Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
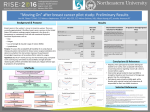
1 The importance of education on breast cancer related lymphedema Pinar Borman MD, Aysegul Yaman MD, Sina Yasrebi MD, Oya Özdemir MD, Alp Çetin MD. University of Hacettepe Faculty of Medicine Department of Physical Medicine and Rehabilitation, Sihhiye, Ankara, Turkey, 06100. Coorespondence: Prof. Dr Pınar Borman Hacettepe University Medical Faculty Dept of PMR, Ankara, Turkey e-mail: [email protected] phone: 90.312.3094142 fax: 90.312.4186363 2 Introduction Improvements in early detection and treatment of breast cancer have led a growing number of survivors. The maintenance of overall health and quality of life are major concerns since side effects of cancer treatments may arise and can result in significant long term physical and psychological disabilities (1,2). Lymphedema is an abnormal accumulation of protein-rich fluid within the intertistial tissue that can occur after breast cancer surgery or radiation therapy. Lympedema affects up to 50% of breast cancer patients and substantially increase their postoperative medical costs. The prognosis for these patients, is worse and treatment is more costly when the lymphedema is not diagnosed and treated in the earlier stages. Although breast cancer related lymphedema can lead to physical emotional and psychological challenges and impaire quality of life, it is under-recognized and under- treated (3,4). Therefore the awareness of the condition and sufficient education of the breast cancer survivors are of great importance. Recent studies have shown a general lack of knowledge and awareness regarding lymphedema risk and risk reduction guidelines (5-12). Previous studies have also indicated that patients’ knowledge and education were shown to be correlated with risk of developing the condition (8,9,12). We aimed to determine the knowledge and education of breast cancer patients who referred to a tertier university hospital, Physical Medicine and Rehabilitation (PMR) Department for lymphedema rehabilitation. MATERIALS AND METHODS Participants were all women and recruited from PMR department among the breast cancer survivors who were admitted for diagnosis and or treatment of lymphedema between June 2013 and April 2014. The demographic and clinical characteristics including age, literacy, duration of surgery, type of surgery, body mass index, duration and site of lymphedema, stage of lymphedema were recorded. Each participant was asked to complete a survey to assess lymphedema status, knowledge and education about lymphedema and we also aimed to determine the related factors with lymphedema in their first visit. The duration of lymphedema, the site of lymphedema (proximal, distal), the grade of lymphedema (subclinic, reversible, spontaneous irreversible, elephantiasis), the stage of lymphedema according to girth measurements (stage 1,2,3), were recorded. The positivity of Stemmer sign was checked. 3 The patients responded to questions in the survey, asking whether they have received information about awareness of lymphedema or whether they have educated for reducement of the risk of lymphedema after the breast cancer surgery. The patients were answered as yes or no. In addition quality of life of the patients was assessed with EORTC Quality of life Questionnaire Breast cancer module (EORTC-QOL-C30) (13) questionnaire and functional status was determined by Disabilities of Arm Shoulder and Hand (DASH) (14) questionnaire. All the assessments were performed by an experienced lymphedema specialist. The study was approved by the institutional ethical board. Statistical analysis: Descriptive statistics were expressed with mean +standard deviation, median and percentage values. Groups were compared with student’s t test or Mann Whitney U test or chi square analysis. All tests of statistical significance were two sided and considered statistically significant at p<0.05. Analyses were conducted by SPSS 13.0 statistical package. RESULTS Seventy-one patients who had admitted to lymphedema rehabilitation unit between June 2013 and April 2014, were recruited to the study. All patients were women. The mean age and duration of surgery were 52.03+9.9 years (28-77) and 32.8+27.6 months (-). Most women were diagnosed with mild to moderate stage breast cancer 41 (57.7%) patients had grade 1, 27 (38%) patients had grade 2 and 3 (4.2%) patients had grade 3 lymphedema. Among the participants, only 15 (21.1%) had reported that they have received information or education about lymphedema. 56 patients (78.9%) did not informed or trained about the development of lymphedema. The demographic and clinical characteristics in regard to lymphedema knowledge and, education, are shown in Table 1. The degree of lymphedema according to girth measurements, and duration between breast cancer surgery and lymphedema were lower in patients that have informed or educated about lymphedema as compared to the patients that have not been informed (p<0.05). Also the number of patients having pitting edema and having pain in the area of lymphedema were higher in patients that did not DISCUSSION Our intervention was designed to identify the level of awareness and education about breast cancer related lymphedema in survivors, admitted to a tertiary university hospital in a 4 developing country. The frequency of postoperatively educated patients about the risk of lymphedema was only 21%. The educated patients have a delayed progression of lymphedema and lower stages than in patients lacking awareness of lymphedema. Also the educated patients shortly after their surgery had higher quality of life scores indicating a nonimpaired wellbeing. Previous studies have assessed lymphedema knowledge or awareness and reported average to low knowledge levels (5-9,15). Bosompra et al measured lymphedema awareness and reported higher scores of awareness among the patients reporting swelling compared with subjects having no swelling (15). Lee et al conducted a study assessing lymphedema knowledge by asking prevention and care about lymphedema to breast cancer survivors and found a high rate of patients having lymphedema knowledge, contrary to our results (16). This difference can be explained with cultural and developmental degree of different populations. A more recent study reported that women who received lymphedema information had higher knowledge scores and lower lymphedema symptoms compared to those who did not receive information, again resembling our data (17,18). These results suggest that approaches to lymphedema education can be potentially beneficial in improving awareness on lymphedema risk and risk reduction strategies among breast cancer patients diagnosed and treated in surgery wards (8,10,18). The small study group and a cross sectional design of the study, are the limitations of our study. Also the non quantitative assessment of lymphedema knowledge may also be considered as another limitation. But as far as we have known this is the first study evaluating the knowledge about lymphedema among breast cancer survivors in our region which may highlighten the unmet need for education in a developing country for the awareness of lymphedema and may lead to improve health care delivery settings in order to enhance the quality of life of these patients. In conclusion there is a lack of awareness of the lymphedema or risk of lymphedema, and an unmet need sufficient education and knowledge among breast cancer survivors, especially in developing countries. We believe that education programs about lymphedema and risk reduction methods after the breast surgery are strongly needed. There is also a need for the continuing education of health care providers and surgeons for the importance and early diagnosis of lymphedema in order to better inform and educate breast cancer survivors and their families. Future studies comparatively assessing lymphedema knowledge and 5 monitoring effects of education between different cultures will enhance the experiences and will help to standardize this education in developing countries. REFERENCES 1. Lawenda BD, Mondry TE, Johnstone PA. Lymphedema: a primer on the identification and management of a chronic condition in oncologic treatment. CA Cancer J Clin 2007;57:43-66. 2. Rourke LL, Hunt KK, Cormier JN. Breast cancer and lymphedema: a current overview for the healthcare provider. Omen’S health 2010;6(3):399-406. 3. Shah C, Arthur D, Riutta J, Whitworth P, Vicini FA. Breast-cancer related lymphedema: a review of procedure-specific incidence rates, clinical assessment aids, treatment paradigms and risk reduction. Breast Journal 2012;18(4):357-61. 4. Gartner R, Jensen MB, Kronborg L, Ewertz M, Kehlet H, Kroman N. Self-reported arm-lymphedema and functional impairment after breast cancer treatment- a nationwide study of prevalence and associated factors. The Breast 2010,19:506-15. 5. Radina ME, Armer JM, Culbertson SD, Dusold JM. Post breast cancer lymphedema: understanding womens’ knowledge of their condition. Oncol Nurs Forum 31(1):97104. 6. Gray RE, Fitch M, Grenberg M, Hampson A, Doherty M, Labrecque M. The information needs of well, longer term survivors of breast cancer. Patient Educ Couns 1998;33(3):245-255. 7. Runowicz CD. Lymphedema: patient and provider education: current status and future trends. Cancer 1998;83(suppl12):2874-2876. 8. Ridner SH. Pretreatment lymphedema education and identified educational resources in breast cancer patients. Patient Educ Couns 2006;61(1):72-79. 9. Fu MR, Chen CM, Haber J, Guth AA, Axelrod D. The effect of providing information about lymphedema on the cognitive and symptom outcomes of breast cancer survivors. Ann Surg Oncol 2010;17(7):1847-1853. 10. Paskett ED, Stark N. Lymphedema: Knowledge, treatment and impact among breast cancer survivors. Breast J 2000;6(6):373-78. 11. Greenslade MV, House CJ. Living with lymphedema: a qualitative study of women’s perspectives on prevention and management following breast cancer related treatment. Can Oncol Nurs J 2006;16(3):165-179. 6 12. Kwan ML, Shen L, Munneke JR, Tam EK, Partee PN, et al. Patient awareness and knowledge of breast cancer related lymphedema in a large,integrated health care delivery system. Breast Cancer Res Treat 2012;135:591-602 13. Demirci S, Eser E, Ozsaran Z, Tankısı D, Aras AB, et al. Validation of the Turkish versions of EORTC-QoL-C30 and BR23 modules in breast cancer patients. Asian Pacific J Cancer Prev 2011;12(5):1283-7. 14. Koldas-Dogan S, Ay S, Evcik D, Baser O. Adaptation of Turkish version of the questionnaire of the Quick disability of the arm, shoulder and hand (Quick DASH) in patients with carpal tunnel syndrome. Clin Rheumatol 2011;30:185-91. 15. Bosompra K, Ashikaga T, O’Brien PJ, Nelson L, Skelly J, Beatty DJ. Knowledge about preventing and managing lymphedema: a survey of recently diagnosed and treated breast cancer patients. Patient Educ Couns 2002;4782):155-163. 16. Lee YM, Mak SS, Tse SM, Chan SJ. Lymphedema care of breast cancer patients in a breast care clinic: a survey of knowledge and health practice. Support Care Cancer 2001;9(8):634-641. 17. Nielsen I, Gordon S, Selby A. Breat cancer realted lymphedema risk reduction advice: a challenge for health professionals. Cancer Treat Rev 2008;34(7):621-628. 18. Tam EK, Shen L, Munneke JR, Ackerson LM, Partee PN, et al. Clinician awareness and knowledge of breast cancer related lymphedema in a large, integrated health care delivery setting. Breast Cancer Res Treat 2012;131:1029-1038. 7 Table 1: The demographic and clinical characteristics of the patients in regard to lymphedema education Age (years) (mean+SD) BMI (kg/m2) (mean+SD) Education illiterate Primary Secondary-lycee university Duration of surgery (mean+SD) (years) smoking Surgery Mastectomy Radical mastectomy Modified radical lumpectomy Duration of lymphedema (month)(mean+SD) Site of lymphedema Proximal distal Pitting Positive negative Pain in area of lymphedema Positive negative Type of lymphedema Subclinical Reversible Spontaneous irreversible elephantiasis Stage according to girth measure 1 2 3 Stemmer sign Positive negative Duration between surgery and lymphedema (mean+SD) median DASH EORTC-QOL-30 (global health) Patients educated for lymphedema (n=16) 48,44± 9,187 29,58± 4,60 Patients not educated for lymphedema (n=57) p 53,26± 9,595 29,61 ± 4,50 0.778 0.980 2 3 6 5 5.1±3.9 1 20 18 18 4.9±4.2 0,312 3 7 0,506 2 0 13 11 1 42 0,704 18,60± 30,69 18,87± 28,39 0.98 10 11 21 36 0,170 10 6 17 40 0,017 5 11 19 38 0,025 6 10 0 37 18 1 0,153 6 10 0 36 19 2 0,047 11 5 31,81±32,65 20 36 26,95±41,65 0.62 24 40.6±26.4 59.9±27.4 11 36.9±18.7 61.01±20.7 0.86 0.55 0,816 0,019