Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
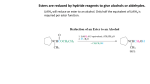
HIGHLY EFFECTIVE AND YET NON-HARMFUL: FUMARIC ACID ESTERS TO FIGHT MS Research made in Bochum: successful treatment of relapsing-remitting multiple sclerosis Ralf Gold, Gisa Ellrichmann and Ralf Linker Multiple sclerosis is a disease for which no cure has yet been found. Its progression may be delayed thanks to new drugs, but the active ingredients in those drugs are either only partially effective or may lead to severe side effects. New discoveries in the field of dermatology have given rise to hope. Researchers in Bochum have discovered that MS symptoms are considerably alleviated through the application of an active pharmaceutical ingredient on the basis of fumaric acid that has long been successfully used against psoriasis. A chronic disease of the central nervous system, the autoimmune disease multiple sclerosis (MS) is the most common neurological cause of disabilities in young adults. At present, the number of MS patients in Germany is calculated to amount to 130,000, with some 70 per cent of them being women. In MS patients, the body’s own immune system attacks the nerve fibres’ “insulating layer” (myelin sheath) and destroys it. Early MS symptoms, so-called episodes, frequently include impairment of visual functions caused by optic neuritis, paralysis of the arms and legs caused by inflammations in the brain or in the spinal cord, and paraesthesia (fig. 1). These episodes last for over 24 hours and are usually treated with cortisone in high doses to encourage remission. In case of severe flare-ups that do not remit after cortisone treatment, patients have the option to undergo plasmapheresis in specialised centres. Typically, all regions of the central nervous system – brain and spinal cord – are affected as the disease progresses. The inflammations result in ataxia, impairment of fine motor skills, as well as concentration loss, bladder function impairment, fatigue and depressive episodes. Disease progression varies from person to person: some 90 per cent of all patients suffer from relapsing-remitting MS, with symptoms initially remitting after an episode. Without proper treatment, the disease evolves into the secondary (chronic) progressive form, where patients experience no symptom relief between episodes. Some 10 per cent of all patients suffer from primary progressive MS, which means they have never experienced symptom relief between episodes (fig. 2). This form of MS affects men and women equally. Despite intensive research into and the development of new therapy methods, there is, as yet, no cure for MS. Nonetheless, considerable progress has been made regarding the treatment of relapsing-remitting MS in the last 20 years. In the 1990s, injectable drugs were released to the market that modulate the immune system: interferon beta and glatiramer acetate reduce the frequency of the episodes by one-third and suppress the formation of new inflammatory foci in the brain and in the spinal cord. As a result, MRI scans (fig. 3 and 4) show 70 per cent fewer newly formed inflammatory foci in patients undergoing this type of treatment. These drugs are not harmful, but at the same time, their efficacy is quite limited. Particularly severe cases are treated with the chemotherapeutic agent Mitoxantron. Originally developed to treat cancer, it may cause severe side effects such as cardiac insufficiency, secondary leukaemia and infertility. Released in 2006, the monoclonal antibody Natalizumab has proved efficient in reducing MS episodes by up to 68 per cent. Biocellular and biomolecular engineering methods are deployed for the production of this antibody that binds to certain structures on the surface of white blood cells, thus stopping them from migrating through vascular walls into inflamed tissue. Consequently, the agent inhibits the leukocytes’ destructive effect that, in case of MS, is directed against the insulating layer of the nerve fibres. But because the destruction of harmful foreign bodies such as viruses and bacteria is what white blood cells are all about, this therapy method results in a weakening of the body’s immune defences. The after effects may include so-called opportunistic viral infections of the brain, such as the frequently fatal progressive multifocal leukoencephalopathy (PML). Available in capsule form, the recently approved drug Fingolimod, which likewise suppresses the immune system, boasts a similar effectiveness; however, here, too, comprehensive measures must be taken to prevent opportunistic infections. In view of all this, the demand for highly efficient and non-harmful immune therapeutics has never faded. There are new grounds for hope, and they derive from a wholly unexpected field: namely dermatology. Here, fumaric acid esters have long been successfully used in psoriasis therapy (info) – likewise an auto-immune disease. Fumaric acid is a fruit acid found in numerous plants, fungi and lichens and an approved food acidulant that also occurs naturally in the human body. In its pure form, the substance is not effective against psoriasis; it is not until the acid is condensed with alcohol that esters are formed which have a therapeutic effect against autoimmune diseases. The application of fumaric acid esters to fight autoimmune diseases has been the result of the collaboration between the dermatology and neurology departments at the RUB clinic St. Josef Hospital in Bochum. It all began when patients suffering from both MS and psoriasis who were treated with fumaric acid esters experienced a remission of their MS symptoms. The physicians at the RUB clinic thus made surprising discoveries regarding the neuroprotective properties of fumaric acid esters. Currently, their therapeutic effect against multiple sclerosis has caused a considerable stir on an international level. A blend of several fumaric acid esters has been available in the German market under the brand name Fumaderm® since the 1990s. The agent is absorbed by the body through the small intestine; small amounts are excreted through urine and faeces. The half-life of the double ester dimethyl fumarate (DMF) is only a few minutes. By splitting enzymes, so-called esterases, DMF is rapidly metabolised into mono-methyl fumarate (MMF) whose half-life in human blood is 60 minutes. A small molecule, MMF can actually permeate the protective blood-brain barrier that separates the brain from various agents: in an experimental model, the local effective concentrations of fumaric acid ester measured in the brain reached up to three micromol that may have a therapeutic effect in the inflamed regions caused by MS. In the field of dermatology, a broad range of immune mechanisms had been researched. It has been postulated that key cells of the immune system, so-called dendritic cells, use fumaric acid ester to process white blood cells (lymphocytes) of the aggressive TH1 type into the TH2 type that modulates immune activity and, in a manner of speaking, soothes auto-aggressive cells through various messenger substances. An autoimmune disease, psoriasis is mediated by the T cells of the immune system, which is why it is reasonable to assume that the symptoms may be reduced or even entirely suppressed if the immune system is reprogrammed. During our initial research into the effect of fumaric acid esters on a disease similar to MS (Experimental Autoimmune Encephalomyelitis, EAE) conducted on mice in an experimental model at the MS Institute in Göttingen in 2004, we observed that the migration of the phagocytes of the immune system (macrophages – microglia) into the mice’s inflamed spinal cord was inhibited to a considerable degree. At the same time, we discovered that the damage to the myelin sheath of neurons (demyelination) was reduced: a larger number of myelin sheaths surrounding nerve fibres remained intact. Eventually, we also demonstrated a higher density of nerve fibres (axons), thus providing an explanation of why mice treated with fumaric acid ester showed less severe symptoms. At that point, the cause underlying these findings was still unclear: we suspected that fumaric acid ester reduced the damage to the nervous system in the first place and, consequently, fewer phagocytes migrated there as “cleaners”. This would indicate that the agent had a protective effect on neurons, in addition to providing immune modulation, as had been postulated in the field of dermatology. This hypothesis was supported by the fact that the number of inflammatory T cells of the immune system was only slightly reduced. Further research showed that protective antioxidant metabolic pathways were triggered in cell cultures through the addition of fumaric acid esters. The transcription factor Nrf2 (nuclear factor derived-E2-related factor 2, fig. 5), a modulatory protein in neurons, acts as the molecular mediator. Typically, this factor is suppressed within the cytosol by its counterpart Keap. By sulphidising Keap, fumaric acid esters dissolve the blockage, allowing Nrf2 to migrate into the nucleus and to trigger a number of antioxidant pathways (fig. 5). These, in turn, neutralise various cytotoxins that are formed due to oxidative stress, for example through so-called free radicals. This is very clearly demonstrated in an experimental model: the process of Nrf2 permeating the nucleus in nerve cells as well as in myelin sheath-forming oligodendrocytes and in astrocytes that surround brain neurons can be observed under the microscope. Thus, it became obvious that nerve cells are protected, as if by a firewall, from inflammatory agents, mainly from free radicals and nitrogen monoxide. The implementation of a protective mechanism in the nervous system through therapeutic measures would constitute a wholly new approach in MS treatment; however, conducting the necessary studies in humans is possible only to a limited extent, and such hypotheses can be only indirectly verified, for example through MRI scans (fig. 3 and 6). Further examinations in experimental models demonstrated, moreover, that fumaric acid esters had a protective effect on nerve cells in patients suffering from Huntington’s, a most severe neurodegenerative disease. In Huntington’s patients, genetic defects lead to cellular metabolism dysfunctions, thus causing nerve cells to die off. In Germany, 10,000 people suffer from this hereditary disease whose progression is unstoppable and which causes severe disabilities that last for the rest of the patients’ lives. Treated with fumaric acid ester, Huntington’s mice with a similar genetic defect live a longer and more active life, and a higher number of neurons survive in them than in untreated Huntington’s mice. Current neuroimmunologic studies have shown that, in EAE, a disease with MS-like symptoms, the effect of fumaric acid esters could be enhanced if they were applied in combination with interferons – chemical messengers of the immune system. Fumaric acid esters also proved effective in the treatment of spontaneously progressing genetic EAE diseases. The then-managing director at the neurology clinic, Prof Dr Horst Przuntek, observed significant MS symptom relief in MS patients who also suffered from psoriasis after they had been undergoing fumaric acid ester treatment carried out by -Bochum-based dermatologists. Accordingly, a small-scale study was conducted with ten patients suffering from relapsing--remitting MS. In the course of 70 weeks, the researchers observed that the frequency of the episodes decreased considerably and that changes typical for MS were reduced by up to 90 per cent, as evident in MRI scans. What followed was a phase 2 dose-finding study (clinical study with several hundred patients) sponsored by Biogen-Idec. The result was: a single dose of the drug has to contain at least 240 mg DMF, also known as ‘BG-12’. Subsequently, phase 3 studies with more than 2,400 patients were conducted, comparing treatment groups of patients who took daily doses of 2 x 240 mg or 3 x 240 mg DMF respectively in form of tablets, as well as control groups of patients undergoing placebo therapy or a proven basic treatment (glatiramer acetate). Fumaric acid esters reduced the episode frequency by up to 50 per cent and the number of active inflammatory foci that were visible in MRI scans by up to 90 per cent. Two daily doses offered results comparable to three daily doses. The side effects of fumaric acid ester treatment include gastrointestinal problems that have been observed in some 20 per cent of patients taking the drugs as part of their dermatological therapy. The reason is: when fumaric acid esters are absorbed through intestinal mucosa, locally irritating inflammatory cytokines are released. Therefore, the BG-12 compound has a delayed-release formula. As a result, gastro-intestinal intolerances occurred considerably less frequently in phase 3 trials than they had done with the dermatological drug, amounting to a mere three to five per cent. Apart from digestive disorders, the second most common side effect was the so-called flush syndrome, which occurred in some 40 per cent of all patients. This reaction is certainly quite unpleasant, but it is by no means dangerous. The symptoms disappear some four to six weeks into the treatment. There was no evidence of any immunosuppressive effects, opportunistic infections or cancerous cell growth such as may develop following a reprogramming of the immune system whose functions include protecting the body from cancer. Blood-counts that were routinely conducted in two-month intervals showed no abnormalities. Highly efficient and yet non-harmful – a wholly new experience in MS therapy! Fumaric acid esters enhance the therapy spectrum for relapsing-remitting MS. The new drugs are an interesting treatment alternative as they combine high efficacy and safety such as have long been achieved with the old formula in the field of dermatology and are supported with data corresponding to more than 150,000 patient years. Moreover, the oral formulation is a relief for many MS patients who have long developed ‘injection fatigue’. Market authorisation being scheduled for spring 2013, the substance will then be ‘officially’ available to patients; at present, the only option are so-called off-label prescriptions. Considering the evidence of their protective efficacy for nerve cells gathered in experiments as described above, it is possible that fumaric acid esters might also prove effective in case of other neurodegenerative diseases for which no treatment has yet been found. A study regarding the application of fumaric acid esters to treat motor neuron diseases, a group of disorders affecting the nerve cells that control locomotion, is forthcoming. Motor neuron diseases include, for example, amyotrophic lateral sclerosis (ALS). It is imperative to conduct individual studies for each and every one of the disorders. Already, we can confidently state that fumaric acid esters have found their way from Bochum into the world of MS therapy! Prof Dr Ralf Gold, Dr Gisa Ellrichmann and PD Dr Ralf Linker (currently Neurological University Clinic, University of Erlangen), Neurological Clinic, St. Josef Hospital, Clinic of the Ruhr-Universität Bochum INFO HISTORY OF FUMARIC ACID ESTERS IN THE FIGHT AGAINST AUTOIMMUNE DISEASES The development of fumaric acid esters as autoimmune disease therapeutics has --been marked by many happy coincidences. It all began when biochemist Dr -Walter Schweckendiek, himself a psoriasis patient, and general practitioner Dr Günther Schäfer postulated the substance’s efficacy in the 1950s and 1960s: in case of autoimmune diseases, the T cells of the immune system require an energy input and what fumaric acid esters do is manipulate the citric acid cycle – a series of biochemical reactions in cells that generates energy. After successful external application of a fumaric acid cream, both researchers went a step further and began developing a variety of fumaric acid ester mixtures which they tested on themselves. In the following years, Dr Schäfer successfully treated numerous psoriasis patients in his surgery, which in those days constituted a huge progress. Bochum-based medical researchers, Prof Dr Peter Altmeyer and Dr Uli Matthes, then took up fumaric acid ester research in the academic context and established the substance firmly as the primary psoriasis therapy method – thus going against the contemporary ‘dermatological mainstream’.