Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
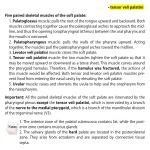
TEMPOROMANDIBULAR DISORDERS: AURAL SYMPTOMS AND CRANIOFACIAL PAIN Ramirez LM, DDS., MSD., Sandoval GP, MD., MSD., Schames J, D.M.D., James P Boyd, DDS. Sarra Cushen, BS In this review twelve different theories will be presented which have been proposed by different researchers since 1920 until the present. These theories offer a possible anatomic and embryologic link between the TMJ, the ear and adjacent structures based on a neurological, vascular and muscular approach connecting temporomandibular dysfunction (TMD) with aural and craniofacial referred symptomatology. INTRODUCTION This paper will explore the ways in which temporomandibular dysfunction (TMD) and otologic and craniofacial symptoms are related. In over 50% of patients with otic pain pathology of the ear is not present.1,2 Otic symptoms such as tinnitus, vertigo, hearing impairment, otic fullness, retroauricular and/or preauricular pain, and popping sensations3 are associated with functional and inflammatory disorders of the Temporomandibular joint (TMJ)4 and the masticatory muscles. Investigations have demonstrated that in TMD muscle hyperactivity can cause primary pain, referred pain, and reflex muscular contraction that can generate muscular dysfunction.5 TMD are a sub-classification of the muscle skeletal disorders and they include a wide range of craniofacial conditions with a multifactor etiology. They mask a great variety of subjective otologic signs and symptoms that are referred from the TMJ, the masticatory muscles, the cervical muscles and associated structures as much in adults as in children.6,7,8,9,10 The prevalence of TMD is two times higher in women than in men. 11,12,13 Bruxism plays a meaningful role in TMD and in craniofacial referred symptoms. The closest relation among a dysfunctional masticatory activity like bruxism, TMD and stress is a cause-effect relationship with the craniofacial disorders. Okeson4 considers bruxism a microtrauma resulting from a subconscious, non-functional clenching and grinding of teeth that can exceed the structural and physiological tolerance of muscles, teeth and articulations. Kato et al.14 establish that bruxism is a spontaneous and rhythmically intense motor manifestation secondary to a sequence of physiological changes observed as the increase of heart beating, motor activity, cortex and respiratory activity preceding the dental wearing. The sustained microtruma and dysfunction that is produced by bruxism is a precipitation as well as perpetuating factor of TMD. Green and Laskin15,16 have demonstrated that psychological stress is the main cause in the origin of TMD . TMD manifests as signs and symptoms in the head, neck and ear.17 These (symptoms) are also associated with shoulder and back pain18,19 that can generate referred craniofacial symptoms by involving the anterior, lateral and suboccipital cervical muscles in maximum occlusion. 20,21,22,23,24 Edmeads25 sets that the referred pain to the head from the cervical zone is generated through the facial and aponeurosis connections sharing functional continuity among shoulders, neck and pericranial muscles, so that the spasm or tension of neck muscles activate the neighboring pericranial muscles as well as the referred pain. Mense26 state that muscle pain and tenderness is not only perceived at the site of lesion but is usually referred to other areas. TMD can occur as aural, myalgic, articular, facial pain, and craniosinusal pain as well as create cephalalgic symptoms. Monson and Wright, in 1920, related the position of the jaw and the TMJ with impairment of hearing in adult and children populations. Goodfriend, in 1933, related the aural symptoms with the TMJ.27 Costen28 in 1934 associated the auricular and craniosinusal symptoms with articular disorders called Costen’s Syndrome. Costen was the first one to describe otic symptoms in total or partial edentulous patients and the reflex muscular contraction29 of muscles innervated by the trigeminal nerve (V3). Heteroptopic projected pain is generated as a result of irritation and compression of the sensorial branches of the auriculotemporal nerve. The functional and inflammatory disorders30 of the TMJ4 in their acute states are recognized by patients as “ear pain” 31, which can be explained by the proximity of both of these structures to the neighboring structures and the shared innervation by V3.27,32 Okeson4 states that 70% of the TMJ artralgias are declared by patients as otalgic pain. Most people are not aware of the possible relationship existing between symptoms, such as headache and otalgia to TMD and the masticatory system. EMBRYOLOGY Focusing on the articulation and the masticatory muscles, as origin of TMD, and their aural effects, it is undeniable that the embryological, physiologic and anatomical proximity of the TMJ and the ear affect each other. In the human being the development of the TMJ and structures such as the pharynges, the Eustachian tube, and the tympanic cavity is complex and still a controversial subject. Meckel’s cartilage, which is the first branchial arch, forms the jaw and the maxillar; the first and second arch forms the ossicle chain. The malleus has a double origin: the anterior process originates from mesenchimal cells (os goniale) through intramembranous ossification, and the rest form Meckel’s cartilage, through endochondral ossification.33 The middle auricular bones relate the malleus, also called the hammer, to the condylar blastema and the temporal blastema by fibrous connections passing through the petrotympanic fissure that Rees34 named the discomalleolar ligament in 1954. These fibrous connections of the external pterygoid muscle in the Meckel’s Cartilage form the interarticular disc by mechanical stimulation of this muscle but Youdelis35 confirms the opposite. The connection existing between the aural symptoms and the muscular and articular dysfunction in the head and neck has been studied.1,2,44 It is not clear yet if TMD contributes to tinnitus development or if they are the same phenomenon.45 Lockwood and Col.46 find some people alternate intensity of tinnitus with voluntary muscular orofacial movement. Vergara47 also found a solid relationship between facial and masticatory muscular movements and the variations in the quality of tinnitus. Morgan48 finds that when the muscles of patients with aural symptoms are palpated 75% present trigger points, which affirms that TMD can be one of the primary causes of tinnitus. The neurological, vascular and ligament connection between the TMJ and the middle ear persists in the course of articulation development because of the continuity in the Meckel’s Cartilage through the petrotympanic fissure that in adults shows an incomplete closing. The internal pterygoid muscle and the tensor tympani develop from the temporal blastema. These structures along with the tensor veli palatini are innervated by V3 through the otic ganglion, which innervates the masticatory muscles coming from the mesoderm of the first branchial arch in the same way.36 In this article we will develop the evident embryological connection regarding the innervation, the irrigation and the formation of auricular, pharinge and articular structures including the Eustachian tube.17,37,38,39,40,41,42 Rubinstein49 states that tinnitus is not a disease by itself but it is a symptom in the otologic spectrum. Rubinstein supports this idea by showing that patients with chronic tinnitus respond less to treatment than those with acute tinnitus. Vernon et al.50 assert that in tinnitus the greater the quantity of different sounds then the more complex this and TMD will be. Chole et al. in 1992 widely demonstrated (Chart 1) that tinnitus and vertigo are highly associated with TMD.51 Lam et al.52 affirm that the prevalence of referred otic pain and other aural symptoms of non otologic origin in patients with TMD varies from 3.5% to 42%1,36 and that the prevalence of tinnitus in patients with TMD seems to be higher than that found in the general population.23 The frequency of tinnitus in patients with TMD varies from 33% to 76%.1,27,31,53 The prevalence Researchers Nº Patients % Otalgia % Tinnitus % Vertigo % Hearing Loss 91 400 1391 64 742 86 25 47 45 200 476 148 996 57 797 338 411 470 3 38 21 100 36 93 100 47 82 --50 --63 40 1.6 100 12-16 32 14 13 32 43 40 42 44 20 76 36 36 14 63 17 6.4 59 12-17 26 5 12 28 5 20 14 --26 33 40 40 15 41 8.7 1.6 70 --18 26 13 32 38 15 33 --24 80 35 38 14 25 26 7.6 ----12 TMD Goodfriend 1933 Costen 1934 Myrhaug 1964 Dolowitz et al. 1964 Gelb et al. 1967 Bernstein et al. 1968 Principato-Barwell 1978 Koskinen et al. 1980 Brookes et al. 1980 Gelb-Bernstein 1983 Cooper et al. 1986 Wedel-Carlsson 1986 Cooper et al.23 1993 Ogutcen Toller et al.90 1993 Ciancaglini et al.80 1994 Parker y Chole27 1995 Kuttila et al.1 1999 Lam et al.52 2001 % Fullness Ear --6 --48 --62 --26 62 48 ----30 5 ----5-9 --- Chart 1. Chart modified from: Chole RA. MD, PhD, Parker WS. DMD,PhD. Tinnitus and vertigo in patients with temporomandibular disorders. Arch Otolaryngol Head Neck Surg. 1992;118(8):817-21. DIAGNOSIS Patients with otologic symptoms present painful muscles to the palpation more frequently than those without otologic symptoms.1,2 The cause of otic pain in individuals with TMD, but without a pathological condition in hearing or the nasopharinx is explained by the heterotopic referred pain of the masticatory muscles, the TMJ and associated structures. 2,3,23,43 of dizziness in patients with TMD ranges from 40% to 70%51,52 and that of vertigo from 5% to 40%.28,45,54 Hazell55 reported that 39% of the patients with tinnitus presented frequent tensional headaches with fatigue and muscular soreness in facial and masticatory muscles. 31 Bjorne and Col.56,57 assert that hearing damage and auditive loss frequently associated with tinnitus are strongly related to emotional tension symptoms such as cephalalgia, cervical and pericranial muscular tension, as well as dreaming disorders. Otorynolaryngological and odontological exams are vital to set differential diagnosis of the craniofacial symptoms by TMD.21,23,58 These should incorporate both intraoral and extraoral muscle explorations of the head neck59 as well as articular palpation of the muscles. Also a physical and visual examination of associated structures such as the pterygoid hamulus of the soft palate, the estilohioid complex, the temporalis tendon, the sphenopalatinum ganglion, the estilomandibular ligament and the parotid gland, and dental structures should be included as well as looking for possible cervical lesions. These exams are necessary to make a certain diagnostic approachment because of the similarity to craniofacial symptoms. The pain present in TMD is a subjective symptom which possesses a relevant diagnostic difficulty, especially under the absence of objective and unique signs which is why the differential diagnosis with associated structures is vital.4,25,60,61,62,63,64,65,6667,68,69,70,71,72,73,74,75,76,77 AURAL SYMPTOMS: THEORIES AND REALITY: Theory of the Referred Muscular Spasm: Myrhaug79 in 1964 suggested that neuromuscular dysfunctions of the masticatory muscles may trigger alterations in the sound-conducting apparatus. TMD produce tension and contraction in the masticatory muscles and a secondary reflex contraction in the tensor veli palatini and tensor tympani muscles generating aural symptoms. Bernstein et al.18 reported that there could exist a neurological association between the masticatory muscles, the suprahyoids, the middle ear muscles and the Eustachian tube muscles, based on the idea that V3 innervates the masticatory muscles, the tensor tympani and tensor veli palatini muscles.20,21,29,36,37,78,79,80,81,82,83 Myrhaug79 asseverates that in subjective tinnitus there is a contraction reflex of the tensor tympani muscle and that in objective tinnitus, where there is a rhythmical opening and closing of the pharyngeal area of the Eustachian Tube (palatal myoclonus), the contraction reflex is present in tensor tympani and tensor veli palatini muscles.84 Zipfel et al.85 affirms that the most common mechanical causes of objective tinnitus are palatal myoclonus and middle ear myoclonus (rhythmic movement of the tympanic membrane secondary to repetitive contraction of the tensor tympani and stapedial muscles). They also states that objective tinnitus is much less common that subjective tinnitus. Shapiro and Truex29 suggest a possible spasm by reflex contraction of the tensor tympani and the stapedial muscle to peripherally irritate the V and VII pair (facial) respectively. This can originate in the loss of the ability to hear low tones. It is worth mentioning that the reflex contraction of the stapedial and tensor tympani muscle is produced during high sounds and immediately before speaking. 17,86 Kamerer87 declares that the stapedial muscle improves external vocalization too, reducing the masking effect of autogenous sound. He also declares that the tensor tympani responds to external stimuli activated by vocalization, chewing, swallowing and the movement of the facial muscles.88 Travell and Simons89 explain that unilateral tinnitus, in the presence of trigger points in the ipsilateral maseteric and external pterigoid muscles describe a referred sensitivity phenomenon or a reflex muscular spasm of the middle ear muscles. Ogutcen-Toller and Juniper90 noticed that the structures that lead to sound in the middle ear could be affected by the reflexive contraction of the tensor tympani muscle produced by TMD.18 Although they referred to a spasm reflex as a cause of aural symptoms, they performed an audiological evaluation in patients with TMD and aural symptoms but did not find a dysfunction of the middle ear or the Eustachian tube, suggesting a more subjective hearing loss. Schames et al.36 and Myrhaug79 affirm that the dysfunction of the tensor tympani and tensor veli palatini muscles plays an important role in the relationship of TMD and otic symptoms. They name these muscles accessory masticatory muscles.21,31 Vergara47 describes the filogenetic and neurological relationship of the middle ear muscles. He explains that the tensor tympani muscle is a muscle of mastication and that the stapedial muscle is a facial muscle. These muscles are respectively innervated by V3 and VII. The normal function of Eustachian tube equalizes the pressure of the middle ear. The Eustachian tube also communicates with the nasopharinge by contracting the tensor veli palatini muscle which is assisted by the levator palatini muscle during velopharingeal movements such as swallowing and the inhaling phase of respiration.37,91,92,93,94 The alteration of its function can generate tinnitus, vertigo, sensation of hearing loss to low tones, otic fullness and otitis media with effusion, specially in children, secondary to the reflex contraction of the tensor tympani and the tensor veli palatini muscles.95 Marasa and Ham96 as well as Youniss8 assert that the Eustachian Tube dysfunction plays and important role in otitis media with effusion. Children are more susceptible to chronic otitis media with effusion especially during respiratory system infections because they have a short, horizontal and wide lumen of their Eustachian Tubes.97 These complex neuromuscular interactions between the masticatory muscles and the ear were named “Otognatic Syndrome” by Myrhaug79 in 1964 and then "otomandibular syndrome" by Bernstein in 196918 and Arlen in 1977.98 The patients with otomandibular syndrome present one or more aural symptoms, without having pathology in the ear, nose or throat, but with one or more muscles of the mastication in a state of constant spasm.18 Bjorne and Col.56,57 find a strong affinity among Meniere’s Syndrome and TMD, showing how the craniofacial muscular pain and the cervical spine disorders presented in TMD can produce fluctuant impairment of hearing, vertigo and tinnitus, supporting Goodfriend,27 Ciancagliani80 and Rubinstein53 findings. These findings show a strong correlation among deafness and the TMD associated with vertigo and tinnitus. Theory of the tensor veli palatini muscle origin Rood and Doyle99 as a result of adult and fetal cadaveric dissections found that the tensor veli palatini was composed of a medial portion, which Gray named the “tubae dilator” in 1918.100 They also found and external portion of the same muscle composed by the tensor veli palatini and an intratympanic zone composed by the tensor tympani muscle that intermingling its fibers with the external zone of the tensor veli palatini muscle.94,101,102 The lateral zone of the tensor veli palatini originates in the sphenoid spine, scaphoid fossa, tensor tympani muscle and the entire lateral osseous ridge of the sphenoid sulcus. The medial zone of the tensor veli palatini originates in the posterior and middle one-third of Eustachian Tube’s lateral membranous wall. These muscles converge and descend the hamular process in a strong tendon that curves around this zone to insert horizontally in the soft palate like an aponeurosis. Rood and Doyle affirm that movement patterns such as yawning, laughing, swallowing and coughing involve pharyngeal and laryngeal muscles that activate the tensor tympani muscle. Kamerer,87 in 1978, expresses his astonishment that there is not a unified theory dealing with this phenomena, even though there is a close anatomical relationship between the tensor tympani and the tensor veli palatini and electromiographically shows that they work simultaneously during swallowing assisting in Eustachian tube ventilation, like an air pump. Djupesland explained how the tensor tympani, during its reciprocal contraction with the tensor veli palatini, generates an inner deflection of the tympanic membrane that breaks the seal among the mucosal membranes of the Eustachian Tube isthmus. This expels air and contributes to the venting of the middle ear.88,97,103 Barsoumian, Kuehn and Col.104 corroborate Lupin’s 1969 findings and posteriously Rood and Doyle’s findings by observing in adult cadavers how the fibers of the most external zone of the tensor veli palatini muscle and the fibers of the tensor tympani are joined in the middle ear because of a small tendionous portion, showing an anatomical connection in the function of these muscles. Tensor tympani and tensor veli palatini muscles act synergistically together and temporary increase intra-tympanic pressure.88 These findings affirm that the tensor veli palatini has an additional bone origin in the manubrium of the malleus. The dysfunction of the tensor veli palatini muscle in TMD can either individually or in combination modify the medial position of the malleus and the tympanic membrane because of the insertion of the tensor tympani muscle. Even the spatial disposition of the oscicular chain can be modified by tension of the tensor tympani muscle because of its continuity with the tensor veli palatini muscle. In addition Schames and Col.36 attribute the secondary miofibrotic contraction to adhesions and trigger points of the tensor tympani and tensor veli palatini muscles due to dysfunction generated by TMD. This complicates the anatomical and functional relationship between these and aural symptomatology which is a consequence of reduced muscle fiber length. In 2002, Kierner et al.105 found the functional connection amount the tensor veli palatini and the tensor tympani muscles.106 They found this connection through histological analysis of five human cadavers. They affirm the re-confirmation of this finding and that it represents an important step in understanding the “functional unit” that these two muscles create in man. Ligamental Biomechanical Theory: Myrhaug79 affirms that the oscicular chain and the middle ear muscles belong embryologically to the chewing system. Posteriorly they become and serve as the hearing sense. Dissections of human adults and fetuses carried out by Pinto,32,107 Komori108 and other researchers34,38,82,109,110,111,112,113,114,115 proved a specific anatomical link between the TMJ, the sphenomandibular ligament and the middle ear made by the discomalleolar and the anterior malleolar ligaments that connect to the malleus separately in the anterior process or processus gracilis to conform to the previously described anterior ligament of the malleus.100,116 The anterior malleolar ligament is a continuation of the sphenomandibular ligament noted by Burch117; these according to Komori et al.108 and Ogutcen-Toller118 inserted on the ventral surface of the hammer coming out to form a horizontal “V” with the discomalleolar ligament in the petrotympanic fissure (Figure 1). According to Pinto the discomalleolar ligament is found more external and is inserted in the medioposteriorsuperior border of the capsular ligament and the disk. According to Komori et al. it is inserted only to the medioposteriorsuperior zone of the retrodiscal area and to the articular capsule. The anterior malleolar ligament is more medial than the discomalleolar ligament and connects the sphenomandibular ligament along with the Chorda Tympani nerve (VII). The sphenomandibular ligament is inserted in the lingula or mandibular spix spine and originates in the malleus, part of the sphenoid spine and the most medial zone of the petrotympanic fissure.119 The malleolar anterior ligament is an embryological remainder of Meckel´s cartilage and the disk-malleolar ligament is a remainder of the external pterygoid muscle. Pinto and later, in more detail, Komori show how the petrotympanic fissure in the Iter Chorda Anterius is trespassed by the Chorda Tympani and these two ligaments together within the Huguier Channel, separated by a bone ridge of triangular base on its path leaving the middle ear. The stretching of these ligaments by functional and/or inflammatory disorders4,120 affects the middle ear structures in some patients. According to Eckerdal82 the range of movement of these ligaments depends on the fibrous connection in the walls of the petrotympanic fissure, corroborating Coleman findings in 1970.121 Costen´s Theories -Neural Compression, Muscular Spasm and Muscular Tone. Figure 1. Graphic of superior view of Ear and TMJ zone dissections: A. External ear, B. Anterior Process of malleus, C. Chorda Tympani nerve, D. Tympanic anterior wall, E. Discomalleolar Ligament, F. Sphenoid spine, G. Posterosuperomedial retrodiscal and capsular zone, H. Anterior Malleolar Ligament, I. Disc, J. Sphenomandibular Ligament, K. External pterygoid muscle This ligament link between the TMJ and the middle ear can be biomechanically subjected to a functional or inflammatory articular disorder since the luxation or displacement of the disk and the secondary edema by inflammation,122,123,124,125 would generate additional anterior tension on the discomalleolar ligament because of the disk’s disposition and the increase of intrarticular pressure.126 The malleolar anterior ligament might be stretched by elongation of the sphenomandibular ligament in extreme movements, explaining the increase of tinnitus in exaggerated intermaxilar positions.18,31 Libin127 in 1987 suggested that the sphenomandibular ligament and the retrodiscal bilaminar zone could be tensed in the petrotympanic fissure under the normal physiological movements of jaw opening or as a result of cranial trauma to the temporal bone structures. Movements named the “Cranial Mechanism” can have deep implications in the movement freedom of the discomalleolar ligament and malleolar anterior ligament during jaw opening. Bernstein27 in 1933 observed how in extreme jaw movements some patients could change the intensity and quality of tinnitus. Burch128 researched the accessory ligaments finding that the sphenomandibular ligament relaxed in maximum jaw opening and it tensed in a position of marked overbite. Loughner et al.110 advise that in surgeries to the TMJ where condyle distractions of more than 10 mm are performed, the ossicular chain could be injured by the extreme traction of these ligaments over the anterior process of the malleus. They also suggest that in presence of infectious otitis media, the TMJ can be involved in generating capsulitis, especially in newborns where the connection of the middle ear and the TMJ is noticeable through the petrotympanic fissure.111 Marasa and Ham96 explain that the inflammation produced by inflammatory or functional disorders of the TMJ can spread through the petrotympanic fissure to the middle ear and generate otitis media. Reflex Vascular Spasm's Theory: Merida-Velasco et al.129 affirmed Bleicker’s 193829 findings that in newborns small vessels of the anterior portion of the middle ear cross the petrotympanic fissure and reach the venous retrodiscal plexus that drains into the retromandibular vein which is a part of the articular vascular plexus. In adults the most medial branches of the posterior group of the tympanic anterior artery irrigate the tympanic cavity and the external auditory meatus. They demonstrate how these most medial branches are in intimate contact with the discomalleolar ligament that enters the middle ear through the petrotympanic fissure and with the external ear through the most external branches in the scamotympanic fissure. They show that the intimate relationship between the TMJ and the middle ear and in presence of secondary reflex vascular contraction by functional or inflammatory articular disorders could explain the referred otic symptoms.114 Reflex One of Costen’s hypotheses28 associated otologic symptoms with abnormal amounts of auriculotemporal nerve (V3) compression by the TMJ in the posterior and medial portion of the gleniod cavity. He confirmed that its medial and posterior path to the condylar head could project otic symptoms. The mechanical compression exerted near the chord tympani (that emerges from the medial area of petrotympanic fissure and then unites the lingual nerve17,107,130) and the symptoms referred to the tongue were equally related. He postulated that aural symptoms were the result of Eustachian tube’s compression because of the relaxation of the superior head of the external pterygoid muscle and the internal pterygoid muscle that occurs with the posterior condylar movement that then produces a loss of vertical dimension.28,29,131,132 Ash and Pinto32 explain that it cannot be excluded that an abnormal anatomical position of the jaw secondary to a diminished vertical dimension in dentate and edentulous patients could indirectly occlude the membranous area of Eustachian tube as a result of compression of the muscular mass and associated structures in relaxation or muscular hypotension. Costen stated that the occlusion of the Eustachian tube changes the intratympanic pressure that could generate vertigo. Kelly133 found a relevant causal association among vertigo, nausea, vomit and syncope in 105 patients with over-closed dental relation and found the complete resolution of their symptomatology in 89% of these patients at increasing it. In relation to the possible compression of the retrodiscal structures because of the posterior movement of the condyles, it is important to note that in healthy articulation this posterior movement is limited by the temporomandibular ligament (Figure 2). This is a strong ligament without elastic fibers that maintains the condyle, disc and temporal bone firmly opposed, even restricting the most posterior condylar position in the TMJ. This ligament is composed of horizontal and oblique portions. The horizontal portion restricts the posterior movement of the condyle and is assisted partially by the oblique portion.4 In situations in which the partial and total edentulism and the advanced tooth attrition permit the abnormal closing of the jaw, the condylar movement could generate mechanic compression of the auriculotemporal nerve (transits posteroinferior to the condyle) in abnormal articulations by elongation of this ligaments. Figure 2. A. Horizontal Portion to Condyle and Disc of the Temporomandibular Ligament, B. Oblicous Portion of the Temporomandibular Ligament , C. Auriculotemporal Nerve. Modified from: Okeson JP. Managment of temporomandibular disorders and occlusion. 4th Ed, The CV Mosby Publishers, St. Louis, MO, 1998. Page 15 In 1943, Sicher,134,135 among other anatomists, argued that these hypotheses were incorrect, although they didn’t deny the possibility of considering them. More than half a century later, in 1990, Johansson123 carried out histological and radiographic studies that corroborated not only the compression of the auriculotemporal nerve in luxated disk articulations, but also the probable compression of the masseteric nerve, the branches of the deep posterior temporal nerves and the possible compression of the lingual and inferior alveolar nerves in some luxated articulations. In articulations with disc luxation, the retrodiscal vasculo-nerve plexus is compressed where the auriculotemporal nerve is included. The auriculotemporal nerve profusely innervates the articulation as well as innervating the tympanic membrane, the anterosuperior zone of the external ear, the tragus and the external part of the ear upon it, among other structures. The retrodiscal zone has been extensively studied136,137,138,139 and similarly confirms that adaptive inflammatory changes occur because of discal luxation and the presence of mechanical force in the retrodiscal vascular and nervous system. In his study Johansson123 explained that in the nervous entrapment etiology is important not only to anatomical mobility and bone deformities but also inflammation of vascular and muscular structures that can injure closely situated nerves117 since inflammation can alter and reduce the normal contour and size of the anatomical passages. Theory of Hypertonicity: In relation to the muscular dysfunctional spastic contraction Marasa96 in 1988, and Youniss8 in 1993, suggested that the internal pterygoid muscle hypertonicity observed in TMD could externally compress the tensor veli palatini muscle, as well as cause anatomical interferences of the normal function of Eustachian tube, generating audiologic symptoms. Normally the Eustachian tube is maintained closed by the collapsing pressure of the external mass which is composed of structures like the internal pterigoid muscle in the lateral zone, the levator palatini muscle in the inferior zone and the Ostmann’s fat pad in the internal zone. Under normal conditions the contraction of the tensor veli palatini muscle opens the lumen of the Eustachian Tube while it presses laterally the internal pterygoid muscle.140 If the internal pterygoid muscle is hypertonic, it interrupts the contraction of the tensor veli palatini muscle causing difficulty in opening the Eustachian Tube.141 If the mastication muscles are hypertonic because of TMD, it is also possible that the tensor veli palatini is hypertonic as well because of the common innervation by the of V3. As the tensor veli palatini remains spastic, its normal function of opening and closing the Eustachian Tube will cease. High, Narrow, Arched Palate Theory Marasa and Ham96 in 1988 proposed that the long, high, narrow palate concavities in children contribute to anatomical changes like internal rotation of the palatini and maxilar bones that modify the peripherical muscular efficacy and its relation with the Eustachian Tube, generating aural symptoms and otitis media with effusion. The higher the separation and extension of the pterygoid plate and the pharingeal tubercle in high, narrow and arched palates, because of internal rotation of the palatini and maxillar bone, the higher the tension in the superior fibers zone of the superior pharingeal constrictor muscle that tightens the pharynx concavity by elevating it in relation to the Eustachian Tube. This raises the inferior and medial pressure generated over the Eustachian Tube, producing a blockage in the Eustachian Tube. Consequently they suggested that in high, narrow arched palates the contraction of the tensor veli palatini will have to be higher to move the palatine aponeurosis due to the longer axial length that reduces the efficacy of this muscle to open the Eustachian Tube. They state that the nasopharyngeal constricted airway seen in high vaulted palate of thumb-sucking children (initiating and perpetuating habit in TMD)could narrow it, also the presence of enlarged tonsils and adenoids, can block the Eustachian Tube. Otic Ganglion's Theory: An auriculotemporal nerve lesion not only involves the preganglionar sensorial fibers of this nerve but also the secretomotor component of the parotid gland which is generated by parasympathic postganglionic fibers of the glosopharingeal (IX). It also involves the sympathic postganglionar component of the blood vessels and sweat glands in the skin, which are innervated by this component. The sympathetic fibers in the TMJ also contribute to the articular inflammation increasing the activity of these postganglionic sympathetic nervous fibers in TMD.142 Ash and Pinto32 relate the aural symptomatology, explaining that the parasymphatic nervous fibers of the otic ganglion that come from the glosopharingeal nerve (tympanic plexus) through the small petrosal nerve, reach the TMJ in its route with the auriculotemporal nerve. When this is irritated it can produce a reflex vascular spasm in the labyrinthine system of the internal ear, which is secondary to abnormal stimulation of these fibers to the tympanic plexus and is associated with TMD.82,143,144 Since 1934, Costen28 related the neuralgic glosopharingeal etiology in articular pathologies to the irritation of its sensorial connections in the IX pair of the otic ganglion. Cochlear Associated Innervation Theory Vass and Col.145 found that in animals the trigeminal innervation of the vascular system controls the cochlear and the vestibular labyrinth. This innervation is found specifically in the modiolar artery and in the septum interscala giving a rich vascularization to the stria vascularis, where the endolymph that maintains the ionic and fluid balance of the cochlea is produced. They also found this innervation in the ampullar crest of the vestibular labyrinth but neither in its neuroepithelium nor in the semicircular canals. The projection of the ophtalmic fibers of the trigeminal Gasser ganglion to the cochlea, through the basilar and anterior inferior cerebella arteries, can play an important role in its vascular tone in quick vasodilatatory responses of the inner ear face to metabolic stresses like intense noise. Inner ear pathology which produces aural symptoms such as sudden hearing loss, vertigo and tinnitus can originate from the reduction of the cochlear blood flow because of the presence of abnormal activity in the trigeminal ganglion in patients with herpes zoster, migraine or by central excitatory effect caused by chronic or deep pain. The authors also found that the trigeminal sensorial innervation plays an important role in the regulation and balance of the cochlear vascular tone and in the vestibular labyrinth canal that can be responsible of the symptomatic complexity of some cochlear diseases related to inner ear blood flow. They also state that cephalalgia in cluster headaches, tinnitus, hearing loss, vertigo and Meniere’s Syndrome can have a similar relation (and can be explained by this innervation. Articular Inflammatory Pattern's Theory: Myers,124 in 1988, suggests that in articulations with luxated disks chronic inflammation is generated.125 Inflammation is generated because of vascular damage that produces edema, vascular leakage and fibrosis that extends into neighboring areas following the patterns of smallest resistance generated in the activity of the muscular masses, especially in medial and anterior-medial areas of the TMJ (Figure 3). When edema takes place in the anterior-medial area, localized between the internal and external pterygoid muscles, it can cause inflammatory compression of the alveolar, lingual, chord tympani nerves and the middle meningeal artery. Figure 3. Possible Medial Inflammatory Paths from the TMJ in Inflammatory Disorders. Modified form: Myers LJ, DDS. Possible inflammatory pathways relating temporomandibular joint dysfunction to otic symptoms. The J Craniomand Prac. January 1988, Vol. 6(1): 65-70 When edema moves to the medial area it can take two patterns. One pattern runs posterior, surrounding the styloid process following the facial tissues in a distal and caudal direction to the area of the internal carotid artery, the jugular vein and the hypoglossal and glosopharyngeal nerves (carotid sheath region). The second pattern is directed to the carotid sheath, generating fibrosis and adhesions that produce tension in the carotid sheath with the jaw and neck movements. This tension is transmitted to the jugular foramen and to the endolymphatic sack, generating pressure over the hair cells of the cochlea producing tinnitus and vertigo. A third pattern is described which passes between the origin of the levator palatini muscle and the tensor veli palatini muscle, which form a space along with the apex of the isthmus of the Eustachian tube, allowing edema and fibrosis to go toward the most vulnerable area (isthmus) because of its narrow lumen that can be pressed, lightly closing the isthmus and generating otological symptoms of fullness and otitis media. Myers demonstrates the fragility of the extrabony extensions of the middle ear in the Eustachian tube and of the internal ear in the endolymphatic sack. He suggests that Meniere's Syndrome (increased endolymphatic pressure) involves the transitory or permanent impairment of hearing, tinnitus and vertigo and has an etiologic explanation in this theory. Heterotopic Pain Theory - Convergence Miller and Wyrwa43 demonstrate that in the "theory of the convergence," studied by Sessle,146,147,148,149 the pain referred to the ear, secondary to a orofacial pathology150 and a chronic painful stimuli alters the normal physiologic functioning of the brain and sensitizes the Central Nervous System (CNS) from the sensitization of the Peripheral Nervous System (PNS). The sensorial innervation of the ear and periaural region is derived form cranial nerves V, VII, IX, X, C2, and C3. These nerves receive peripheral nociceptive impulses to the second-order neurons through the trigeminal subnucleus caudalis.120 The neurons of the spinal nucleus of the trigeminal nerve in the brain stem, particularly in the subnucleus caudalis and the transition zone between caudal and interpolar subnucleous, receive these craniofacial afferents nociceptive signals.22,151 The central sensitization also involves spinal motor neurons, the thalamus and the somatosensorial cortex. The “convergence” of these afferent nerves toward the spinal nucleus of the trigeminal and lately the thalamus and the cortex can confuse the brain in the appreciation of the sources of peripheral chronic pain by the sensation of afferent interneurons not related. Okesson4 affirms that if the pain stimuli is continuous it gives place to an accumulation of neurotransmitter substance in the interneuronal synapses, leading to the leakage of this chemical substance toward groups of adjacent interneurons being modulated by the action of these neurotransmitters, generating in the brain the perception of these impulses like coming from the same pain area. Explain that the excited original neuron gives information about the real origin of pain (primary pain), but the other neuron only shows central excitement, then the pain perceived from this neuron is a heterotopic pain, particularly a referred pain.146 Woolf et al.152 assert that the pathogenicity of pain is in part a reflex of the CNS neurons’ capacity to suffer dynamic alterations in the properties of response and that the nociceptive fibers can trigger this functional plasticity. Chronic pain brings out, as a consequence, a reduction in the threshold of the cutaneus afferent ways and an expansion of the peripheral response. The repeated peripheral stimuli of primary afferent fibers, the pain receptors, produces a progressive increase in the action potential discharge and in the same manner a prolonged enlargement in the excitability of spine and brain stem neurons posterior to the deep and chronic pain stimulus. Coderre et al.153 sustain that it is possible that the normal pain inhibition process154 in the brain stem is altered by peripheral pain reception and the central sensitization process generating expansion of the perceived peripheral pain. Bjorne and Col.56,57 describe a type of vertigo and tinnitus without a cochlear and labyrinth origin. They assert that these symptoms can be unchained in the facial and cervical muscular dysfunction in TMD, which generates hypertonicity and muscular spasm irritating nerves and blood vessels by muscular trapping. When this compression develops in the neck, it distorts the normal propioceptive reception to the vestibular nucleus in the oculo-vestibular muscle reflex that controls the postural position of the head.132 They affirm that constant muscular tension is associated with tinnitus and vertigo by neuroplasticity originating in irritation and posterior peripheral sensitization. Theory of Lability in the Internal and Middle Ear Stability: In 1964, Myrhaug79 suggests a theory that states that the equilibrium of the ossicular chain, tensor tympani muscle and stapedial muscle (antagonistics) depends on the normal functioning of the structures that lead sound into the middle ear. He affirms that in TMD, the sustained reflex contraction of these muscles can alter the endolimphatic pressure through the transmitted changes from the oval window to the labyrinth walls. This can unchain and unbalance the vestibular impulses and a symptomatologic reaction similar to Meniere’s Syndrome can develop. He also affirms that the tympani chord (VII) can be mechanically irritated in its path between the hammer and the incus by an existing reflex contraction of the tensor tympani muscle and that it can modify the positions between both of the oscicular structures, permitting the episodic or sustained contusion of this nerve and its corresponding sensorial expression projected to the tongue as an alteration of tasting sensation, a metallic taste and a burning sensation. It is important to mention that the tympani chord contains preganglionar parasympathic fibers of a secretor nature that correspond to the submaxilar, sublingual and accessories glands that when irritated can explain the variable salivate flow observed in patients with TMD. (Figure 4) DISCUSSION TMD in their acute and chronic states can come to seriously affect social life, labor performance and life quality. and perpetuating causes increase the biomechanics and the neuromuscular factors. The interdisciplinary handling is mandatory in the differential diagnosis of TMD and the golden rule for the detection of these and related symptoms is the oral clinical exam. The pain present in TMD is like a mystery where the symptoms characterize the clues and the current epidemiological information and a good clinical exam gives support for where this mystery is armed and takes form. Sometimes it is necessary to be ready to renounce some of the procedures and theories accepted as paradigms in professional practice. Only the flexible use of refreshing new knowledge and adoption of a new direction will benefit our patients, and diminish the unavoidable uncertainty of our daily practice. Many of these theories are not possible to prove using measuring instruments, but in the daily clinical practice they are constantly applied. Consten’s 1934 positions are regularly applied and seem to be the correct vision of TMD and their causal association with referred symptomology. Even after 68 years these theories seem applicable in the explanation of the craneofacial symptoms. The investigators that lean on anatomical and physiological exploration in their daily clinical practice have given form to each one of these theories. These theories should be kept in mind as diagnostic tools as they are the best understanding we currently have of the etilogy and pathogenicity of these disorders. A B The causal relationship of heterotopic pain (aural symptoms, migraines, miofascial pain) to the masticatory system is found in large numbers of adult patients as well as in the infantile population.) Although the cause-effect relationship has a significant association in TMD, continuous study is still needed. It seems that for the development of TMD is necessary a multifactorial model centered in local, systemic and recent psychological factors. Predisposition, initiator Figure 4. A. Equilibrium of ossicular chain in middle ear zone. B. Incus and malleus trespassed by the Chorda Tympani nerve. Modified modified from: Myrhaug H. The incidence of the ear symptoms in cases of malocclusion and temporomandibular joint disturbances. Br J Oral Maxillofac Surg 1964;2(July):28-32 Kuttila S. MD; Kuttila M. DDS,PhD. Aural Symtoms and Signs of Temporomandibular Disorder in Association with Treatment Need and Visits to Physician. Laryngoscope 109: October 1999;1669-73 2 Kuttila S. MD; Kuttila M. DDS,PhD. Secundary otalgy in adult population. Archives of otolaryngologic head and neck surgery. April 2001. Vol 127:401-405. 3 Gelb H. Tarte J. A two-year dental clinical evaluation of 200 cases of chronic headache: the craniocervical-mandibular syndrome. JADA 1975;91:1230-6 4 Okeson JP, ed. Managment of temporomandibular disorders and occlusion. Ed 4, St. Louis: Mosby,1998 5 Gelb H. Syndromes of the head and neck of dental origin. Arch Otolaryngol 1959;70:681-691 6 Moncayo S. y Col. Desordenes Temporomandibulares. 1 Ed, Diciembre 1998. Editorial Graficas Jes. 7 Skeppar J, DDS. Treatment of craniomandibular disorders in children and young adults. J Orofacial Pain 1993;7:362-369. 8 Youniss S, DDS. The relationship between craniomandibular disorders and otitis media in children. The J Craniomandib Pract. April 1991, Vol.9 No.2: 169-173 9 Zamburlini I.,DMD. Long-term results of appliance therapies in anterior disk displacement with reduction: A review of the literature. The J Craniomandib Pract. October 1991,Vol.9(4):361-367. 10 McNeill C, DDS. History and evolution of TMD concepts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;83:51-60 11 Dao TT. Gender differences in pain. J Orofac Pain 2000;14:169-184 12 Klausner JJ. Epidemilogic of chronic facial pain: diagnostic usefulness in patient care: J Am Dent Assoc 1994, 125:160411 13 Solberg WK. Prevalence of mandibular dysfunction in young adult. JADA,1979;98:25-34. 14 Kato T, Rompre R. Sleep bruxism: and oromotor activity secondary to micro-arousal. J Dent Res 80(10):1940-1944, 2001 15 Greene CS, Laskin DM. Temporomandibular disorders: Moving from a dentally based to a medically based model. J Dental Res. 79(10):1736-1739, 2000 16 Greene CS,DDS, Marbach JJ, DDS. Epidemiologic studies of mandibular dysfunction: A critical review. J Prosthet Dent August 1982. Vol 48,2:184-190. 17 MacKinnon, Morris. Oxford Anatomia funcional. Vol 3 Cabeza y Cuello. Panamericana. 18 Bernstein JM. Temporomandibular joint dysfunction masquerading as disease of ear, nose and throat. Trans Am Acad Ophthalmol Otolaryngol 1969;73:1208-1217. 19 Hellstrom F., Thunberg J. Elevated intramuscular concentration of bradykinin in jaw muscle increases the fusimotor drive to neck muscles in the cat. J Dent Res 79(10):1815-1822,2000 20 Curtis AW. Miofascial pain-dysfunction syndrome: the role of non-masticatory muscles in 91 patients. Otolaryngol Head Neck Surg 1980;88:361-367 21 Candido dos Reis A. DDS, Takami H. DDS. Ear Symptomatology and occlusal factors: A clinical resport. J Prosthet Dent January 2000. Vol 83. 1: 21-24 22 Santander H, DDS, Millares R, DDS. Influence of stabilization occlusal splint on craniocervical relationships. Part II: Electromiographic analysis. Cranio 1994 Oct;12(4):227233 23 Cooper BC, Koper DL. Recognizing otolaryngologic symptoms in patients with temporomandibular disorders. J Craniomand Pract 1993;11:260-67 24 Keersmaekers K, De Boever JA, Van Den Verg L. Otalgia in patients with temporomandibular joint disorders. J Prosthet Dent 1996;75:72-76. 25 Edmeads J. The cervical spine and headache. Neurology 1988;39:1874-8 (1988;38(12):1874-8) 26 Mense S. Nociception form skeletal muscle in relation to clinical muscle pain. Pain 1993;54:241-89 1 27 Parker WS, Chole RA. Tinnitus, vertigo and temporomandibular disorders. Am J Orthod Dentof Orthop 1995;107:153-58 28 Costen , J.B. A syndrome of ear and sinus symptoms dependent upon disturbed function of the temporomandibular joint. Ann Otol 43:1 March 1934:1-15 29 Shapiro HH, Truex RC. The temporomandibular joint and the auditory function. J Am Dent Assoc 1943;30:1147-1168 30 Moses JJ, DDS. A functional approach to the treatment of temporomandibular joint internal derangement. J Craniomandib Disord Facial Oral Pain 1991;5:19-27. 31 Rubinstein B, DDS. Prevalence of signs and symptoms of craniomandibular disorders in tinnitus patients. J Craniomandib Dis Facial Oral Pain 1990;4:186-192. 32 Ash CM,DDS, Pinto OF, CD.MS. The TMJ and the middle ear: Structural and functional correlates for aural symptoms associated with temporomandibular joint dysfunction. Int J Prosthodont 1991;4:51-57. 33 Rodriguez Vazquez JF A study of the os goniale in man. Acta Anat (Basel) 1991 142:188-92 34 Rees LA. The structure and function of the mandibular joint. Br.Dent J 96(1954):125 35 Youdelis RA. The morphogenesis of the human temporomandibular joint and associated structures. J Dent Res 45(1966):182-191 36 Schames J, Schames M. Trigeminal Pharyngioplasty: Treatment of the forgotten accessory muscles of mastication which are associated with orofacial pain and ear symptomatology. American Jouranal of Pain Management Vol.12 No.3 July 2002 37 Misurya VK, MB,BS,DOMS,DMS. Functional anatomy of tensor palati and levator palati muscles. Arch Otolaryngol Vol.102, May 1976:265-270 38 Perry HT, DDS,MSD,PhD, Xu Y, DDS. The embryology of the temporomandibular joint. The Journal of Craniomandib Pract. March 1985-may 1985. Vol 3(2):125-132. 39 Thilander B, Carlsson GE. Postnatal development of the human temporomandibular joint. Acta Odontol Scand. 34, 117-126, 1976. 40 Sadler TW. Langman Embriología médica Séptima edición. Capítulos 16, 17. Editorial médica Panamericana. Impreso en México, 1998. Páginas 229 a 335. 41 Yoshikuni OHTA. Development and histology of fibrous architecture of the fetal temporomandibular joint. Okajimas Folia Anat Jpn 70(1):1-6, May 1993. 42 Wong GB. Morphology of the developing articular disc of the human temporomandibular joint. J Oral Maxillofac Surg 43(1985):565-569 43 Miller DA, Wyrwa EB. Ear pain: A dental dilema. Compend Contin Educ Dent 1992;13:676-684 44 Koskinen J. Otological manifestations in temporomandibular joint dysfunction. J Oral Rehabil 1980;7:249-254 45 Bush FM. Tinnitus and Otalgia in temporomandibular disorders. J Prosthet Dent 1987;58(4):495-8 46 Lockwood AH. The functional neuroanatomy of tinnitus . Evidence of limbic system links and neural plasticity. Neurology 1998;50:114-120 47 Vergara RM. Audición y sordera. LERNER LTDA, DRG 2000 LTDA. Primera Edicion. 1996. Colombia 48 Morgan DH. Tinnitus of TMJ: A preliminary report. J Craniomandib Pract, 1992;10(2):124-129 49 Rubinstein B. Effects of Stomatognathic treatment on tinnitus: A retrospective study. Cranio 1987;5:254-9 50 Vernon J, Ph D. Attributes of tinnitus that may predict temporomandibular joint dysfunction. The J Craniomandib Pract October 1992, Vol 10 (4):282-288. 51 Chole RA. Tinnitus and vertigo in patients with temporomandibular disorders. Arch Otolaringol Head Neck Surg. 1992;118(8):817-21. 52 Lam DK. Lawrence H. Aural symptoms in temporomandibular disorder patients attending a craniofacial pain unit. J Orofac Pain 2001;15:146-57. 53 Rubinstein B. Tinnitus and craniomandibular disorders: Is there a link? Swed Dent J 1993;95:1-46 54 Cooper BC, Alleva M. Miofascial pain dysfunction: Analysis of 476 patients. Laryngoscope 1986;96:1099-1106. 55 Hazell JWP. Patterns of tinnitus: Medical audiological findings. J Laryngol Otol 1981 (4):39-47 56 Bjorne A. Craniomandibular disorders in patients with Meniere’s disease: a controlled study. J Orofacial Pain 1996;10:28-37 57 Bjorne A. Cervical signs and symptoms in patients with Meniere’s disease: a controlled study. J Craniomandib Pract 1998;16;3:194-202 58 Gelb H. Calderone JP. The role of the dentist and the otolaringologist in evaluating temporomandibular joint syndromes. J Prosthet Dent 1967;18:497-503. 59 Suk Kim H, DDS. Pain-pressure threshold in the head and neck region of episodic tension-type headaches patients. J Orofacial Pain 1995;9:357-364 60 Raustia AM. DDS,PhD. Parotid gland carcinoma simulating signs and symptoms of craniomandibular disorders- A case report. The J Craniomandib Pract April 1993, Vol.11(2)153156 61 Kronman JH. Bursitis of the tensor veli palatini muscle with a osteophite on the pterygoid hamulus. Oral Surg 1991;71:420-2 62 Salins PC. Bursitis: a factor in the differential diagnosis of orofacial neuralgias and myofascial pain dysfunction syndrome. Oral Surg 1989;68:154-7 63 Noone RB. The effect of middle ear disease of fracture of the pterygoid hamulus during palatoplasty. Cleft Palate J 1973;10:23-33 64 Hertz RS. Pain resulting fm elongated pterygoid hamulus: Report of case. Oral Surg 1968;26:668-90 65 Wooten JW. The pterygoid hamulus: a possible source of swelling, erythema and pain: report of three cases. J Am Dent Assoc 1970;81:688-90 66 Brook IM.Pterygoid hamulus hyperawareness. Br Dent J 1982 Aug 17;153(4):150 67 Shankland WE, DDS, MS. Pterygoid hamulus bursitis: one cause of craniofacial pain. J Prosthet Dent 1996;75:205-10 68 Shankland WE, DDS, MS. Bursitis of the hamular process. Part I: Anatomical and histological evidence. The J Craniomandib Pract July 1996, Vol 14,NO 3:186-189. 69 Shankland WE, DDS, MS. Bursitis of the hamular process. Part II: Diagnosis, treatment and report of three cases studies. The J Craniomandib Pract July 1996, Vol 14,NO 4:306-311. 70 Shankland WE, DDS, MS. Ernest syndrome as a consecuence of stylomandibular ligament injury: A report of 68 patients. J Prosthet Dent April 1987, Vol.57(4):501-506. 71 Correll RW. Mineralization of the stylohyoid-stylomandibular ligaments complex. Oral Surg 1979;48:286-91 72 Sandoval GP, MD. Proceso estiloideo elongado y síndrome de eagle..Acta de otorrinolaringología y cirugía de cabeza y cuello. Dic 2001. Vol 29, 4:171-177 73 Ernest EA,DMD. Photomicrogrphic evidence of insertion tendonosis: The etiologic factor in pain for temporal tendonosis. J Prosthet Dent 1991;65:127-31 74 Peterson JN, DDS, Schames J, DMD. Sphenopalatine ganglion block: A safe and easy method for the management of orofacial pain. The J Craniomandib Pract July 1995,Vol.13(3):177-181 75 Kunachak S. Anterior cervical pain syndromes: hyoid, thyroid, and crycoid cartilages syndromes and their treatment with triaminalone acetamide. J Laringol Otol 1995;109:49-52 76 Koelbaek JM. Generalised muscle hyperalgesia in chronic whiplash syndrome. Pain 1999;83:229-234 77 Steinmann EP. A new light on the pathogenesis of the styloid syndrome. Arch Otolaryngol 91:171, 1970 78 Manni A, Brunori P, Giuliani M, Modoni M, Bizzi G. Otovestibular symptoms in patients with temporomandibular joint dysfunction. Electromyographic study (Abstract). Minerva Stomatol 1996 Jan-Feb;45(1-2):1-7 79 Myrhaug H. The incidence of the ear symptoms in cases of malocclusion and temporomandibular joint disturbances. Br J Oral Maxillofac Surg 1964;2(July):28-32 80 Ciancaglini R, MD,DMD, Loreti P. MD,DMD. Ear, nose and throat symptoms in patients with TMD: The association of symptoms according to severity of arthropathy. J Orofacial Pain 1994;8:293-297. 81 Campbell CD. Loft GH. TMJ symptoms and referred pain patterns. J Prosthet Dent April 1982 Vol.50(47).Num 4. 82 Eckerdal O. The petrotynpanic Fissure: A link connecting the tympanic cavity and the temporomandibular joint. The J Craniomand Pract. 1991 Vol 9(1):15-21 83 Greene C.S,DDS. The etiology of temporomandibular disorders: Implications for treatment. J Orofacial Pain soportados por evidencia científica Vol 15(2):93-105, 2001 84 Virtanen H.Objective tubal tinnitus: a report of two cases. J Laryngol Otol 1983 Sep;97(9):857-62 85 Zipfel TE, Kaza SR, Greene JS. Middle-ear myoclonus. J Laryngol Otol 2000 Mar;114(3):207-9 86 Klockholff IH. Reflex activity in the tensor tympani muscle recorded in man. Acta Oto-laryngologica 51(1960):184-188 87 Kamerer DB. Electromyographic correlation of tensor tympani and tensor veli palatini muscles in man. Laryngoscope 1978;88:651-662 88 Gray LP.The relationship between the “superior constrictor swallow” clicking of the ears and ear disease. J Laryngol Otol 1983 Dec;97(12):1121-8 89 Travell JG, Simons DG: Dolor y disfuncion miofascial. El manual de los puntos gatillo, Mitad superior del cuerpo. Vol 1 Segunda Edición. Editorial Panamericana 2002. 90 Ogutcen-Toller M. Audiological evaluation of the aural symptoms in temporomandibular joint dysfunction. J Craniomaxillofac Surg 1993 21:2-8 91 Spauwen PH, Hillen B, Lommen E, Otten E.Threedimensional computer reconstruction of the eustachian tube and paratubal muscles.Cleft Palate Craniofac J. 1991 Apr;28(2):217-9 92 Ishijima K. Functional anatomy of levator veli palatini muscle and tensor veli palatini muscle in association with eustaquian tube cartilage. Ann Otol Rhinol Laryngol June 2002;111(6):530-536 93 Misurya VK.Tensor tympani, a 'tuner' of tensor palati muscle. Acta Otolaryngol 1976 Nov-Dec;82(5-6):410-4 94 Swarts JD, Rood SR. The morphometry and threedimensional structure of the adult eustachian tube: implications for function. Cleft Palate J 1990 Oct;27(4):374-81 95 Alper CM, Tabari R, Seroky JT, Doyle WJ.Magnetic resonance imaging of the development of otitis media with effusion caused by functional obstruction of the eustachian tube. Ann Otol Rhinol Laryngol 1997 May;106(5):422-31 96 Marasa F. Case reports involving the treatment of children with chronic otitis media with effusion via craniomandibular methods. J Craniomandib Pract, 1988;6:256-270 97 Holborow C. Eustaquian tubal function: changes throughout childhood and neuro-muscular control. J Laryngol Otol 1975;89:47-55 98 Arlen H. The otomandibular síndrome: A new concept. Ear Nose Throat J 1977;56:60-62 99 Rood SR, Doyle WJ. Morphology of the tensor veli palatiny, tensor timpani and dilatator tubae muscles. Ann Otol Rhinol Laryngol 1978;87:202-210 100 Gray, Henry. Anatomy of the human body. Philadelphia: Lea Lea & Febiger, 1918 20th ed. 101 Prades JM, Dumollard JM. Descriptive anatomy of the human auditory tube. Surg Radiol Anat 1998;20(5):335-40 102 Rood S. The morphology of m.tensor veli palatini in the five month human fetus. Am J Anat 138:191-196,1973 103 Salen B, Zakrisson JE. Electromyogram of the tensor tympani muscle in man during swallowing Acta Otolaryngol 1978 May-Jun;85(5-6):453-5. 104 Barsoumian R, Kuehn DP, Moon JB, Canady JW.An anatomic study of the tensor veli palatini and dilatator tubae muscles in relation to eustachian tube and velar function. Cleft Palate Craniofac J 1998 Mar;35(2):101-10 105 Kierner AC, Mayer R, v Kirschhofer K. Do the tensor tympani and tensor veli palatini muscles of man form a functional unit? A histochemical investigation of their putative connections. Hear Res 2002 Mar;165(1-2):48-52 106 Proctor B. Embriology and anatomy of the eustaquian tube. Arch Otolaryngol 86:503-514,1967 107 Pinto OF. A new structure related to the temporomandibular joint and middle ear. J Prosthet Dent 1962;12(1):95-103. 108 Komori E, Sugisaki M, Tanabe H. Discomalleolar ligament in the adult human. Cranio 1986;4:300-305 109 Rodríguez-Velasquez JF. Anatomical considerations on the discomalleolar ligament. J Anat 1998;192:617-621. 110 Loughner BA, Larkin LH. Discomalleolar and anterior malleolar ligaments: Possible causes of middle ear damage during temporomandibular joint surgery. Oral Surg Oral Med Oral Pathol 1989;68:14-22 111 Rodriguez Vazquez JF. Relationships between the temporomandibular joint and the middle ear in human fetuses. J Dent Res. 72(1):62-66, January, 1993. 112 Douglas H. Morgan, D.D.S., The TMJ-Ear Connection. Journal of Craniomandibular Practice Vol. 13, No. 1, 1995 113 Ioannides CA. The disco-malleolar ligament: A possible cause of subjective hearing loss in patients with TMJ. J Maxillofac Surg 1983;11:227-231 114 Merida Velasco JR, Rodriguez Vazquez JF, Jimenez Collado J. Anterior tympanic artery: course, ramification and relationship with the temporomandibular joint. Acta Anat 997;158(3):222-6 115 Coleman RD. Temporoamndibular joint. Relations of the retrodiscal zone to meckel’s cartilage and lateral pterygoid muscle. J Dent Res 49(1970):626-630. 116 Hoshino T Surgical anatomy of the anterior epitympanic space. Arch Otolaryngol Head Neck Surg 1988 Oct;114(10):1143-5 117 Burch JG. The cranial attachment of the sphenomandibular (tympanomandibular) ligament. Anat Rec 1966;156:433-437 118 Ogutcen-Toller M. The morphogenesis of the human discomalleolar and sphenomandibular ligaments J Craniomaxillofac Surg 1995 Feb;23(1):42-6. 119 Rodriguez Vazquez JF. Development of the human sphenomandibular ligament. Anatomical Rec 1992;233:453460 120 Okeson ,J.P.: Orofacial pain. Guidelines for assessment, diagnosis, and management. The American Academy of Orofacial Pain. Quintessence, Chicago, 1996. 121 Coleman RD. Temporoamndibular joint. Relations of the retrodiscal zone to meckel’s cartilage and lateral pterygoid muscle. J Dent Res 49(1970):626-630. 122 Ramfjord S, LDS,MS,PhD, Ash MM, BS,DDS,MS Occlusion, 3rd ed W.B Saunders Company. 1983 123 Johansson AS, DDS. A radiographic and histologic study of the topographic relations in the temporomandibular joint region. J Oral Maxilofac Surg 48:953-961, 1990 124 Myers LJ, DDS. Possible inflammatory pathways relating temporomandibular joint dysfunction to otic symptoms. The J Craniomand Prac January 1988, Vol 6(1): 65-70 125 Luder HU. Articular degeneration and remodeling in human temporomandibular joints with normal and abnormal disc position. J Orofacial Pain 1993;7:391-402 126 Schaefer JR. Pressure-pain thresholds and MRI effusions in tmj artharlgia. J Dent Res 80(10):1935-1939, 2001 127 Libin BM. The cranial mechanism: Its relationship to craniomandibular function. J Prosthet Dent 1987;58:632-638 128 Burch JG.. Activity of the accesory ligaments of the temporomandibular joint. J Prosthet Dent 24:621-628. 1970 129 Merida-Velasco JR. The vascualr relationship between the temporomandibular joint and the middle ear in the human fetus.J Oral Maxillofac Surg;57:146-153,1999. 130 Rohen-Yokochi. Atlas fotografico de anatomia humana. Vol.1 Cabeza, cuello y tronco. Ediciones Doyma. 1984. Pag 100 131 Dolowitz EA. The role of muscular incordination in the pathogenesis of TMJ syndrome. Laryngoscope, 1964;74:790 132 Michelotti A. Mandibular rest position and electrical activity of the masticatory muscles. J Prosthet Dent 1997;78:48-53 133 Kelly HT. Vertigo attributable to dental and temporomandibular joint causes. J Prosthet Dent 1964;1:159173 134 Sicher H.Temporomandibular articulation in mandibular overclosure. J Am Dent Assoc 36:131, 1948. 135 Sicher N. Structural and functional basis for disorders of the temporomandibular articulation. J Oral Surg 1955;12:275-279 136 Scapino RP. The posterior attachment: Its structure, function, and appearance in TMJ imaging studies. Part 1. J Craniomandib Disord Facial Oral Pain 1991;5:83-95 137 Scapino RP. The posterior attachment: Its structure, function, and appearance in TMJ imaging studies. Part 2. J Craniomandib Disord Facial Oral Pain 1991;5:155-166 138 Wilkinson TM. A histologic study of retrodiscal tissues of the human temporomandibular joint in the open and closed position. J Orofacial Pain 1994;8:7-17 139 Kino K. Reconsideration of the bilaminar zone in the retrodiscal area of the temporomandibular joint. Oral Surg Oral Med Oral Pathol 1993;75:410-21 140 Leuwer R, Schubert R, Kucinski T, Liebig T, Maier H. The muscular compliance of the auditory tube: a model-based survey. Laryngoscope 2002 Oct;112(10):1791-5 141 Ross M. Functional anatomy of the tensor palati. Arch Otolaryngol 93:1-8,1971 142 Storrs TJ. A variation of the articulotemporal syndrome. Br J Oral Surg;2:236, 1974 143 House LR. Temporomandibular joint surgery: results of a 14 years follow up study. Laryngoscope, 1984;94 (4):534-538 144 Kopp S, DDS, PhD. Neuroendocrine, immune, and local responses related to temporomandibular disorders. J Orofacial Pain 2001;15:9-28 145 Vass Z. Direct evidence of trigeminal innervation of the cochlear blood vessels. Neuroscience Vol.84(2), Feb 1998:559-567 146 Sessle BJ, Hu JW. Convergence of cutaneous, tooth pulp, visceral, neck and mussle afferents onto nociceptive and nonnociceptive neurons in trigeminal subnucleus caudalis (medullary dorsal horn) and its implications for refered pain. Pain 1986;27:219-235 147 Sessle BJ. Acute and chronic craniofacial pain: Brain stem mechanism of nocicptive transmission and neuroplasticity and their clinical correlates. Crit Rev Oral Biol Med 2000;11:57-91 148 Sessle BJ. The neurobiology of facial and dental pain, present knowledge, future directions. J Dent Res 1987;66:962-81 149 Sessle BJ. The neural basis of temporomandibular joint and masticatory muscle pain. J Orofacial Pain 1999;13(4):238-245 150 Svensson P. Craniofacial muscle pain: Review of mechanisms and clinical manifestations. J Orofacial Pain. 2001;15:117-145. 151 Calhoun KH, MD. Expert guide to otolaryngology. American College of Physicians. Philadelphia, Pennsylvania 2001 152 Woolf CJ. The induction and maintenance of central sensitizacionis dependent on N-methyl-D-aspartic acid receptor activation: Implications for the treatment of postinjury pain hypersensitivity. Pain 1991;44:293-300 153 Coderre TJ. Contribution of central neuroplasticity to pathological pain : Review of clinical and experimental evidence. Pain 1993;52:259-285 154 Wall PD. The gate control theory of pain mechanisms: A reexamination and restatement. Brain 101:1-18, 1978.