Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
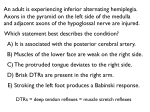
Rajiv Gandhi University of Health Science, Karnataka Curriculum Development Cell CONFIRMATION FOR REGISTRATION FOR SUBJECTS FOR DISSERTATION Registration No. : Name of the candidate : Ms. REMYA HARIDAS Address : #160, CHELIKERE,BANASWADI OUTER ROAD, BEHIND BTS BUS DEPOT, KALYAN NAGAR, BANGLORE 43 Name of the Institution : Banglore city college of Nursing Course of Study and Subject : MSc Nursing in MSN Date of submission : Title of study : “A STUDY TO EVALUATE THE EFFECTIVENESS OF STRUCTURED TEACHING PROGRAMME ON KNOWLEDGE REGARDING THE IMPORTANCE OF PUPILLARY CHANGES IN NEUROLOGICAL CLIENTS AMONG STAFF NURSES IN SELECTED HOSPITALS AT BANGALORE” Brief resume of intended work : Attached Signature of the Student : Guide Name : Mrs. VIJAYA LAKSHMI Remarks of the guide : Signature of the guide : Co-Guide Name : Mrs. VIJAYA LAKSHMI Signature of Co-Guide : HOD Name : Signature of the HOD : Principal name : Principal mobile No. : Principal E-mail ID : Principal signature : RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES. BANGALORE, KARNATAKA. “A STUDY TO EVALUATE THE EFFECTIVENESS OF STRUCTURED TEACHING PROGRAMME ON KNOWLEDGE REGARDING THE IMPORTANCE OF PUPILLARY CHANGES IN NEUROLOGICAL CLIENTS AMONG STAFF NURSES IN SELECTED HOSPITALS AT BANGALORE” SYNOPSIS PROFORMA FOR REGISTRATION OF SUBJECT FOR DISSERTATION Miss. REMYA HARIDAS BANGALORE CITY COLLEGE OF NURSING BANGALORE -43, KARNATAKA RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, BANGALORE, KARNATAKA. SYNOPSIS PROFORMA FOR REGISTRATION OF SUBJECT FOR DISSERTATION 1 NAME OF THE CANDIDATE AND ADDRESS Miss. Remyaharidas 1st year M.sc Nursing. Bangalore City College of Nursing Bangalore-560043 KARNATAKA 2 3 4 5 NAME OF THE INSTITUTION COURSES OF THE STUDY AND SUBJECT Bangalore City College of Nursing Banglore M.Sc(N) 1st year MEDICAL SURGICAL NURSING DATE OF ADMISSION TITLE OF THE SUBJECT A STUDY TO EVALUATE THE EFFECTIVENESS OF STRUCTURED TEACHING PROGRAMME ON KNOWLEDGE REGARDING THE IMPORTANCE OF PUPILLARY CHANGES IN NEUROLOGICAL CLIENTS AMONG STAFF NURSES IN SELECTED HOSPITALS AT BANGALORE 6. BRIEF RESUME OF INTENTED WORK INTRODUCTION: HEALTH CAN BE DEFINED AS A CONDITION OF BEING SOUND IN BODY, MIND OR SPIRIT ESPECIALLY FREEDOM FROM PHYSICAL DISEASE OR PAIN. To be in good health its important that each and every in our body should function properly. Eyes is an important organ which most of us take it for granted. It’s a highly specialized sense organ which unlike most organ of body, is available to external examination .One of its external structure include pupils. The pupil is the space that dilates and constricts in response to light. Normal pupils are round and constrict symmetrically when a bright light shines on them. About 20% of population have pupils that are slightly unequal in size that respond equally to light.[1] Different neuroanatomical pathways are involved in the control of pupil , the integrity and the functionality of these neurological pathways can be often be ascertained through the analysis and interpretation of pupillary behavior .This makes the pupil size and the pupillary light reflex an important factor to be considered in many clinical conditions. More specifically , the location of the pupillomotor nuclie and efferent occulomotor nerve is important for assessing the onset of descending transtentorial herniation and brainstem compression ,its has also been shown through blood flow imaging the pupillary changes in neurological patients in ICU are highly correlated with brainstem oxygenated and perfusion or ischemia[2] . High intracranial pressure in a brain injured patient result more frequently in poor neurological outcomes and death. High intracranial pressure are associated with pupillary abnormalities of brain injured patient. The signs of pupil problems can be noted by change in pupil size, which can occur as a result of medications drugs and toxins. Some neurological conditions such as stroke, brain tumor and injury to the brain can also cause change in pupil size on both eyes. The pupillary mechanism can also be characterized by different neuronal and mechanical nonlinearitis. Pupillary evaluation in the clinical settings in often performed in very subjective manner with a pen flash light for reactivity and a pupil gauge for pupil size. Pupil reaction to light should be brish and after removal of light source the pupil should return to its original size. There should also be a consensual reaction to the light source that is the opposite pupil also constricts when the light source is applied to one eye. In addition to controlling the amount of light that enters the eye, the pupillary light reflex provides a useful diagnostic tool. It allows for testing the integrity of the sensory and motor functions of the eye. Under normal conditions, the pupils of both eyes respond identically to a light stimulus, regardless of which eye is being stimulated. Light entering one eye produces a constriction of the pupil of that eye, the direct response, as well as a constriction of the pupil of the unstimulated eye; the consensual response Comparing these two responses in both eyes is helpful in locating a lesion. For example, a direct response in the right pupil without a consensual response in the left pupil suggests a problem with the motor connection to the left pupil (perhaps as a result of damage to the nerve or Edinger-Westphal nucleus of the brainstem[3]). Lack of response to light stimulation of the right eye if both eyes respond normally to stimulation of the left eye indicates damage to the sensory input from the right eye (perhaps to the right retina or optic nerve. 6.1 NEED FOR STUDY: Medical caregivers examine pupil size because they can be directly correlated to health conditions. In this case, it isn’t only the size of the pupils that are noted but their reactivity and equality too. In normal circumstances, pupils should be neither large nor small, but average. If extra light is supplied, both pupils should constrict and if surroundings become darker, both pupils should dilate, equally. What happens in one eye should also happen in the other, giving a bilateral reaction. Since nurse is also one of the important personality in the medical field, the nurse practitioners should have a fair knowledge about pupillary changes among the neurological clients. The pupillary evaluation in the clinical settings is ofen performed in very subjective manner with a pen flash light for reactivity and a pupil gauge for pupil size , which can be used by the nurse practitioner also. Traumatic brain injuries (TBIs) affect more than 1.4 million Americans annually[4] Nurses caring for these patients routinely perform serial neurologic assessments, including pupillary examinations. While nurses are likely familiar with basic components of the pupillary examination, some confusion about more specific aspects of the examination and the physiologic basis of the pupillary response may still remain. Therefore, it is important to identify the key components of a pupillary examination and its associated physiologic response. So once they know how to perform this pupillary examination, it will be a great help to the patients. The pupillary changes can be mostly seen in the cases such as brain injury, stroke ,brain tumer, thired nerve palsy. Horner’s syndrome some of the medications such as atropine steroids contraceptives etc and early detection of these changes may save the life of the patients. Appropriate training and ongoing professional development in this field of study are essential for optimised clinical outcomes. Therefore the identification of pupillary changes among the critically ill patient may prevent further detoriation of their health condition. The pupillary light reflex is a reflex that controls the diameter of the pupil, in response to the intensity (luminance) of light that falls on the retina of the eye, thereby assisting in adaptation to various levels of darkness and light, in addition to retinal sensitivity.[5] Greater intensity light causes the pupil to become smaller (allowing less light in), whereas lower intensity light causes the pupil to become larger (allowing more light in). Thus, the pupillary light reflex regulates the intensity of light entering the eye. Twenty-two patients with acute optic neuritis were studied by the techniques of infrared pupillometry and visual evoked responses (VER) to pattern reversal. A relative afferent pupillary defect was found in all cases and the magnitude of this defect was found to be related to the amplitude, but not to the latency, of the VER. During follow-up the afferent defect was found to remain persistently abnormal while other methods of clinical evaluation could not demonstrate abnormality reliably. The amplitude of the VER also remained low.[6] Emergency room physicians routinely assess the pupillary reflex because it is useful for gauging brain stem function. Normally, pupils react (i.e. constrict) equally. Lack of the pupillary reflex or an abnormal pupillary reflex can be caused by optic nerve damage, oculomotor nerve damage, brain stem death and depressant drugs, such as barbiturates. Therefore involvement of nurses in assessment of pupillary reflexes among the neurological clients is considered as a vital , to detect the changes in brain stem function.. Early detection of brain death can also be done using the pupillary reflexes to external stimuli, as such organ transplantation can also be promoted by using this as a tool ,after confirming the brain death with additional scanning method such as CT Scan ,MRI etc .. The focus of this study is mainly to evaluate the knowledge among the staff nurses who come in direct contact with the neurological clients of importance of pupillary reflexes and also to improve their care by providing knowledge regarding management of pupillary changes in these patients… 6.2 REVIEW OF LITERATURE: Review of literature is the key step in the research process. It improves the systematic identification, location, and summary of the written material that contains information of research problem. The overall purpose of the review of literature is to develop a strong knowledge base to carry out research and other scholarly education. Pupillographic findings in 39 consecutive cases of harlequin syndrome was done In this, a consecutive series of 39 patients with harlequin syndrome who were referred to a tertiary autonomic function laboratory underwent slit-lamp examinations. Results were compared with a meta-analysis of all previously reported cases of harlequin syndrome. From this the following conclusions were made .The frequent coexistence of harlequin and Horner syndromes without other neurologic deficits suggest pathologic changes affecting the superior cervical ganglion. Because either syndrome may occur alone, damage is apparently selective. Among the patients with harlequin syndrome who also have tonic pupils and tendon areflexia (HolmesAdie syndrome), we postulate a ganglionopathy affecting not merely the (sympathetic) superior cervical ganglion, but also the (parasympathetic) ciliary and dorsal root ganglia. Because we found that more than 10% of patients had an undisclosed mass lesion in the chest or neck or a generalized autonomic neuropathy, we recommend a targeted evaluation in selected patients with harlequin syndrome.[7] A study related to Neurological features of congenital fibrosis of the extraocular muscles type 2 with mutations in PHOX2A was done .Congenital fibrosis of the extraocular muscles type 2 (CFEOM2) is a complex strabismus syndrome that results from mutations in the homeodomain transcription factor PHOX2A. To define the clinical and neuroimaging features of patients with this autosomal recessive syndrome, the study included 15 patients with genetically defined CFEOM2. All patients underwent full neurological, neuro-ophthalmological and orthoptic assessments.[8] Twelvepatients had pupillary pharmacological testing and nine had 3.0 tesla MRI of the brain, brainstem and orbits. They concluded the CFEOM2 phenotype and neuroimaging are both consistent with the congenital absence of CNs 3 and 4. Additional features included presence of most central ocular motility reflexes, a central lack of pupillary responsiveness of uncertain aetiology and modest phenotypic variability that does not correlate with specific PHOX2A mutations. Clinical presentation, neuroimaging and Phox2a-/- animal models all support the concept that CFEOM2 is a primary neurogenic abnormality with secondary myopathic changes.[9] Prehospital status and treatment among severe traumatic brain injury was conducted. In this collected data sets from 396 patients with severe TBI (Glasgow Coma Scale score < 9) included by 5 Austrian hospitals were available. The analysis focused on incidence and/or degree of severity of typical clinical signs, frequency of use of different management options, and association with outcomes for both. The following outcome was find out ,the majority of patients were male (72%), mean age was 49 +/- 21 years, mean injury severity score (ISS) was 27 +/- 17, mean first GCS score was 5.6 +/- 2.9, and expected hospital survival was 63 +/30%. ICU mortality was 32%, 90-day mortality was 37%, and final outcome was favorable in 35%, unfavorable in 53%, unknown in 12%. They found that age > 60 years, ISS > 50 points, GCS score < 4, bilateral changes in pupil size and reactivity, respiratory rate < 10/min, systolic blood pressure (SBP) < 90 mm Hg, and heart rate < 60/min were associated with significantly higher ICU and 90-day mortality rates, and lower rates of favorable outcome.[10] A study on False negative apraclonidine test in two patients with Horner syndrome in this two women aged 34 and 46 years with a cocaine-confirmed oculosympathetic defect (Horner syndrome) were tested with 1 % topical apraclonidine on separate days. Neither patient demonstrated a reversal of anisocoria, the current criterion for diagnosing a Horner syndrome using apraclonidine. Thus, these two patients with an established oculosympathetic defect were said to have a "negative test" for Horner syndrome. Yet both women showed subtle pupil and/or lid changes in response to apraclonidine that were consistent with sympathetic denervation supersensitivity. Reversal of anisocoria following topical apraclonidine does not occur in all patients with a unilateral oculosympathetic defect and more specific parameters for defining a positive test result might optimize apraclonidine's utility as a diagnostic test for Horner syndrome.[11] Evaluation of visual functions in patients on ethambutol therapy for tuberculosis was done to study the incidence of clinical and subclinical optic nerve toxicity with ethambutol therapy in patients with tuberculosis and to evaluate the reversibility of its side effects after cessation of therapy. This prospective randomized controlled study included 60 newly diagnosed adult cases of tuberculosis, who were randomly assigned into two groups. The study group included 30 patients (60 eyes) who received ethambutol as a part of their anti-tubercular treatment and the control group included 30 patients (60eyes) who did not receive ethambutol. The patients were examined on monthly basis. The visual parameters studied were best corrected visual acuity, pupillary reactions, optic disc changes, color vision, contrast sensitivity, pupilcycle time, visual field charting and visual evoked potential. Ethambutol was stopped in those patients in whom toxicity was detected and they were followed more frequently ethambutol induced ocular toxicity was seen in three patients (10%) in this study. The maximum visual recovery occurred in first six to eight weeks after stopping ethambutol. The visual recovery was complete in only one patient, but it was partial in two patients i.e. visual fields, contrast sensitivity and visual evoked potential remained abnormal.[12] Pupil response components among patients with Parinaud's syndrome was included In addition to light flux changes, it is well established that other stimulus attributes such as colour, spatial structure or movement can also cause a transient constriction of the pupil, even when the onset of the stimulus causes a net decrease in light flux level on the retina. Although experimental findings in human subjects with postgeniculate lesions show that the generation of such responses must involve the processing of stimulus attributes in extrastriate areas of the cortex, little is known about the site of integration of cortical signals into the pupillomotor pathway. We have investigated how visual performance and the various components of the pupil response have been affected in subjects with damage to the dorsal midbrain (Parinaud's syndrome). The results show that the probable destruction of the olivarypretectal nucleus and the nucleus of the optic tract has little or no effect on pupil grating or pupil colour responses.[13] The objective evaluation of improvement in optic neuropathy following radiation therapy for thyroid eye disease was to quantify the changes in parameters of optic neuropathy after orbital irradiation for thyroid eye disease twelve consecutive patients with optic neuropathy from thyroid eye disease were followed by a single neuro-ophthalmology practice and treated by one radiation oncologist with radiation therapy from 1991 through 1995. All cases were prospectively followed for visual acuity, color vision, mean deviation, and/or foveal sensitivity and afferent pupillary defect. All patients received 2000 cGy in 10 fractions with megavoltage irradiation to the orbits as a result this study objectively demonstrates improvement in optic neuropathy from radiation therapy for thyroid eye disease.[14] Pupillographic sleepiness testing in hypersomniacs and normals in this Seven patients (four with sleep apnea syndrome, three with narcolepsy) and seven agematched controls underwent pupillography for 11 min in complete darkness. The changes in pupil size were analyzed mathematically to determine quantitatively the amount of pupillary instability this study showed that a pupillographic sleepiness test based on the evaluation of spontaneous pupillary changes in darkness is applicable in hypersomniacs and may facilitate therapy control, i.e. diagnostic grading by measuring daytime sleepiness objectively.[15] Optic neuropathies and peripheral oculomotor disorders in patients with AIDS In patients with the acquired immunodeficiency syndrome (AIDS) there is an 8% incidence of neuro-ophthalmological changes. ophthalmological changes are: 1) The Cranial commonest nerve pareses 2) of Optic these neuroneuropathy and 3) Pupil disorders. The cranial nerve pareses are usually combined, rather than single, and are due to intraparenchymatous lesions (toxoplasmosis or lymphoma) or to meningitis (tuberculous or lymphoma). The optic nerve changes tend to be papillitis due to CMV or optic neuropathy due to syphilis or to cryptococcal meningitis. Among the pupil changes, Bernard-Horner syndromes due to sympathetic involvement, Argyll-Robertson pupils due to mesencephalictectal lesions and mydriasis associated with the common oculo-motor nerve have been described.[16] Clinical pearls in optometric management of the geriatric patient clinical management techniques (pearls) are discussed which aid in the diagnosis and treatment of problems specific to geriatricpatients. Factors noted in patient presentation are stressed and include physical appearance, ability to move about, and use of other senses. The most commonly occurring eye anomalies occurring in the geriatric population are discussed including iatrogenic drug side effects, pupillaryanomalies, extraocular palsies, dry eye, corneal degenerations, refractive error changes, lenticular changes, glaucoma, age-related maculopathy, vitreoretinal disease, and ocular manifestations of systemic disease (vascular occlusive disease, diabetes, ischemic optic neuropathy, other neuro-ophthalmic disease) optometrists as primary health care providers often provide the only avenue individuals with blinding and sometimes life threatening conditions have in managing these conditions. Optometrists managing geriatric patients are required to know what happens to this population from an ocular disease as well as other function and dysfunction standpoint.[17] Prognosis in solitary intraventricularhaemorrhage.Clinical and computed tomographic observations.Isolated intraventricularhaemorrhage (IVH) in the absence of parenchymal haematoma is unusual. Fifteen patients with solitary IVH among 170 with intracranial haemorrhage were studied. Clinical details and computed tomographic features were analysed to evaluate the prognostic significance of various clinical and CT parameters. Outcome is affected by hypertension, level of consciousness, clinical progression, pupillary changes and restriction of eye movements. Factors found on CT to have prognostic significance included degree of ventricular bleed, presence of cisternal bleed, hydrocephalus and cerebral atrophy.[18] STATEMENT OF THE PROBLEM “A study to evaluate the effectiveness of structured teaching programme on knowledge regarding the importance of pupillary changes in neurological clients among staff nurses in selected hospitals at Bangalore.” 6.3 OBJECTIVES OF THE STUDY: 1. To assess the knowledge level of staff nurses regarding importance of pupillary changes. 2. To evaluate the effectiveness of structured teaching programme on the importance of pupillary changes in neurological clients among staff nurses. 3. To find out the association between pre and post test knowledge scores regarding importance of pupillary changes among staff nurses 4. To find out the association of post test level of knowledge with selected demographical variables. 6.4 OPERATIONAL DEFINITIONS: KNOWLEDGE It refers to the correct response from the participants regarding the importance of pupillary response and is assessed by knowledge questionnaire. EFFECTIVENESS It refers to the significant of gaining knowledge as measured by the instrument and shown by post test knowledge school. STAFF NURSES Staff nurses who are working in neurological icu and wards IMPORTANCE OF PUPILLARY REFLEXES It refers to the intervention taken to the prior to the onset of pupillary changes for promoting patient care. 6.5 ASSUMPTIONS 1. Staff nurses have less knowledge regarding importance of pupillary changes 2. Education enhances the staff nurses to identify pupillary changes by themselves. 3. Group teaching will provide opportunity for active learning among participant 6.6 HYPOTHESIS H1:- There will be significant association between pretest and post test knowledge and selected demographical variables of staff nurses such as age sex education experience, skill marital status and source of information. H2:- The main post test knowledge scores of staff nurses regarding the importance of pupillary changes will be significantly higher than that of pretest knowledge score. 6.7 VARIABLES UNDER STUDY 6.7.1 DEPENDENT VARIABLES:Knowledge level of staff nurses regarding pupillary changes in neurological clients. 6.7.2 INDEPENDENT VARIABLES:Structured Teaching programme 6.8 MATERIALS AND METHODS :6.8.1 SOURCE OF DATA: Staff nurses working in selected hospital 6.8.2 METHODS OF DATA COLLECTION: Prepared questionnaire 6.9 RESEARCH DESIGN:PRE-TEST,POST TEST DESIGN 7. SETTING OF THE STUDY:The study will be conducted among the staff nurse in selected hospitals at banglore 7.1POPULATION:The study includes staff nurse in selected hospitals at banglore. 7.2 SAMPLE SIZE:60 staff nurses. 7.2.1 SAMPLING TECHNIQUE Simple random sample technique 7.3 SAMPLING CRITERIA 1. INCLUSION CRITERIA 1. The staff nurses who works in selected hospital at banglore 2. The staff nurses who are willing to participate in the study 3. The staff nurses who knows English and kannada 2. EXCLUSION CRITERIA 1. The staff nurses who does not works in selected hospitals at banglore 2. The staff nurses who are not willing to participate in the study 3. The staff nurses who does knows English and kannada 7.4 TOOLS OF DATA COLLECTION Prepared questionnaires that consists of three parts Part1: Consists of objective questions related to demographic data Part2: Consists of questions regarding pupillary changes in nuerological clients. 7.5 METHODS OF DATA COLLECTION: The prepared questionnaire will be distributed to the subjects or interviewed by the questionnaire . Prior to the study the purpose of the study will be explained and consent of the participants will be obtained to involve in the study. Before the original , a pilot study will be conducted and necessary modifications and further refinements of the tools will be done. Researcher herself will collect the data. 7.6 DATA ANALYSIS AND INTERPRETATION Descriptive and inferential statistical techniques such as frequency distribution , central measures ( mean, median, mode) standard deviation. Chi square and corelation co-efficient will be used for data analysis and presented in the form of tables , graphs and diagrams 7.7 DOES THE STUDY REQUIRE ANY INVESTIGATION OR INTERVENTION TOBE CONDUCTED ON CLIENT/SAMPLE POPULATION /HUMANS OR ANIMALS? The study will be conducted among the staff nurses in selected hospitals at Bangalore. 7.8 HAS ETHICAL CLEARANCE BEEN OBTAINED FROM INSTITUTES? Prior permission will be obtained from the concerned authorithies of selected hospitals at Bangalore to conduct a study and also from research committee of Bangalore City College of Nursing, Bangalore. The purpose of the study will be explained to the management authority of selected hospitals at Bangalore.Scientific objectivity of the study will be maintained with honesty and impartiality. 8. LIST OF REFERENCES:1.Suzanne C. Smeltzer, Brenda G. Bare , Jaince L. Hinkle , Kerry H. Cheever, “Text book of medical surgical nursing ,12th edition , Lippincott, Williams and Wilkins Page no. 1835-1840. 2. A .K . Khurana , “ Book of ophthalmology”, 4th edition , Oxford Blackwell Publications, page no 167 3.Glen view IL , “Fundamental nuero science for basic and clinical application ,3rd edition, Churchilll Livingston, Elsevier, Page no. 245-247. 4.Porth, C.M. And atfin, “ Pathology : Concepts of altered health states, Philadelphia Lippincott William and Wikins,Page no. 1456-1467. 5.Hickey,J.”The clinical practice of neurological and neurosurgical nursing, 6th edition,Philadelphia , Churchill , Page no.134-145 6.Barker,R.A. and Barasi,S,”Neuroscience at a glance, 3rd edition, Oxford Backwell publishing, Page no.1456,1476. 7. J Neuroophthalmol. ,“Pupillographic findings in 39 consecutive cases of harlequin syndrome”,2008 Sep;28(3): 171-7. 8. Brain. “Neurological features of congenital fibrosis of the extraocular muscles type 2 with mutations in PHOX2A”. 2006 Sep;129(Pt 9):2363-74. 9. Lenartova L, Janciak I, Wilbacher I, Rusnak M, Mauritz W; Austrian Severe TBI Study Investigators,“Severe traumatic brain injury in Austria III: prehospital status and treatment” 10.Bosley TM, Oystreck DT, Robertson RL, al Awad A, Abu-Amero K, Engle EC Bremner F, Smith S,“Neurological features of congenital fibrosis of the extraocular muscles type 2 with mutations in PHOX2A” 11. Kawasaki A, Borruat FX,“False negative apraclonidine test in two patients with Horner syndrome” 12. Goyal JL, De Sarmi, Singh NP, Bhatia A,“Evaluation of visual functions in patients on ethambutol therapy for tuberculosis: a prospective study” 13. Wilhelm BJ, Wilhelm H, Moro S, Barbur JL,“Pupil response components: studies in patients with Parinaud's syndrome” 14. Rush S, Winterkorn JM, Zak R,“Objective evaluation of improvement in optic neuropathy following radiation therapy for thyroid eye disease” 15. Wilhelm H, Lüdtke H, Wilhelm B,“Pupillographic sleepiness testing in hypersomniacs and normals” 16. Torras-Sanvicens J, Arruga-Ginebreda J,“Optic neuropathies and peripheral oculomotor disorders in patients with AIDS” 17. Selvin GJ, Townsend JC,“Clinical pearls in optometric management of the geriatric patient” 18. Jayakumar PN, Taly AB, Bhavani UR, Arya BY, Nagaraja D,“Prognosis in solitary intraventricularhaemorrhage.Clinical and computed tomographic observations”