Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
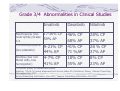
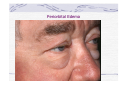
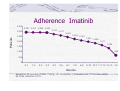
Managing Treatment Related Side Effects Objectives Review common side effects of tyrosine kinase inhibitors used to treat CML Provide practical suggestions for management of side effects Discuss drug-drug interactions Discuss challenges of long-term treatment and strategies to promote treatment adherence TKI Side Effects Side effects vary from person to person. Individuals may tolerate one drug much better than another. Side effects generally increase as dose increases. Management of side effects essential to encourage compliance or adherence. Imatinib Blood Level Testing Excessive side effects may occur if person metabolizes imatinib slowly. Inadequate response if person is a fast metabolizer and imatinib levels low. Can help evaluate potential drug interactions that may increase or decrease imatinib blood levels. Imatinib Blood Levels Imatinib blood levels reported in ng/ml. Trough level, taken 22-24 hours after last dose, lowest blood level of the day. Based on data obtained thus far, the minimum plasma trough concentration goal for imatinib is approximately 1000 ng/mL, somewhat higher acceptable if tolerated. For more information, please refer to Peng B et al. J Clin Oncol. 2004;22:935942; Shmidli H et al. Br J Clin Pharmacol. 2005;60:35-44;Blasdel C et al. imatinib (Glivec)® (imatinib mesylate) Imatinib to Nilotinib, Change in Dosing from with Food to Fasting Imatinib (Glivec) is to be taken with food, once a day unless on 800 mg when taken as 400 mg twice a day. Nilotinib (Tasigna) is to be taken FASTING, every 12 hours: Dose #1: Morning, before breakfast. Dose # 2 Evening, at least 2 hours after eating, then wait at least one hour before eating again. Evening dose more difficult timing for most, may require lifestyle adjustment. Nilotinib (Tasigna) Dosing Example Morning dose Fasting overnight Nilotinib 07.00 Breakfast after 08.00 Evening dose NO food after 17.00 Nilotinib at 19.00 Dinner after 20.00 Myelosuppression-low blood counts Ph-positive Ph-negative TKI In untreated CML, the majority of blood cells are Ph+ cells. TKI eliminates Ph+ cells. Few normal cells left; this therapeutic effect may cause very low blood counts. Grade 3/4 Abnormalities in Clinical Studies Imatinib Dasatinib Nilotinib Neutropenia (low neutrophils) Grade 3-4 17-36% CP 59% AP Thrombocytopenia (low platelets) 9-21% CP 44% AP 4-7% CP 41% AP 46% CP 68% AP 41% CP 71 %AP 18% CP 55% AP 28% CP 37% AP 28 % CP 37% AP 8% CP 23% AP Anemia (low red blood cells, low hemoglobin) CP=chronic phase; AP=accelerated phase. Imatinib: CP=Gr 3/4 newly diagnosed and chronic phase Ifn (interferon) failure; Gleevec Prescribing Information Nov 2007. Sprycel Prescribing Information, Nov 2007; Tasigna, Prescribing Information, Oct 2007 Neutropenia If absolute neutrophil count (ANC) is less than 500, at higher risk for infections. If ANC less than 1000, usually temporarily hold therapy; in patients with advanced disease consider growth factors, G-CSF (filgrastim) or the long acting form, pegfilgrastim so can stay on TKI. Infections not the problem they are with traditional IV chemotherapy. Monitor blood counts weekly or more if neutropenic. Thrombocytopenia-low platelets Can cause excessive bruising or bleeding. No effective drug currently available. With imatinib may take 3 weeks for full effect on platelets, faster and more pronounced drops with dasatinib. If less than 50,000/mm3(50 x 10^9/L), hold therapy and allow counts to recover. With accelerated or blast crisis may allow patients to go down to platelets 20,000/mm3 (20 x 10^9/L); transfusions often needed in blast crisis. Anemia-low red cell counts Anemia can cause fatigue, headaches, shortness of breath. Can treat with ESA’s (erythropoietic stimulating agents) such as erythropoietin or darbepoetin. May need ESA on an ongoing basis to keep hemoglobin (Hgb) up; don’t exceed Hgb 12, use less as counts improve. Use of ESA’s now controversial due to potential adverse effects and high cost. Anemia continued Adequate iron also necessary, check ferritin level, erythropoietin prescribing information recommends ferritin level of at least 100. Oral iron supplements may be needed; iron also well absorbed from red meat. Recent study found intravenous iron can be helpful, use if oral supplements not tolerated. (NCI Cancer Bulletin, vol. 5/no. 8, April 15, 2008). Check B12 and folic acid levels. Transfusions used in extreme cases. TKI dose decrease may be necessary. Non-Hematological Side Effects Imatinib (Glivec) Common Side Effects (all grades, newly diagnosed) Edema (fluid retention) 61.7% Nausea 49.5% Muscle cramps 49.2% Musculoskeletal pain 47% Diarrhea 45.4% Prescribing Information, Novartis November 2007 Rash 40.1% Fatigue 38.1% Headache 37% Abdominal pain 36.5% Vomiting 22.5% Imatinib Serious Side Effects Severe edema, including pleural and pericardial effusions 2-11% Severe CHF (congestive heart failure) and left ventricular dysfunction, <1% Hepatotoxicity (liver) 5%, <1% discontinued treatment Hemorrhage 1.8 % in CP, 11% AP, 19% BC Other severe rare events occur Sprycel (dasatinib) Common Side Effects (All Patients, All Grades) Fluid retention (edema) 37% Diarrhea 31% Headache 24% Nausea 22% Pleural effusion 22% Rash 22% Fatigue 21% Hemorrhage 21% Dyspnea 20% Musculoskeletal pain 14% Dasatinib Prescribing Information, Bristol-Myers Squibb, November 2007. Dasatinib Severe Effects Bleeding and thrombocytopenia (platelet dysfunction in vitro), platelets can drop very quickly, hemorrhage possible, monitor carefully. Fluid retention can be severe, including pleural or pericardial effusion. If develop dyspnea (shortness of breath), do chest x-ray. May occur months into therapy. Side effects less severe at 100 mg once a day dose vs. 70 mg twice a day. Possible prolongation of QTc interval (heart rhythm change). Nilotinib (Tasigna) Common Side Effects Rash 33% Pruritis (itching) 29% Nausea 31% Headache 31% Fatigue 28% Diarrhea 22% Constipation 21% Vomiting 21% Arthralgias (joint aches/pains) 18% Cough 17% Nilotinib Prescribing Information, October 2007. Nilotinib (Tasigna) Other Tasigna can affect the electrical activity of the heart by prolonging the QT interval, time it takes for ventricle to repolarize. Do not use in patients with long QT syndrome. Must correct low potassium, (hypokalemia), low magnesium (hypomagnesemia). Sudden deaths reported (0.6%), may have been cardiac related. Tasigna (nilotinib) Liver Use with caution in patients with hepatic (liver) impairment. Liver enzyme and bilirubin elevations are often transient, resolve with short treatment break. Elevated lipase and amylase may occur. Pancreatitis has also occurred. Hair Hair loss, thinning hair, reported for all three TKI’s; often has other causes. Imatinib--other variable effects: Thicker hair, darker hair, less gray. Others report more gray but also everyone on imatinib getting older! Salon products as desired. Eyes Swelling around the eyes (periorbital edema), usually worst in morning, very common on imatinib. Excessive tearing (imatinib) or dry eyes. Bleeding in whites of eyes (subconjunctival hemorrhages). Blurry vision, particularly with imatinib, probably related to tearing and changes in fluid balance in lens. Periorbital Edema Periorbital Edema Eyes--Management Avoid high sodium (salt) foods. Mild diuretic if necessary, e.g. combination of hydrochlorothiazide and triamterene which conserves potassium. Plastic surgery in severe cases. Eyes--Management Artificial tears, plain Prescription steroid eye drops Subconjunctival hemorrhages (bleeding into whites of eyes). No treatment needed Prevention: Avoid straining, heavy lifting. Diet with plenty of fruits and vegetables (bioflavonoids may decrease platelet fragility) Fluid Retention (Edema) Commonly in hands, feet, legs, hands, occasionally around heart or lungs. Dasatinib--pleural (lung) effusion 22% incidence all grades, less common with 100 mg once daily, ~10%. For pleural effusion may use diuretics, steroids, drainage of fluid (thoracentesis) if necessary, dose interruption and decrease. Nausea and Vomiting Important to take imatinib (Glivec) after a substantial meal; nilotinib (Tasigna) on an empty stomach; dasatinib with or without food. Take imatinib with at least 240 mL of water; eat additional bland food if mild nausea. May help to divide the imatinib dose, e.g. 300 and 300 mg. taken twice a day. Anti-nausea drugs available if necessary, ondansetron, prochlorperazine. Take 1-2 hours before taking TKI. Heartburn More common in patients with a history of dyspepsia or gastroesophageal reflux (GERD). Prevention: avoid overeating, spicy foods Decrease caffeine and alcohol. Elevate head of bed approximately 15 cm using blocks under legs of bed, not pillows. Remain upright sitting or standing 1-2 hours after taking TKI. Heartburn continued Imatinib-consider H2 blockers e.g. famotidine, and proton pump inhibitors (PPI’s), omeprazole or esomeprazole, lowest dose possible. Use of H2 blockers or proton pump inhibitors with dasatinib not recommended. Use antacids instead. Antacids should be given 2 hours prior to or 2 hours after imatinib or dasatinib. Antacids, H2 blockers, or proton pump inhibitors NOT recommended with nilotinib. Diarrhea Increased volume and soft stools common with imatinib. Diarrhea may occur with all 3 TKI’s. Avoid sorbitol, mannitol, maltitol (common ingredients in “sugar-free” foods and gum). Anti-diarrheal medication: loperamide. May be helpful to take ½ or one tablet daily to PREVENT diarrhea. Diarrhea Psyllium seed--increased fiber. Lactase enzyme supplements with milk products if sensitive. Lactose intolerance may occur temporarily after gastrointestinal illness. (Nilotinib and dasatinib contain lactose). Acidophilus to restore normal gut bacteria, particularly after antibiotics. Constipation Extremely rare with imatinib, can occur with dasatinib and nilotinib. Increase fruits and vegetables in diet. Drink adequate oral fluids since dehydration worsens constipation. Stool softeners. Psyllium seed or other fiber. Mild laxatives. Muscle Cramps Most common with imatinib, usually in hands, feet, calves of legs but can occur anywhere. Often helped by calcium, take in divided doses of 500 mg. two to three times a day. Avoid taking at same time as TKI. Calcium citrate more easily absorbed than calcium carbonate which is also an antacid. Potassium supplements as needed, especially if on diuretics. Muscle Cramps Tonic water (quinine) very effective for some. Adequate hydration important in hot weather. Check electrolytes: calcium, potassium, phosphorus and magnesium. Muscle, Joint, Bone Pain May be severe when patients first start therapy, occurs with all 3 TKI’s. Usually resolves within days to weeks, but may persist. May be relieved by non-steroidal antiinflammatory drugs. Rarely short-term opioids are needed. Muscle and Joint Pain Can be difficult to treat when persistent and require change to different TKI because individuals vary in their sensitivity to the individual TKI’s. Check creatine kinase if severe. Consider possible drug interactions, e.g. simvastatin. Bone Pain Recent study used pregabalin 75-300 mg twice daily. Patients reported significantly lower pain scores, improved mood, reduced sleep disturbance and improved qualityof-life. F. Iuliano et al. J Clin Oncol 26: 2008 (May 20 suppl; abstr 18007). Skin Problems--Rash Occurs with all 3 TKI’s. Topical hydrocortisone creams. Stronger steroid creams, e.g. triamcinolone. For severe cases, hold drug and use oral prednisone to control rash, then reinstitute TKI gradually, starting with lower dose. Sometimes rash is a onetime occurrence. Antihistamines. Keep skin moisturized. Mild rashes may be intermittent. Imatinib Associated Skin Rash Other Skin Problems Dry skin, itching—apply moisturizing lotion after bathing; baking soda in bath water, hydrocortisone. Imatinib-Fragile skin that tears easily, usually after long-term use. Protect skin with clothing. Imatinib-Changes in skin pigmentation, lighter, more noticeable in dark skinned people. Sun sensitivity-use sunscreen and protective clothing, hats. Sunburn with imatinib can be severe. Fatigue Occurs with all 3 drugs. Correct anemia if present. Check thyroid function. Moderate regular exercise, starting very gradually, often helpful. Rest before exhaustion, otherwise takes a long time to recover. May need daily nap. Fatigue continued Pace and prioritize activities. Counseling, stress management, meditation, yoga can be helpful. Fatigue often improves but may persist. Treat depression and anxiety which can contribute to fatigue. May be associated with memory loss, difficulty concentrating. Weight Gain Weight loss common before CML diagnosis. Metabolic rate drops once out of control white cell production stopped, weight gain then likely. Some patients report increased appetite on imatinib. To avoid weight gain, decrease calorie intake and get more exercise. Decrease sodium (salt) intake to minimize fluid retention. Drug Interactions Imatinib, dasatinib, and nilotinib metabolized via CYP3A4 pathway, inhibitors. CYP3A4 inhibitors may INCREASE TKI plasma concentration (blood level), Cmax and AUC. CYP3A4 inducers may DECREASE TKI plasma concentration (blood level), Cmax and AUC. If one of these drugs must be used, can increase or decrease dose of TKI accordingly, but usually possible to instead substitute another drug. Drug Interactions Examples Imatinib, Dasatinib, Nilotinib Increase Plasma Concentrations TKI’s Ketoconazole Itraconazole Erythromycin Clarithromycin Decrease Plasma Concentrations TKI’s Dexamethasone Phenytoin Carbamazepine Phenobarbital Rifampin Rifapentine St. John’s Wort Plasma Concentrations Altered by TKI’s Simvastatin Cyclosporine Pimozide Triazolobenzodiazepines Dihydropyridine calcium channel blockers Warfarin Acetaminophen Drug Interactions continued For list of CYP3A4 substrates, inhibitors and inducers, by entering “CYP3A4” at wikipedia.com. Prescribing information recommends NOT using warfarin with imatinib, avoid with nilotinib, and use caution with dasatinib. Patients requiring long-term anti-coagulation may not be able to use low molecular weight heparin as a practical matter. Monitor INR carefully if on warfarin. Drug Interactions Acetaminophen (paracetamol) should be limited to 2000 mg. per day, and avoid completely if liver enzymes elevated. Use caution with drugs that irritate the stomach or increase bleeding risk, e.g. ibuprofen. Herbals St. John’s Wort (hypericum) decreases TKI levels unpredictably—patients may think it is safe because it is “natural.” Many herbs have interactions with TKI’s, local usage and names vary, vital to check with doctor or pharmacist before taking these. Food Interactions Do not take TKI’s with grapefruit juice as may unpredictably increase blood levels. Avoid star fruit, Seville oranges. Black mulberry, wild grape, pomegranate, black raspberry juice may also affect metabolism. Surgery--General Considerations For imatinib, consider holding it 72 hours prior to surgery to prevent any possible interactions with anesthesia, drugs needed in emergencies. Dasatinib and nilotinib hold 48 hours prior. Generally can resume TKI as soon as able to eat and drink normally and recovery going well. QTc Prolongation Nilotinib--avoid drugs that cause a prolonged QTc interval. Monitor EKG’s if dose changed or new drugs added. Dasatinib--use caution. List of drugs causing QTc prolongation is extensive: anti-arrhythmics, haloperidol, erythromycin etc. List available at www.torsades.org. Summary All 3 TKI’s well-tolerated compared to traditional chemotherapy and interferon. With aggressive side-effect management, most patients have good quality of life. Side effects generally decrease over time. Long-term effects --Due to animal studies with imatinib, long term monitoring of liver, urinary tract function recommended. Longterm effects of dasatinib and nilotinib unknown. Oral Therapy Considerations Compliance or adherence and persistency are issues with all three TKI’s. CML is a chronic disease that requires ongoing daily therapy. Limited opportunities and mechanisms to counsel patients on oral therapy, not in clinic as much as if on intravenous therapies. Source: Novartis Oncology, 2004. Oral Therapy Considerations Reasons for non-adherence included drug cost (full dose too costly), feeling treatment was unnecessary because patients felt well, psychosocial factors, and using a different dosage than prescribed in an attempt to manage side effects. Aoki E, et al. J Clin Oncol. Proceedings of the 42nd Annual Meeting of the American Society for Clinical Oncology (ASCO), June 2-6, 2006, Atlanta, GA; Part 1, Vol. 24, No. 18S (June 20 Suppl):6506. Cortez JE, et al. Hematol Oncol Clin N Am. 2004;18:619-639. Novartis Survey, 2004. Dosing imatinib (Glivec)® for Optimal Results in Chronic Myeloid Leukemia, Novartis Oncology, 2004. Pharmacy Record Analysis of 4043 Patients Prescribed imatinib (Glivec) Patient adherence with imatinib (Glivec) therapy estimated at 75%. Dramatic decline in persistency over time(looking at individual patients): • Month 4: near 100%. • Month 5: 94%. • Month 14: 23%. Nonadherence can compromise therapeutic outcomes; this data in line with studies done with other drugs used to treat serious chronic diseases. 1. Tsang J-P, Rudychev I, Pescatgore SL. Poster presented at: The American Society of Clinical Oncology Meeting. 2006. 2. Partridge AH, Avorn J, Wang PS, Winer EP. J Natl Cancer Inst. 2002;94:652-661. Adherence Imatinib 3,500 2,921 2,913 2,908 2,883 Patients 3,000 2,742 2,617 2,448 2,269 2,500 2,126 1,997 1,866 1,671 2,000 1,368 1,500 685 1,000 500 0 0-1 1-2 2-3 3-4 4-5 5-6 6-7 7-8 8-9 9-10 10-11 11-12 12-13 13+ Months Based The typical on 14 persistency months of curve data, Tsang, drops off J-P, at 1-2 Rudychev months. I, Pescatore SL. J Clin Onc. 2006; 24:330s. Abstract 6119. Adherence by Gender-Age 92% 90% 90% 89% 87% 88% Avg. Compliance 89% 88% 87% 86% 86% 85% 84% 87% 84% 84% 81% 82% 80% 78% 76% <25 F <25 M 25-35 F 25-35 M 35-45 F 35-45 M 45-55 F Gender-Age 45-55 M 55-70 F 55-70 M >70 F >70 M Non-adherence and costs Retrospective analysis of claims of 267 patients with CML in US, analyzed imatinib refill data. Medication possession ratio (MPR) for imatinib 77.7%. 20% had MPR of <50%. 31% had treatment interruption of at least 30 days. Lower MPR levels in women, those with multiple concomitant medications, higher starting dose of imatinib, high disease complexity. Lower MPR resulted in higher annual healthcare costs. Darkow T et al. Treatment interruptions and non-adherence with imatinib and associated healthcare costs. Pharmacoeconomics 2007, 25(6): 481496. Strategies to Improve Adherence • Encourage patientphysician communication • Multidisciplinary team approach that includes the patient • Encourage establishing a routine way to take doses • Educate patients to take medications as prescribed and why this is important • Use routine monitoring to engage patients, review progress, and monitor compliance • Manage side effects proactively Promoting Adherence Most patients do best if they take their CML medication in conjunction with something they habitually do every day. Helpful to use pill container, calendar or chart to mark doses taken. Carry extra doses especially when traveling. Trust Trust between health care provider and patient is crucial. Studies show adherence to treatment depends on whether health professional was viewed as an ally in cooperation with patient. Dimateo MR. Variations in patients’ adherence to medical recommendations: a quantitative review of 50 years of research. Med care. 2004; 42:200-208. Please check with your physician before taking any medications suggested in this guide.