. References 1. Binet JP, Langlois J: Aortic arch anomalies in children and infants. J Thorac Cardiovasc Surg 73: 248, 1977 2. Eklof 0, Ekstrom G, Eridsson BO, Michaelsson M, Stephensen 0, Soderlund S, Thoren C, Wallgren G: Arterial anomalies causing compression of the trachea and/or the oesophagus. Acta Paediat Scand 60: 81, 1971 3. Edwards JE: Anomalies of the derivatives of the aortic arch system. Med Clin North Am 32: 925, 1948 4. Paul RN: a new anomaly of the aorta - left aortic arch with right descending aorta. J Pediatr 32: 19, 1948 5. Edwards JE: Retro-esophageal segment of the left aortic arch, right ligamentum arteriosum and right descending aorta causing a congenital vascular ring about the trachea and esophagus. Mayo Clin Proc 23: 108, 1948 6. Heinrich WD, Tamayo RP: Left aortic arch and right descending aorta. Am J Roentgenol 76: 762, 1956 7. de Balsac RH: Left aortic arch (posterior or circumflex type) with right descending aorta. Am J Cardiol 5: 546, 1960 8. Schlamowitz ST, Di Giorgi S, Gensini GG: Left aortic arch and right descending aorta. Am J Cardiol 10: 132, 1962 9. Hastreiter AR, D'Cruz IA, Cantez T: Right-sided aorta. Part 1. Occurrence of right aortic arch in various types of congenital heart disease. Br Heart J 28: 722, 1966 10. Park SC, Siewers RD, Neches WH, Lenox CC, Zuberbuhler JR: Left aortic arch with right descending aorta and right ligamentum arteriosum. J Thorac Cardiovasc Surg 71: 779, 1976 Vascular ring due to left aortic arch and right descending aorta. W Berman, Jr, S M Yabek, T Dillon, J F Neal, B Akl and J Burstein Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 Circulation. 1981;63:458-460 doi: 10.1161/01.CIR.63.2.458 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1981 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/63/2/458 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/