Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
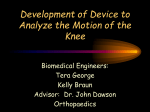
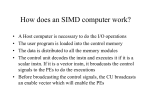
Medicine exam 2013/14 Course title: 5.2 Nervesystemet og bevægeapparatet II (Neurology II) Programme: Bachelor in education Semester: 5th semester Exam date: 20-02-2014 Time: 09:00-13:00 Evaluation form 7-point scale Important information: Remember to bring your student identification card Remember to put your student number – not your name and cpr no – on all sheets that you hand in for evaluation (if written exam) Remember to hand in the assignment if you leave the exam before it has ended No written aid is allowed Your paper must be handed in on paper in hand written form Quicktionary pen is allowed (no other electronic devices are allowed) The study board/the university cannot be held liable if any problems should occur regarding the electronic aid during the examination It will be considered cheating or attempting to cheat if the technical equipment of the student is communicating or trying to communicate with other equipment not relevant to the exam, without an explicit permission. Before the beginning of the exam, the student should make sure that all communication devices in the equipment at the exam are turned off. Communication is not allowed Answers both in Danish and English allowed. Point system (7-scale, max: 206 Points, 60%: passed (123.5 P)): Passed: 12 (206-191.5); 10 (191-174,5); 7 (174-157.5); 4 (157-140,5); 2 (140-123.5); Failed: 0 (123-61.5); -3 (61-0) Student number 1. Epilepsy/seizures (30 Points) a) Give a brief definition for epilepsy and seizure as well as an overview of main 5 characteristics each (7 Points) b) Give 4 examples for simple partial seizure symptoms. Give 4 examples for complex partial seizure symptoms. The examples should include short descriptions. (8 Points) c) State 2 different treatment options via AED/anti-epileptic drugs. This should include pharmacological examples!!! (4 Points) a) Def./characteristics seizure: Are time-limited paroxysmal events/Result from abnormal, involuntary, rhythmic neuronal discharges in the brain./Are not predictable./Can occur at inconvenient, embarrassing, or even dangerous times./Unpredictability is the most distressing aspect of epilepsy./Are usually short, lasting less than 5 minutes./Can be preceded by a prodromal phase/Can be followed by a long postictal phase, during which there is gradual return to baseline. Def./characteristics epilepsy: Epilepsy is a disease characterized by spontaneous recurrence of unprovoked seizures. Epileptic syndromes are defined by many factors, including: Type of seizure/Age at onset of seizures/Family history/Findings at physical examination/Ictal and interictal electroencephalography (EEG)/Neurological imaging b) Simple partial seizures: Somatosensory: tingling of contralateral limb, face, or side of the body/Focal Motor: tonic-clonic movements of upper (lower) limb/Grimacing/Controversive: head +eyes turned to opposite site/Visual: seeing flashes of light, scotomas, uni- or bilateral blurring/Auditory: Hearing ringing, hissing or noise/Autonomic: sweating, flushing or pallor, and/or epigastric sensations Complex partial: Impairment of consciousness: cognitive, affective symptoms; Dreamy state; blank, vacant expressions; déjà vu, jamais vu, or fear/ Formed auditory hallucinations: hears music etc./Formed visual hallucinations: sees houses, trees … that are not there/ Olfactory hallucinations: bad or unusual smell/Psychomotor phenomena: Chewing movements, wetting lips, automatisms (picking at clothing) d) AED/anti-epileptic drugs convential examples: carbamazepine, clonazepam, lrorazepate, valproic acid, ethoxusimide, phneytoine … new examples: felbamate, gabapentine, lamotrigine, tiagabine, … unconventional examples: ACTH, acetazolamide, amantadine, … MoA: enhancing GABA-mediated synaptic inhibition (pre-/post-synaptic); examples/post-synaptic: benzodiazepines, barbiturates examples/pre-synaptic: vigabatrin, valproate, tiagabine promoting inactivation state of Voltage-gated Na+ for limiting sustained, repetitive neuronal firing; examples: carbamazepine, phneytoine, valproate 1 Student number limiting activation of voltage-activated T-Type Ca (T currents); examples: valproate/ethoxusimide 2 Student number 2. Ear/Inner ear/posture & balance (29 P) a) Fill in the missing labels (8 P) b) Describe which semicircular canal is responsible for which sense in terms of “direction of head movement”. (3 P) c) Describe the purpose of the horizontal vestibulo-ocular reflex. Describe as well excitatory and inhibitory connections (reflex arcs) within this reflex (drawing possible). (14 P) d) Fill in the missing labels. (4 P) a) b) Posterior canal: head tilt / left vs. right Superior Canal: nodding (yes) Horizontal canal: head shake (no) 3 Student number c) The vestibulo-ocular reflex (VOR/oculocephalic reflex): reflex eye movement; stabilizing images on the retina during head movement by producing an eye movement in the direction opposite to head movement, thus preserving the image on the center of the visual field (e.g. the head moves to the right, then eyes move to the left). Slight head movement is present all the time: the VOR is very important for stabilizing vision; VOR independent from visual input/works even in total darkness or eyes closed. 4 Student number d) 5 Student number 3. Cranial nerves (27 P) a) Name the cranial nerves X, XI and XII and give a very short description of their component fibers (mixed, purely sensory/motor, etc.), functions and structures that are innervated. (12 P) b) What are the three branches of the cranial nerves V? Where do these branches exit from the skull? (6 P) c) Give 3 possible signs of a cranial nerve III nerve lesion (+ name of the nerve) Which clinical testings are performed routinely? (6 P) d) Double vision can be the clinical sign for which damaged cranial nerve(s)? (3 P) a) X/N. vagus; mixed; motor/GVE: smooth muscle & glands in pharynx, larynx, thoracic/abdominal viscera; M. palatoglossus, soft palate, larynx, pharynx; sensory: taste from epiglottis, pharynx; larynx, laryngopharynx, auricle, diaphragm; external acoustic meatus; aortic baro-/chemoreceptors, esophagus, bronchi, lings, heart, … XI/N. accessorius: motor; innervates M. sternocleidomastoideus/trapezius XII/N. hypoglossus; motor; innervates M. hyoglossus/genioglossus/styloglossus/all intrinsic tongue muscles b) V1/N. ophthalmicus; superior orbital fissure V2/N. maxillaris; foramen rotundum V3/N. mandibularis; foramen ovale c) N. occulomotorius; ptosis/mydriasis/double vision (diplopia)/outward deviation of the eyeball/impairment of accommodation; clinical tests: pupillary light reflex+following object with the eye; (1 point each) d) diplopia/double vision: N. occulomotorius/III; N. trochlearis/IV; N. abducens/VI 6 Student number 7 Student number 4. Psychological aspects of pain (22 P) a) Give a definition of pain according to the IASP (International association for the study of pain). What is the relation between nociception and pain (define nociception as well!)? (5 P) b) Elaborate briefly on the impact of the gate-control theory on the understanding of psychological aspects pain. (6 P) c) Name 4 components of pain. (4 P) d) How can you “quantify” pain? Give three options. (3 Points) e) Define the terms “operant (instrumental) conditioning and “classical conditioning”. Give one short example each. (4 Points) a) Def. Pain: “unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage” Def. Nociception: neural processing of afferent input from nociceptor Usually, nociception leads to pain: the higher the amount nociceptor activation & nociceptive transmission, the higher the pain perception; BUT: Nociception without pain perception possible Pain perception without nociceptive transmission possible b) Gate control theory: “gating” synaptic transmission/neuronal cross talk (based on “touch inhibits pain”/inhibitory interneuron action of ascending nociceptive input). More than 1 gate postulated: amongst others (tactile afferent input activating inhibitory interneurons; Spinal modulation/Lamina via descending tracts before ascending transmission enters the spinothalamic tract from e.g skin). Principal proposed gates: physical (opening: injury; closing: medication, touch), emotional (opening: anxiety; closing: happiness), behavioral (opening: attention; closing: distraction) The DCT enabled the inclusion of factors beyond physiology (psychology) in the better/broader understanding of pain. c) Sensory-discriminative Emotional affective Autonomic Cognitive Motor (Psychomotor) d) Psychophysiology/Verbal Rating Scale (VRS)/Visual Analogue Scale (VAS), nociceptive physiology (anything that can objectively be measured such as evoked potentials, nociceptive reflexes, …), psychology (Questionnnaires) e) operant: reinforced individual response to pain by showing pain behavior (pity/partner) classical: Associating a particular environment with pain experience; dentist 8 Student number 9 Student number 5. Mixed topics (36 P) a) Response of a photoreceptor to light/Phototransduction: Describe the state of the photo receptor in the dark (3 P) b) Response of a photoreceptor to light/Phototransduction: Give the steps involved in conversion of light energy into electrical signals. (5 P) c) Describe out of which 2 “portions” intraocular fluid consists of and where to find them. What is the normal range for intraocular pressure? (5 P) d) What are the main parameters of the Glasgow Coma Scale (GCS)? What can you use the GCS for in general? Give one example where to use the GCS routinely. (5 P) e) What are the modes of action for: methotrexate, etanercept, acetylsalicylic acid? (3 P) f) Neuromuscular blocking agents: What have the substances hemicholinium and botulinum toxin in common and what are there differences? What have the substance mivacurium, atracurium and acuronium in common and what are the differences? (7 P) g) Anaesthesia Describe briefly what the main neurophysiological changes are caused by general anaesthesia. What are the main 2 effects of general anaesthesia on a cellular level? What is the main difference between Ether, Halothane and Nitrous oxide when it comes to induction/recovery speed? (8 P) 10 Student number a) 1. cGMP levels in cytosol are high/ 2. Na+ channels are open/ 3. Na+ enters cell causing depolarization – spreading from outer segment to the terminal/ 4. Ca++ channels open due to depolarization/ 5. Ca++ enters the cell – triggering transmitter exocytosis/ 6. Transmitter causes graded potentials in bipolar cell (0.5 P each) b) 1. Light absorption in photopigment/ 2. Retinal and opsin dissociate/ 3. Activation of transducing/ 4. Activation of phosphodiesterase/ 5. cGMP in cytosol decrease/ 6. Less Na+ entering the cell: cell hyperpolarizes/ 8. Ca++ channels close/ 9. Decreased transmitter release/ 10. Graded potential in bipolar cell gets smaller (0.5 P each) c) aequous (in front of lens) + vitreous (between lens and retina) humor 12-21 mmHg (1 P each) d) main parameters: Eye opening (spontaneous/to voice/to pain/ no response), Verbal response (Oriented/confused/inappropriate words/incomprehendable sounds/no response), Motor response (Follows commands/ purposeful, localizes/ Withdraws to pain/ abnormal flexion (decorticate)/ abnormal extension (decerebrate)/ No response) GCS: assess level of consciousness after head injury Use: first aid, doctors, nurses, for medical and trauma patients/chronic patients.(1 P each) e) MoA: - Methotrexate: Folic acid antagonist, cytotoxic and immunosuppressant/ ↓ purine metabolism enzymes/ ↓ T cell activation - etanercept: TNF-alfa binding recombinatnt fusion protein (TNF-Fc domain fused to human IgG molecule) - acetylsalicylic acid: Cox-1/Cox-2 peroxidase inhibitor (PGH2 synthase) (1 P each) f) hemicholinium/botulinum: in common: pre-synaptic neuromuscular blocking agents; difference: hemicholinium/ affects choline re-uptake; botulinum/ affects acetylcholine release 3P mivacurium, atracurium and alcuronium: in common: stabilizing/non-depolarizing neuromuscular blocking agents difference: Short/intermediate/long-acting (in that order!!!) 4P g) GA: unconsciousness/ loss of response to painful stimulation/ loss of reflexes 3P Main effects: ↓ transmitter release, ↓ postsynaptic response 2P Ether, Halothane and Nitrous oxide: slow/medium/fast (in that order!!!) 3 P 11 Student number 6. Lower extremities (33 P) a) Give the name of the tarsal bones. (7 P) b) Which are the ligaments of the articlatio talocruralis and what are their main functions? (7 P) c) Name the stabilizers of the transverse foot arch (4 P) d) Summarize the main differences between Pes rectus, Pes planus, Pes cavus and Pes transversoplanus. (4 P) e) Describe the structures within the fossa poplitea (cf. figure)! (7 P) f) Name and briefly describe 2 tests for the ACL (anterior cruciate ligament). 4 P 12 Student number a) talus/ calacaneus/ cuboideum/ naviculare/ cunieforem mediale+laterale+internmedium b) Medial: Lig. deltoideum (Pars tibiotalaris anterior + posterior/ tibionavicularis/ tibiocalcanea); function: resists excessive eversion Lateral: Lig. Collaterale (Lig. Talofibulare anterius + posterius/ calcaneofibulare); Lig. Tibiofibulare anterius + posterius; function: resist inversion c) Lig. metatarseum transversum profundum/ M. adductor hallucis - metatarsal arch/ M. fibularis longus/ M. tibialis posterior/ d) Pes rectus: normal plantar arches Pes planus: loss of longitudinal arch Pes cavus: increased height of longitudinal arch Pes transversoplanus: loss of transversal arch e) 1 Biceps femoris 2 Semimembranosus 3 Semitendinosus 4 Gracilis 5 Sartorius 6 medial head of gastrocnemius 7 lateral head of gastrocnemius 8 adductor hiatus 9 popliteal artery 10 anterior tibial artery 11 peroneal artery 12 posterior tibial artery 13 tibal nerve 14 common peroneal nerve F) Pivot-Shift Test: Anterolateral instability of the knee/ Person lies on one side of the body/ Knee is extended and internally rotated/ Stress applied to lateral side of the knee, while the knee is being flexed/ A crash felt at 30 degrees flexion indicates positive test. Lachman’s Test: Knee is flexed at 30 degrees/ Pulls on the tibia to assess the amount of anterior motion of the tibia in comparison to the femur./ ACL-deficient knee will demonstrate increased forward translation/ of the tibia at conclusion of movement. Anterior Drawer Test: Patient lying supine, the hip flexed to 45°, knee to 90°/ Examiner in front of the involved knee/ Grasping the tibia just below the joint line of the knee./ Thumbs placed along the joint line on either side of the patellar tendon. / Palpating hamstring tendons with index fingers to ensure that they are relaxed; hamstring muscle group must be relaxed to ensure a proper test./ Tibia is drawn forward anteriorly./ Increased amount of anterior tibial translation vs. opposite limb or lack of a firm end-point indicates either a sprain of the anteromedial bundle of the ACL or a complete tear of the ACL./ This test should be performed along with other ACL-specific tests to help obtain a proper diagnosis. 13 Student number 7. Upper limb (32 P) a) Name the proximal and distal carpal bones. At which bone do most frequently occur fractures and at which one dislocations? (10 P) b) Name 3 primary grip types of the normal hand. (3 P) c) According to the “Verdan Extensor Tendon Injury Calassification System”, extensor tendon injuries can be classified in 8 different zones? What are these 8 zones? At which zones do the “Mallet finger” and “Boutonnier’s deformity” occur? (10) d) Describe briefly the cause of the “de Quevain’s disease”. (4 P) e) Name the hypothenar muscles. Which nerve innervates them? (5 P) a) Proximal: Scaphoid (most common fractures)/ Lunate (most common dislocated)/Triquetum/ Pisiform (acts: ossa sesamoideum) Distal: Trapezium (aligns with 1st metacarpal)/ Trapezoid (2nd metacarpal)/ Capitate (3rd metacarpal)/ Hamate (4th & 5th metacarpal) b) Pinch or precision grip/ Power grip/ Key grip/ Hook grip c) 1: DIP 2: middle phalanx 3: PIP 4: proximal phalanx 5: MCP 6: metacarpals 7: carpals 8: proximal wrist “Mallet finger”: I-II; Boutonnier’s deformity”: II-IV; d) de Quevain’s disease: Stenosing tendovaginitis of the first dorsal extensor compartment/ The two tendons concerned are the tendons of the extensor pollicis brevis and abductor pollicis longus muscles; Tendovaginitis /stenosing tendovaginits: Tendon constriction in narrow fibro-osseus canals; Fibrocartilaginous metaplasia & thickening of sheath e) Opponens digiti minimi/ Flexor digiti minimi/ Abductor digiti minimi/ Palmaris brevis; N. ulnaris 14