Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
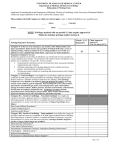
EXAMPLE Unacceptable Criteria-based Privilege Set SPECIALTY: ANESTHESIOLOGY NAME:______________________________________ Please print □ Initial □ Change in Privileges □ Renewal of Privileges To be eligible to request these clinical privileges, the applicant must meet the following threshold criteria: Basic Education: Minimum Training: Board Certification: Clinical References: Proctoring Requirements: Other: MD, DO Successful completion of a residency training program Board eligibility required Three peer references who can attest to current competence First 10 cases License in (state), DEA, malpractice insurance CORE PRIVILEGES - ANESTHESIOLOGY □ Preoperative, intraoperative and postoperative examination, consultation, management, monitoring, evaluation and treatment of patients who are to be rendered unconscious or insensitive to pain during a surgical, obstetrical, dental and/or medical invasive procedure, and treatments that fall within the usual and customary scope of practice of a fully trained general anesthetist. SPECIAL PROCEDURES □ Pain Management: Admission, consultation, diagnosis, treatment, and management of painful syndromes, including post traumatic musculoskeletal pain, myofascial pain syndrome, cancer pain, reflex sympathetic dystrophies by the use of nerve blocks; drug therapy. Required Additional Criteria: Evidence of current competence. ADDITIONAL PRIVILEGES: If you wish privileges not included above, please list here ___________________________________________________________________________________ ___________________________________________________________________________________ ______________________ Date ____________________________________________________________________ Applicant’s Signature □ privileges as requested □ privileges with modifications ______________________ □ do not recommend _______________________ Date _____________________________________________________________________ Department Chair Signature ___________________ Credentials Committee Date _______________________ Date Medical Executive Committee _______________________ Date Board of Trustees Buchanan & Associates Consulting Handouts – Performance-based Privileging Rev. 05/10 EXAMPLE Acceptable Criteria-based Privilege Set SPECIALTY: Anesthesiology NAME_________________________________________ Please print To be eligible to request clinical privileges, the applicant must meet the following threshold criteria: At Your County Hospital, General Anesthesia services are covered by a Professional Services Agreement. Physicians who are not party to the Agreement are not eligible to request General Privileges in Anesthesiology, regardless of education, training and/or experience. Basic Education: MD, DO Minimum Formal Training: □ Successful completion of an ACGME or AOA-accredited residency training program in Anesthesiology. □ Current ABA Board Certification (or ABA equivalent board certification); or □ attain Board Certification within five years of completion of training program. Maintenance of Board Certification required for reappointment eligibility. Failure to obtain board certification within the required timeframe, or failure to maintain board certification, will result in automatic relinquishment of privileges. Documentation of active practice in Anesthesiology and management of anesthesia care for a minimum of 300 cases in an accredited hospital or healthcare facility during the past 24 months. Recent residency or fellowship training experience may be applicable. If applicant cannot document appropriate experience, a specified proctorship/review plan may be considered at the discretion of the medical staff. Training director, or appropriate chair from another hospital where applicant has held active privileges within the past year; and two additional peer references who have recently worked with the applicant and directly observed his/her professional performance over a reasonable period of time and who will provide reliable information regarding current clinical competence, ethical character and ability to work with others. At least 2 references must be surgeons who have directly observed professional performance. Board Certification: Required Previous Experience: (required for new applicants) Clinical References: (required for new applicants) Continuing Medical Education Other: Sufficient to meet licensure and/or board certification Current, unrestricted license to practice medicine in _________ Malpractice insurance in the amount of ____, or as established by the Board of Trustees Current, unrestricted DEA certificate Eligible to participate in federally funded programs (Medicare/Medicaid) Applicants have the burden of producing information deemed adequate by the hospital for a proper evaluation of current competence and other qualifications and for resolving any doubts or questions raised by appropriate medical staff leaders, committees, or governing board. If you meet the threshold criteria above, you may apply for those privileges appropriate to your training and current competence: Buchanan & Associates Consulting Handouts – Performance-based Privileging Rev. 05/10 GENERAL PRIVILEGES – ANESTHESIOLOGY Preoperative and postoperative assessment, consultation, management, monitoring, evaluation and treatment of patients of all ages (unless specifically excluded from practice) who are to be rendered unconscious or insensitive to pain during a surgical, obstetrical, dental and/or medical invasive procedure, and treatments that fall within the usual and customary scope of practice of a fully trained general anesthetist. Such privileges include but are not limited to: Preoperative evaluation Intravenous conscious/moderate sedation management of fluid, electrolyte and metabolic parameters Airway management, basic and complicated, including all associated devices and techniques Invasive monitoring local and regional anesthesia with and without sedation, including topical and infiltration, minor and major nerve blocks management of intraoperative complications management of PACU problems peripheral nerve block to include major plexus block anesthesia for laser surgery of the airway manipulation of body temperature manipulation of cardiovascular parameters cardio-pulmonary resuscitation including tracheal intubation, ventilation, and basic and advanced CPR monitoring; ■ East Buchanan West Buchanan □ Requested □ Requested -------------------- -------------------- □Approved □Approved □W/ Conditions □W/ Conditions □ Not Approved □ Not Approved □ Requested □ Requested -------------------- -------------------- □Approved □Approved □W/ Conditions □W/ Conditions □ Not Approved □ Not Approved Excludes: Privilege to admit. Cross out & INITIAL any privilege you are not applying for in this set of General Privileges Criteria for Renewal of Privilege: Evidence of management of 300 cases in past 24 months. SELECTED PRIVILEGES Must request General Privileges in specialty in order to apply for Selected Privileges Documentation of compliance with specified criteria listed below must be submitted at the time of request Pain Management: Consultation, diagnosis, treatment, and management of painful syndromes, including post traumatic musculoskeletal pain, myofascial pain syndrome, cancer pain, reflex sympathetic dystrophies by the use of nerve blocks; drug therapy, and/or multidisciplinary approaches. Procedures include: cervical, thoracic, lumbar and caudal blocks Differential spinal blocks Cervical, brachial and lumbar plexus blocks Stellate ganglion blocks Celiac plexus blocks Lumbar sympathetic blocks Regional blocks of the head, neck and limbs Blocks for the treatment of cephalgia Additional Criteria for Initial Appointment: □ Evidence of 12 month ACGME/AOA-approved residency / fellowship devoted to Pain Management; or □ ABMS board certification in Pain Management; or □ Evidence of having actively performed pain management procedures during the previous 24 months; and written evaluation from recent training director or department chair at another hospital where applicant held privilege during the previous 24 months. Buchanan & Associates Consulting Handouts – Performance-based Privileging Rev. 05/10 Proctoring/Review Requirements: Chart review of first 5 cases. Required Activity Level: □ Evidence of successful performance of at least 100 invasive pain management procedures during past 24 months (e.g.: nerve blocks, implantation of electrical stimulators, catheters and pumps). (Activity level required for initial granting and renewal of privilege.) **NOTE: This privilege also available in other specialty delineations and includes equivalent criteria for training/experience. Spinal Cord Stimulators / Neuraxial Infusion System Implementation □ Requested □ Requested Additional Criteria for Initial Appointment: □ Documented evidence from ACGME/AOA -approved residency/ subspecialty training program attesting to training and competence in spinal cord stimulator implantation & infusion pump implantation; or □ ABA board certification with added qualification in Pain Management; or □ Evidence of having actively performed procedures during the previous 24 months; and written evaluation from recent training director or department chair at another hospital where applicant held privilege during the previous 24 months. -------------------- -------------------- □Approved □Approved □W/ Conditions □W/ Conditions □ Not Approved □ Not Approved Proctoring/Review Requirements: Proctor present for first case. Required Activity Level: □ Documentation of successful performance of at least five procedures in past 12 months. ( Activity level required for initial and renewal.) ADDITIONAL PRIVILEGES: A request for any additional privileges not included on this form must be submitted to the Medial Staff Office and will be forwarded to the appropriate review committee to determine the need for development of specific criteria, personnel & equipment requirements. EMERGENCY: In the case of an emergency, any individual who has been granted clinical privileges is permitted to do everything possible within the scope of license, to save a patient’s life or to save a patient from serious harm, regardless of staff status or privileges granted. ACKNOWLEDGEMENT OF PRACTITIONER: I have requested only those privileges for which by education, training, and demonstrated performance I am qualified to perform, and have provided documentation to support my eligibility to request each group of procedures requested. I understand that in making this request I am bound by the applicable bylaws and/or policies of the hospital and medical staff. ________________________________________________________ Applicant’s Signature ________________ Date DEPARTMENT CHAIR REVIEW I have reviewed and evaluated this individual’s request for clinical privileges, the verified credentials, quality data and/or other supporting information. Based on the information available and/or personal knowledge, I recommend the practitioner be granted: □ privileges as requested □ privileges with conditions/modifications as noted ________________________________________________________ Department Chair Signature □ do not recommend _________________ Date Credentials Committee:_____________________ (date of Committee review/recommendation) □ privileges as requested □ privileges with conditions/modifications as noted □ do not recommend Medical Executive Committee:_______________________ (date of Committee review/recommendation) □ privileges as requested □ privileges with conditions/modifications as noted □ do not recommend Board of Trustees:____________________________(date of Board review/action) □ privileges as requested □ privileges with conditions/modifications as noted □ do not approve Conditions/Modifications: Buchanan & Associates Consulting Handouts – Performance-based Privileging Rev. 05/10 Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2-12-25 Baltimore, Maryland 21244-1850 Center for Medicaid and State Operations/Survey and Certification Group Ref: S&C-05-04 DATE: November 12, 2004 TO: State Survey Agency Directors FROM: Director Survey and Certification Group SUBJECT: Centers for Medicare & Medicaid Services (CMS) Requirements for Hospital Medical Staff Privileging Letter Summary The hospital’s Governing Body must ensure that all practitioners who provide a medical level of care and/or conduct surgical procedures in the hospital are individually evaluated by its Medical Staff and that those practitioners possess current qualifications and demonstrated competencies for the privileges granted. State Survey Agency (SA) surveyors are to determine whether the hospital’s privileging process and its implementation of that process comply with the hospital Conditions of Participation (CoPs). The purpose of this memorandum is to provide survey and certification clarification regarding the hospital privileging system requirements in the hospital CoPs at 42 CFR §482. Background The hospital’s Governing Body is legally responsible for the conduct of the hospital as an institution. The Medical Staff is accountable to the Governing Body for the quality of care provided to patients at the hospital. Both hospital bodies must ensure that all patient care is provided by or in accordance with the orders of a practitioner who meets the Medical Staff criteria for the privileges granted; who has been granted privileges by the Governing Body in accordance with established procedures for applying those criteria; and who is working within the scope of those granted privileges. Page 2 – State Survey Agency Directors The hospital must have a privileging process in place that complies with CMS requirements. The hospital’s privileging process must be in compliance with the hospital CoPs at §482.12 (Governing Body), §482.22 (Medical Staff), and with other CoPs that require medical staff oversight of practitioner qualifications and privileges, federal and state law, and the process must be approved by the hospital’s Governing Body. The hospital’s Medical Staff bylaws must describe the privileging process to be used in the hospital. The process must include criteria for determining the privileges that may be granted to individual practitioners and a procedure for applying the criteria to individual practitioners. Medical Staff Composition The Medical Staff must be composed of doctors of medicine (MD) or osteopathy (DO) and, in accordance with state law, may also be composed of other practitioners appointed by the Governing Body. These other practitioners may include, but are not limited to dentists, podiatrists, chiropractors, advanced practice registered nurses (nurse practitioners (NP) and nurse midwives), certified registered nurse anesthetists (CRNA), physician assistants (PA), psychologists, licensed clinical social workers, optometrists, etc. The Medical Staff, as a group, is responsible for the quality of care provided to patients by the hospital, for establishing the bylaws, rules, regulations, policies, etc. for the medical staff and for overseeing the quality of Buchanan & Associates Consulting Handouts – Performance-based Privileging Rev. 05/10 care provided by all the individual practitioners who provide a medical level of care or who conduct surgical procedures at the hospital. Categories of Practitioners The hospital’s Governing Body must determine which categories of practitioners (i.e. MD, DO, NP, PA, dentists, podiatrists, chiropractors, CRNA, midwives, etc. who, in accordance with state law, may be granted active, courtesy, emergency, temporary, etc. privileges in the hospital) are eligible for appointment to its Medical Staff, as well as, which categories of practitioners are not allowed membership on the Medical Staff but are eligible for privileges. Not all practitioners with privileges would necessarily be members of the hospital’s Medical Staff. The hospital’s Governing Body may grant non-members of the Medical Staff medical level privileges and/or privileges to conduct surgical procedures. For example, advanced practice registered nurses, PAs, RN first assistants, psychologists, CRNAs, licensed social workers, optometrists, and other practitioners, including physician residents and other physicians who hold only temporary or honorary privileges may or may not be allowed to become members of the Medical Staff. However, these practitioners are responsible for complying with the bylaws, rules, regulations, and policies in rendering care and services. The hospital’s Medical Staff bylaws must state the duties and scope of privileges each category of practitioner may be granted. Specific privileges for each category must clearly and completely list the specific privileges or limitations for that category of practitioner. The specific privileges must reflect activities that the majority of practitioners in that category can do and that the hospital can support. It cannot be assumed that a practitioner can perform every task/activity/privilege listed/specified for the applicable category of practitioner. The individual practitioner’s ability to perform each task/activity/privilege must be assessed and not assumed. Page 3 – State Survey Agency Directors If the practitioner is not competent to perform one or more tasks/activities/privileges, the list of privileges is modified for that practitioner. Hospitals must assure that practitioners are competent to perform all granted privileges. The Medical Staff must periodically (defined as no less frequently than every 24 months in the absence of a State law that requires more frequent appraisals) conduct appraisals of individual current practitioners for continued or revised hospital privileges and must conduct individual appraisals of practitioner applicants requesting privileges. The Medical Staff must actually examine each individual practitioner’s qualifications and demonstrated competencies to perform each task/activity/privilege he/she has requested from the applicable scope of privileges for their category of practitioner. Components of practitioner qualifications and demonstrated competencies would include at least: current work practice, special training, quality of specific work, patient outcomes, education, maintenance of continuing education, adherence to medical staff rules, certifications, appropriate licensure, and currency of compliance with licensure requirements. All practitioners providing a medical level of care and/or conduct surgical procedures either directly or under supervision, whether employed by the hospital, physician or other entity, or contracted, must be individually evaluated. Board certification, certification, or licensure in and of itself is not recognized as an appropriate basis to bestow or award any or all of the privileges included in a particular practitioner’s category. Any procedure/task/activity/privilege requested by and recommended for a practitioner beyond the specified list of privileges for their particular category of practitioner would require evidence of additional qualifications and competencies, and be an activity/ task/procedure that the hospital can support and is conducted within the hospital. Privileges cannot be granted for tasks/procedures/activities not conducted within the hospital despite the practitioner’s ability to perform the requested tasks/ procedures/ activities. The hospital’s Governing Body and Medical Staff must assure that every individual practitioner who provides a medical level of care and/or who conducts surgical procedures in the hospital is competent to perform all granted privileges. The purpose of the Medical Staff’s evaluation of each individual practitioner is to determine that a new applicant possesses the qualifications and competencies to have specific privileges granted or, in the case of current members of the medical staff, to evaluate the individual practitioner’s qualifications and demonstrated competencies in order to determine if that practitioner’s clinical privileges should be continued, discontinued, or revised. After the Medical Staff conducts its appraisal of individual practitioners, it makes recommendations to the Governing Body as to the extent of the privileges it is recommending be granted to each individual practitioner. Role of Governing Body in Granting Privileges After considering the Medical Staff’s recommendations to grant, deny, continue, revise, discontinue, limit, or revoke specified privileges, and in accordance with established hospital Medical Staff criteria and state and federal laws and Buchanan & Associates Consulting Handouts – Performance-based Privileging Rev. 05/10 regulations, the Governing Body determines whether to grant the recommended privileges for that practitioner. Only the hospital’s Governing Body can grant a practitioner privileges to provide care in the hospital. Page 4 – State Survey Agency Directors The hospital must ensure that the practitioner and appropriate hospital patient-care areas/departments are informed of the privileges granted to the practitioner, as well as, any revisions or revocations to the practitioner’s privileges. Furthermore, whenever a practitioner’s privileges are limited, revoked, or in any way constrained, the hospital must, in accordance with state and/or federal laws or regulations, report those constraints to appropriate state and federal authorities, registries, and/or databases, such as the National Practitioner Databank. CMS does not have a preference as to the “term” used to name the hospital’s privileging process. A hospital’s privileging process must comply with the CMS hospital CoPs. A privileging process that results in a practitioner being granted privileges based on other than the medical staff’s assessment of that individual practitioner’s qualifications and demonstrated competencies would not comply with CMS requirements. Effective Date: Immediately. The state agency should disseminate this information within 30 days of the date of this memorandum. Training: The information contained in this announcement should be shared with all survey and certification staff, their managers and the state/RO training coordinator. /s/ Thomas E. Hamilton cc: Survey and Certification Regional Office Management Buchanan & Associates Consulting Handouts – Performance-based Privileging Rev. 05/10 Chicago Hospital News January 2006 - Volume 3 - Issue 11 Hospitalists’ Committee Involvement Increases Value by Rene Toledo Over the last decade, the hospitalist movement has transformed from a newly coined concept with few practitioners into the fastest-growing medical specialty in the country with more 12,000 physicians in practice. During that time, their influence at the patient’s bedside and throughout the hospital has grown exponentially. I expect that in 2006 hospitalists will continue to increase their worth by actively participating in appointed medical staff committees or holding elected medical staff positions – including chief of staff – at every hospital in which they work. These involved physicians will continue to add significant value at hospitals throughout the greater Chicago area. Because hospitalists have no outpatient practice and instead focus 100 percent of their attention and medical skills on inpatient care, they offer unique insights into what needs improving and what the hospital and its medical staff can do to better serve their patients. More than any other physician, hospitalists have an obligation to their hospital and to their profession to be the catalyst for continuous quality improvement within their facility — from advocating systemic changes where needed to providing firsthand input into medical staff policies to engineering changes in standard hospital procedures. And they should be on the frontlines of the "hot" issues of the day, from patient safety to end-of-life care to how information technology can aid in the delivery of care. Hospitalists who accept this challenge will need to learn to broaden their thinking beyond the hands-on delivery of care one patient at a time and into a more global view of hospital operations. In this regard, I see hospitalists increasingly working hand in hand with their medical center’s leadership and focusing their combined energy and knowledge towards greater efficiencies, improved clinical outcomes and higher patient satisfaction. As hospitals around the country are finding out, coupling a committed administration with a dedicated hospitalist forms a winning combination. The hospital’s vice president of medical affairs and/or the chief of staff who is entrusted with making committee appointments can contribute greatly to this model by placing hospitalists on key committees. Identifying energetic, committed and passionate physicians wanting to serve has always been a challenge. In many facilities here in Chicago, hospitalists are accepting this responsibility with great enthusiasm. As an example, local IPC hospitalists serve on 30 committees at ten different hospitals. Their wide-range of inpatient care makes them an asset to every one of these committees and their influence affects everything from quality assurance to medical standards to ethics to discharge. There is no better time than now for this to happen. The cold reality is that in many markets we are seeing a decline in physician commitment at the local hospital level. The reasons for this are many – from an increased emphasis on cash-related medical businesses (such as cosmetic procedures and boutique practices) to the emergence of specialty hospitals (such as surgi-centers) to the simple fact that primary care physicians are able to do more and more in their office setting. This creates a wonderful window of opportunity for forward-thinking hospitals to identify a committed group of hospitalists who are there every day and who wish to take an active role in how the hospital operates. We have spent the last decade introducing the medical community as well as consumers at large to hospitalists. Beginning in 2006 we should now turn our attention to increasing hospitalists’ value to fellow physicians, hospital executives and patients alike by recognizing and embracing the broader role they can plan in the achievement of better, more patient-focused care. Rene Toledo is the executive director of IPC-The Hospitalist Company which currently serves 13 facilities in th Buchanan & Associates Consulting Handouts – Performance-based Privileging Rev. 05/10 PEER REFERENCE EXAMPLE Date Name Address City / State / Zip Dear Dr. ____________: RE:__________________________ (Physician) The above named physician has applied for appointment to the medical staff and/or clinical privileges at ___(hospital). The applicant has listed you as a peer reference. Your completion of this questionnaire will be greatly appreciated as we assess his/her qualifications and current competence. A Release from Liability statement and a return envelope are enclosed. We will protect the confidentiality of the information you provide to the full extent of the law. Sincerely, XXXXXX 1. Number of years I have know this physician:_________. We are: □ social friends; □ colleagues from medical school, internship or residency; □ professional associates; □ practice partners; □ other ___________________________________ 2. Have you had the opportunity to observe this physician’s practice, skills, competence within the past two years? □ Yes □ No. If yes, in what capacity :______________________________. 3. The applicant has applied for privileges in ___(specialty)___. Do you know of any procedures which should be excluded or limited for this practitioner in this specialty? □ Yes* □ No 4. For the following categories, please rate this physician: Very Good Medical/clinical knowledge _____ Professional judgment _____ Technical skills _____ Recordkeeping _____ Patient management _____ Interpersonal/communication skills _____ Professionalism _____ Sense of responsibility _____ Average ____ ____ ____ ____ ____ ____ ____ ____ Fair/Poor* ____ ____ ____ ____ ____ ____ ____ ____ Unable to Evaluate ____ ____ ____ ____ ____ ____ ____ ____ 5. Are you aware of any health problems (including disability, emotional stability, alcohol or drug problems) which might affect this physician’s ability to care for patients? □ Yes* □ No 6. To your knowledge, has practitioner attempted procedures beyond his/her skill or training? □ Yes* □ No 7. Do you have any basis upon which to doubt his/her personal integrity, honesty, ethics? □ Yes* □ No * If any questions have been answered indicating a “*”, please explain on separate sheet. If you wish to discuss this applicant’s qualifications with a member of our medical staff, please indicate the best time to contact you_________. _____________________________________________________________________________________________ Name (please print) Title Phone # ________________________________________________________ Signature NOTE: You may fax your response to (XXX) XXX-XXXX. Buchanan & Associates Consulting Handouts – Performance-based Privileging ___________________________ Date Rev. 05/10