Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
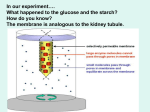
Dialysis Therapy Management ◊ Dialysis Manual Based on requirements of Maryland Board of Nursing Certified Nursing Assistant – Dialysis Technician -1- Table of Contents Background/History ............................................................................................... 3 What Is A Kidney ................................................................................................... 3 What Happens In The Kidney ................................................................................. 3 What Happens When The Kidneys Fail? ................................................................... 4 Dialysis ................................................................................................................. 4 Hemodialysis ......................................................................................................... 4 Transplantation ..................................................................................................... 6 No Option.............................................................................................................. 6 Acute Renal Failure Vs. Chronic Renal Failure .......................................................... 6 What Causes Renal Failure?.................................................................................... 7 How Do We Know That Dialysis Is Working On Our Patients? ................................... 8 Normal Values ....................................................................................................... 8 The Role Of The Dialysis Patient Care Technician ..................................................... 9 Team Members ...................................................................................................... 9 Professional Relationship Boundaries......................................................................10 Confidentiality ......................................................................................................11 Infection Control ...................................................................................................11 Handwashing........................................................................................................12 Equipment ............................................................................................................12 Safety And Environment ........................................................................................13 Mobility And Positioning ........................................................................................13 Assistive Device ....................................................................................................14 Data Collection .....................................................................................................15 How To Take These Measurements........................................................................17 Heparinization ........................................................ Error! Bookmark not defined. Complications ......................................................... Error! Bookmark not defined. Starting Or Initiating Dialysis ................................... Error! Bookmark not defined. Monitoring The Patient During Dialysis ..................... Error! Bookmark not defined. Complications ......................................................... Error! Bookmark not defined. Medication.............................................................. Error! Bookmark not defined. Reuse .................................................................... Error! Bookmark not defined. References ............................................................. Error! Bookmark not defined. -2- Background/History What is a kidney? Kidneys are incredible organs. Perhaps, more than any other organ, the kidney is the most efficient and it does several important jobs. Two of the most common are removing excess fluid and removing excess waste. They also control three hormones. One helps to regulate blood pressure, another works to control your red blood cells, and the third controls vitamin D affecting calcium absorption. Most people have two kidneys. Each weighs about 5 ounces and is about the size of your fist. They are located in the back of the body on either side of your spine, just below your waist. That position keeps them very well protected in the body. Each kidney is surrounded by a tough coating or capsule. Below the capsule is the cortex. If you were to cut a kidney in half, you would find that it is divided into several sections. The inner portion is called the medulla and is made up of several pie-shaped wedges called pyramids. The points of the “pie” are called papillae. Each papilla projects into a cup-shaped opening called a calyx. These calyces empty the urine into the renal pelvis in the lower part of your body. The renal pelvis is connected to a ureter. Both ureters empty into your bladder. The bladder holds the urine until it is emptied through the urethra to the outside the body. What happens in the kidney? Each healthy kidney has an average of one million nephrons. The nephrons are the working units for the kidney. Each nephron has a glomerulus and a tubule. A glomerulus is a twisted ball of capillaries surround by a membrane called a Bowman’s capsule. Blood is pumped from the heart and goes to the afferent arteriole of each nephron. As it passes through the glomerulus, excess fluid and poisons are removed. The cleaned blood is sent out through the efferent arteriole. These excess poisons and fluid are stored in the bladder in the form of urine. When the bladder is full, it empties outside the body and amazingly the blood is clean. Cleaning blood is the function of the kidney and most people are aware of the hormone production. This is the normal process. -3- What happens when the kidneys fail? It stands to reason that as the kidneys fail, the job they are responsible for will fall behind. Since the kidney is such an efficient organ, most patients are not aware of any problems. When the kidneys fail, the patient’s blood work will show the changes before the patient feels much of a change. Typically the creatinine and BUN value will start to rise. When this occurs it is called “uremia.” Often times the nephrologist can give the patient medications that will keep the values closer to a normal range. But these may only help a patient for several years. As the values rise and uremia becomes worse, the patient will typically lose much of his energy. Tiredness, low blood count, itching of the skin, altered coloring of the skin, loss of appetite, and generally not feeling ‘good’ are typical signs of uremia. When all of the efforts to reduce the kidney failure have not been successful, the patient must be started on some type of “Renal Replacement Therapy,” or the patient will die. When the kidneys have lost about 90% of their function the patient is taught about his four options: 1. 2. 3. 4. Hemodialysis Peritoneal Dialysis Transplantation No dialysis. Let’s look at each one. Dialysis Both types of dialysis do the same thing. They both are able to replace two of the functions of a natural kidney: removing excess fluid and removing excess poisons. There are advantages to both therapies. However, neither does as well as the original natural kidney, but they are adequate substitutes. Hemodialysis The hemodialysis type of dialysis is a process where dirty blood is taken outside the body to be cleaned and then returned back once cleaned. Two needles are placed into a patient. One is for removing the ‘dirty’ blood and the second is for returning the ‘cleaned’ blood. The ‘dirty’ blood in transported outside the body to flow through an artificial kidney. The artificial kidney filters out excess fluid and poisons from the blood. While the blood is being filtered, several technical processes are taking place. Two are most important: they are diffusion and ultrafiltration or (convection). -4- Diffusion is a process where particles go across a semipermeable membrane from an area of high concentration to low concentration. Ultrafiltration is a process where fluid is pushed across a membrane by a pressure. To understand this better, let’s break each section apart. When the blood is outside the body it filters through an artificial kidney. The artificial kidney is a plastic cylinder with several hollow fibers packed inside. Blood enters here Dialysate flows Out here Thousands of Hollow fibers Dialysate flows In here Blood leaves here clean Dialyzer Blood enters the top of the kidney and travels through the numerous hollow fibers in the dialyzer. As the blood is forced through the hollow fibers, poisons are drawn to the dialysate side of the artificial kidney. The area surrounding the hollow fibers essentially filters the blood. If you remember, diffusion, by definition, is “particles going from an area of high concentration to low concentration.” An everyday example of diffusion is when a tea bag is placed into a cup of water. The tea inside the bag will work its way out. The water will soon have lots of tea particles. This process is called diffusion. Dialysate is a solution of very few particles and the blood is full, much like the tea bag is full of tea. Therefore, poisons jump from the blood to the dialysate, like the tea moves from the tea bag into the cup of water. The dialysate that travels around outside the hollow fibers moves with pressure. This pressure inside the dialyzer or artificial kidney is called transmembrane pressure or TMP. This pressure on the hollow fibers “squeezes” the fluid from the patient, much like taking the tea bag string and squeezing the water out. Excess fluid is removed by ‘squeezing’ the fibers. 7 -5- So let’s review: dirty blood goes into the top of the dialyzer and comes out of the bottom of the dialyzer cleaned. While inside two major things occur, diffusion and ultrafiltraton (UF). UF or excess fluid is removed because of the transmembrane pressure or TMP, and excess poisons are removed because of the concentration difference of the blood and the dialysate. Transplantation Transplantation is a surgical procedure where a ‘healthy’ kidney is placed inside a patient whose kidneys no longer are able to do its normal work. Once inside, this ‘new’ healthy kidney takes over the place of the ‘old’ kidney. This is the best way to replace the kidney function in a patient who has kidney failure. A healthy kidney can be donated from a family member or friend or someone who has died and has agreed to donate their organs. However, there is a chronic shortage of kidney donors. No Option Some of your patients may choose to do none of the above options. If a patient does not get transplanted or go on one of the forms of dialysis, they will die. However, for some patients, this may be a welcomed option. ACUTE RENAL FAILURE VS. CHRONIC RENAL FAILURE Renal failure is renal failure, right? Not exactly. Acute renal failure is a sudden loss of renal function that may be reversible. Chronic renal failure is almost never reversible. A patient who develops acute renal failure has a good chance of recovering his kidney function. Often times it is caused by an illness or injury that stresses the kidney. When the kidney is no longer under stress the normal function returns. If the stress does not stop, the patient will develop a chronic renal failure. Chronic renal failure takes much longer to develop. Typically, there is a slow steady loss of nephrons, the working units of the kidney. Many of your patients will show NO signs of being sick until 75% of their kidney is damaged. Some form of renal replacement therapy will need to be started when 85% is lost. -6- WHAT CAUSES RENAL FAILURE? Many things can be responsible for a patient’s loss of renal function. Diabetes is the number one cause. About 50% of patients are on dialysis because they have diabetes. The high blood sugar levels wear on the tiny blood vessels in the kidney until they can no longer carry blood efficiently. One of the first signs that a diabetic patient is developing renal failure is microalbuminuria (small amounts of protein in the urine). Diabetics should have their urine checked often to see if any protein is being “spilled out” into the urine. Hypertension, or high blood pressure, is the second most common cause of kidney failure. A blood pressure that is too high can also hurt the small blood vessels that supply the kidney. Continuous high pressure on the tiny vessels of the kidneys can destroy the kidney. Years of varying blood pressures take its toll. Glomerulonephritis is a condition that causes inflammation in the glomerulus of the kidneys. Many patients who developed this condition had a streptococcal infection in their past. Possibly they had a strept throat as a child that was never treated with antibiotics. The body’s immune system worked very hard to fight the strept infection and in doing so, this hurt some of the ‘good’ parts of the body as well. In the past several years, pediatricians have increased their practice of culturing children’s ‘sore throats.’ When strept throats are treated properly, glomerulonephritis is less likely. Polycystic kidney disease is an inherited disease that causes large, fluid-filled cysts to develop in the kidneys. These cysts eventually become so large and frequent that normal kidney function is impaired. The advantage of this type of kidney disease is that the outer shell of the kidney is not affected. This allows the other functions of the kidney to perform more easily. There are many other possible causes of renal failure. The most common causes are drug toxicity, interstitial nephritis, obstruction, lupus, cancer, AIDS, or sickle cell disease. -7- HOW DO WE KNOW THAT DIALYSIS IS WORKING ON OUR PATIENTS? There are a few tests that can be completed to measure how adequately someone is being dialyzed. Measurement of BUN, Kt/V, URR, and Creatinine are most often used. BUN (Blood Urea Nitrogen) is a measure of the amount of protein by-product in the body. When we eat foods containing protein, the body breaks it down into several useful parts and some non-useful parts or waste. Nitrogen is not a useful part, but rather a waste product. Healthy kidneys excrete this poison and, therefore, BUN levels are low. Patients with kidney failure are not able to clear the BUN. When we measure a patient’s BUN value, we can see how many of the waste products have remained. This will give us an idea of how much kidney function is working. Normal Values – 5-25 Kt/V indicates the delivered dose of dialysis. In other words, how well the patient is dialyzed. For hemodialysis a value of 1.2 or greater is ideal. For peritoneal dialysis 2.0 is the target for Kt/V. There is a long calculation to determine a Kt/V. In doing so we include what residual renal function the patient has remaining, added to a long Kt/V calculation. K = dialyzer urea clearance t = length of time on dialysis (minutes) V = patient’s urea distribution volume in milliliters (complex calculation) URR (Urea Reduction Rate) is much easier to calculate and lets us know how adequate the dialysis treatment is alone, (doesn’t add in the residual renal function). URR considers a patient’s BUN value prior to dialysis on a particular day, and then subtracts the BUN value after a dialysis treatment. To calculate: Predialysis postdialysis BUN -BUN X ----------------------------------predialysis BUN 100 65% or better is considered the best measure. Creatinine is a waste-product of muscle. Similar to BUN waste products are removed by a healthy kidney. When the kidney is sick, it is unable to remove waste products efficiently. Patients with renal failure have elevated creatinine levels because the kidney cannot remove all of the wastes. Normal value – 0.7 – 1.5 -8- THE ROLE OF THE DIALYSIS PATIENT CARE TECHNICIAN TEAM MEMBERS Dialysis can only be achieved by a multidisciplinary approach. There are several members of a dialysis team. These include the primary care nurse, primary nephrologists, nurse practitioner, social worker, dietician, and the dialysis patient care technician. The primary care nurse is responsible for supervising the patient’s care while on dialysis. He or she is ultimately responsible for the practice of a CNA-DT. You function directly under a nurse's license. Your tasks are considered ‘delegated tasks.’ This means the nurse must know you are competent in doing the task he or she assigns to you. The social worker is the one who has special training in helping the patient cope with the many changes that affect the patient’s life. They also assist patients with finding resources for many different concerns, including transportation. The dietician helps the dialysis patient decide which foods are best for their very restricted diets. Patients on dialysis have numerous dietary restrictions that can be complicated. If we remember the kidney is responsible for removing the waste products from the food we have eaten. It makes sense that limiting certain foods may be required. The nephrologist (kidney doctor) and nurse practitioner work to monitor the patient’s progress and dialysis prescription. Depending on lab results and how the patient feels, they may alter the plan of care. They also write prescriptions for patients. The technician or tech in a dialysis plays a vital role in the patient’s care. They function very similarly to a primary nurse by setting up the machine and putting the patient on dialysis. Observation skills are used when you put the patient on the machine, during the dialysis treatment, and when the patient is taken off the machine. -9- PROFESSIONAL RELATIONSHIP BOUNDARIES As a healthcare provider, it is essential that a certain level of professionalism is kept. That means acting in a professional manner. There are some expectations. To start with, patients are different, not only in obvious preferences, but our patients come from many different cultures and religions. It is your responsibility to respect their choices. One patient may not be able to attend certain dates due to religious preferences or another may not be willing to take blood transfusions. It is your responsibility to know these differences when caring for your patients. The patient’s charts should contain this information. If not, discuss with the nurse what you’ve discovered and be certain these are added to the chart. Once you know these preferences and follow them, they are to be used and discussed ONLY during your care of that particular patient. All patients have a right to privacy. Patient confidentiality is paramount. No information is to be discussed outside the setting required for caring for the patient. The only exception to this is when you discover that a patient is being abused. This needs to be reported to the nurse and then to the social worker. We will discuss confidentiality further. Organizing and prioritizing is a skill that everyone needs in his or her daily life. This is true in your dialysis position as well. Patient care is always your priority. Monitoring the patient and troubleshooting problems before they start is the best. Acting on potential problems is essential. Always try to strive and apply the skills learned during this training. For the patient’s protection and your legal protection, recognize your limitations. Most of the tasks you will be asked to do are delegated from a registered nurse. If you do not know how to do a task, it is your responsibility to speak up and let that nurse and your supervisor know. Again our goal is for maximum patient care and benefits. In doing so we will need to encourage our patients to do what is best for their health. This includes eating the prescribed diet, staying on the machine the prescribed length of time, arriving to dialysis treatments each ordered day and on-time, and promoting the patient’s independence. All of these tasks need to be completed for the patient at their own pace. Many dialysis patients are preoccupied with their health and avoid recreational activities. There are numerous benefits, for everyone, when outside interests are fulfilled. Research supports an improved quality of life when people do. I’d like to recommend that you consider something. Put yourself in the shoes of the patient. How would you like to be treated? - 10 - CONFIDENTIALITY Patient’s privacy must always be protected. If made public, patients’ health records could cause embarrassment and/or discrimination. Both the law and your job standards require confidentiality. Failure to comply with this practice may lead to disciplinary and/or legal action. Since most of our information is computerized keeping this information private may be more difficult. But keep in mind this information is PRIVATE. INFECTION CONTROL “Sterile” means free from germs. Asepsis means almost the same. When doing dialysis procedures, it is very important that the tools used are kept sterile and your technique is aseptically completed. Why? These germs or microorganisms can cause infection if allowed to get into certain areas of a patient’s body or even your body. Therefore, every effort must be made to avoid germs from entering a patient’s catheter or access it because they could cause an infection. How are organisms spread? Organisms can enter the body three different ways: direct contact, indirect contact, or by droplet. Direct Contact occurs when you touch and infected area or person, then touch an open area on your body such as your mouth, nose, cut, etc. Indirect Contact occurs when you touch doorknobs, equipment, telephones, etc that are contaminated with the germ, then touch an open area. Droplet occurs from breathing, coughing, and sneezing. This allows tiny drops of body fluids to touch or circulate to other people. So, what can you do to prevent the spread of germs? There are several things that must be done AT ALL TIMES! 1. 2. 3. 4. HANDWASH between EVERY patient! Make EVERY connection perfect. Use standard precautions with all patient body fluid contacts. This means, treat all body fluids as having the potential of being extremely dangerous. Remove gloves properly a. Peel on glove off from the wrist area and hold it in the gloved hand. b. With the ‘un-gloved’ hand, peel the second glove off by grabbing the inside area near the wrist. c. Avoid ‘snapping’ the glove. d. Discard the used gloves immediately. - 11 - HANDWASHING IS THE SINGLE MOST IMPORTANT THING YOU CAN DO TO PREVENT THE SPREAD OF INFECTION! Having said that, let’s review the proper way to wash your hands. 1. 2. 3. 4. 5. 6. Water should flow down your hands. Thoroughly cover you hands with soap and water. Vigorously rub your hands together. Scrub your hands for at least 30 seconds being certain not to forget the area under your fingernails. Dry your hands thoroughly. Turn the water off with a dry towel. Standard Precautions requires strict usage of personal protective equipment (PPE). This includes gowns that cover you made of a fabric that resists fluid absorbing and a helmet to protect parts of your face from a body fluid that could splash and gloves that protect the hands. EQUIPMENT Equipment must be cleaned between patients to avoid possible contamination. Special solutions containing different chemicals are used. 1. Dialysis machines are cleaned with a solution that is wiped over all of the front surfaces of the machine. This will remove any blood or body fluids that may have been splashed onto the machine during the previous patient’s treatment. 2. Clamp soak in a beach type solution after being used on a patient. 3. Dialysis chairs are cleaned between patients’ treatment and a new sheet is used to cover. 4. Reuse equipment is also cleaned to protect the reuse tech. - 12 - SAFETY AND ENVIRONMENT For your safety, PPE should be worn whenever there is a potential for body fluid contamination or solution exposure. However if you are exposed, your supervisor must be notified immediately. As for chemicals and cleaners, these must be handled properly meaning the way the manufacturer intended their use. If any of these chemicals get on your body, notify your supervisor. Get information from the Material Safety Data Sheets (MSDS). These standards are created to be in compliance with Occupational Safety Hazard Administration (OSHA). The MSDS contain information concerning what should be done when there are different types of exposures. An MSDS book is located on each unit. Patients occasionally become sick enough that assistance from outside the unit is necessary. When a patient’s heart stops or their blood pressure becomes so low that all interventions are not helping, the CNA-DT must call for assistance. Every unit has protocols and policies in place to manage a patient that is dieing. Always call for help in these situations. MOBILITY AND POSITIONING Whether helping a patient to a chair, out of a stretcher, into the bathroom, or out of a bed, proper body mechanics are required. If not used, you run the risk of hurting yourself. The basics of body mechanics use your own weight and muscles when moving a patient. Keeping your body’s center of gravity always in the center allows the larger muscles to do the work rather than smaller ones. When pushing an object, it is best to lean toward it. When pulling an object try to allow your body’s weight to counter balance. Hold heavy objects close to the body. Avoid jerky movements on your muscles. When standing, keep your feet shoulder-width apart and use your thigh muscles when lifting. TRANSFERRING PATIENTS Allow the patient to assist as much as possible and/or allowed. Do not transfer a patient that requires more than one person alone. WAIT for assistance. DO NOT be impatient. Lock the wheels of a chair or bed or stretcher before moving the patient and check his condition. If the patient states he or she cannot stand and needs a minute first, allow the patient that time. It will save you time in the long run. - 13 - For patients who can assist slightly, a pivot method is recommended. Have the chair and the stretcher or other chair adjacent to each other. Stand in front of the patient and help the patient stand holding under his arms. Slowly pivot the patient and yourself so that the patient’s leg back is touching the surface being used. If the patient starts to fall and you can clearly not stop the fall, try to EASE the patient to the floor or bed. This easing should help reduce injury. If the patients can do nothing for themselves, lifting the patient may be necessary. Two staff members on either side of the patient can lift under the patient’s arm and move the patient or a sheet placed under the patient may be used as a sling and two or more staff members grab the sheet and hammock the patient to the other position. Keep this in mind when transferring patients. Having a sheet or blanket underneath may help in repositioning the patient. It is much easier to grab and pull a sheet than to position yourself comfortably under a patient. After placing the patient in the position, always verify that the patient is comfortable. Placing a blanket on the patient’s lap is desired. Be certain all limbs are supported. A pillow or blanket can be used to help prop certain body areas. If the patient will remain in a bed or stretcher for an extended period of time, skin integrity must be considered. The patient is not to stay in one position for great lengths of time. This could be compared to ‘sitting on your foot.’ Allow me to explain. If you sit on your foot while on a sofa or chair, how long is that comfortable? Not long, right? After about an hour your leg hurts, your foot is falling asleep, and you’re stiff. When a patient is not able to move on their own, this occurs as well. Yet they are not able to move around when their foot falls asleep. This must be considered for patient comfort and skin integrity. ASSISTIVE DEVICES If you patient is mobile with a walker or cane, monitor their steps. Watch to see if the patients can balance himself. Allow the patient as much independence as possible, but intervene if you see that the patient could get hurt. If you patient needs to use a bedpan while on dialysis, use the same body mechanics listed above when moving the patient. When assisting the patient with the use of toilet tissue, standard precautions are to be used. The patient’s skin must be treated with care. All soiled materials should be removed. If soap and water are used, be certain it is rinsed away and dried thoroughly to prevent skin breakdown. If any open areas or reddened areas are seen, bring these to the attention of the nurse immediately. - 14 - DATA COLLECTION Several measurements must be taken to monitor your patient while on dialysis. Monitoring pulse, respiration, blood pressure, temperature, and arterial pressures help follow the patient’s progress during dialysis. The primary purpose is to secure a safe and effective treatment. Any readings that are not within the normal limits (WNL) corrected by using the methods taught during orientation. If there is no improvement, the nurse covering your group of patients must be told. There are several measures that are watched during a hemodialysis treatment. 1. Temperatures are taken prior to the initiation of dialysis and after the termination. An elevated temperature may indication inflammation and/or infection. It is expected that a patient’s temperature will increase during the hemodialysis treatment, but a temperature greater than 100o F is cause for concern and should be reported. 2. Blood pressure readings are usually monitored every 30 minutes. While fluid is being removed from a patient’s body, the blood pressure will typically decrease. This is expected. However, if the patient’s blood pressure gets too low, the heart cannot disperse the blood to all of the places it needs to be and the patient may lose consciousness or have irregular heartbeats. 3. Pulse rate is also monitored. When a patient’s blood pressure drops secondary to decreasing the fluid in the body, typically the patient’s pulse will increase. 4. Respiratory rate is monitored. Breathing 12-24 times a minute falls within a normal range. However, if you patient is breathing much faster or slower, there is often cause for concern. Breathing too slowly could be that the patient might arrest. Breathing too quickly may indicate a stress response from the patient. 5. Arterial pressure readings are checked at the same time blood pressure readings are done. An arterial pressure should be no lower than –260. If the pressure is allowed to become greater ,there is a high chance of hemolyzing or crushing and destroying the Red Blood Cells. While your patient is on the machine, monitor the arterial pressure closely to prevent this from happening. - 15 - 6. Venous pressure readings are checked throughout the treatment. Increases of venous pressure over time may suggest problems with the access. 7. Access site observation is very important during hemodialysis. Monitoring for infiltration (will appear like swelling) or bleeding is important. If the site is infiltrated, the patient’s blood is not being routed properly. If not corrected, this will only get worse. If there is blood at the site, then the needle needs attention as this can cause many problems. One would be infection. This is typically a nursing responsibility. 8. Weight is also monitored before and after hemodialysis. Before the dialysis treatment the patient’s weight is usually elevated above their estimated dry weight (EDW). After a hemodialysis treatment and the fluid is removed the patient’s weight should be lower. The CNA-DT should know how to calculate the difference between their original weight and their goal weight and their pre- or post-weights. 9. Patient’s overall appearance. This would include his skin. Is it pale or purple, cold or warm? Are his nails purple, do they have any cuts or sores? Is there a rash? All of these need to be included in your observations and documentation. - 16 - How to take these measurements 1. Temperature To take a patient’s temperature, place the dotted or pointed end of the thermometer under the tongue. Close the mouth and hold the thermometer in place for 1 minute or till the device signals it is complete. Do not take a temperature immediately after drinking liquids or smoking a cigarette. At least 10 minutes should pass. Normal oral temperature is 98.6 degrees F (37 degrees C). The patient’s doctor or nurse practitioner should be notified if/when a patient’s temperature rises above 1000 (3). 2. Blood Pressure Your blood pressure is the force of blood pushing against artery walls as it flows through your body. Like air in a tire, blood fills arteries to a certain capacity. Just as too much air pressure can damage a tire, so can too much blood pressure damage healthy arteries. A blood pressure reading appears as two numbers. The first and higher of the two is a measure of systolic pressure, or the peak force of blood as it is actually being pumped by the heart. The second number measures diastolic pressure, or the force of blood when the heart is filling for the next beat. Normal blood pressure rises steadily from about 90/60 at birth to about 120/80 in a healthy adult. Anyone with a blood pressure of 140/90 on at least two occasions is said to have high blood pressure. If this continues the person may be placed on antihypertensives (2). The following standards for assessing high blood pressure (without regard to age) have been established by the National Institutes of Health JNCVI. Category Optimal Normal High Normal Hypertension Stage 1 Stage 2 Stage 3 Systolic (mmHg) <120 <130 130 - 139 Diastolic (mmHg) <80 <85 85 - 89 140 - 159 160 - 179 > 180 90 - 99 100 - 109 > 110 - 17 - Have the patient’s arm relaxed and supported so that the cuff is at the same level as the heart. The patient’s legs should not be crossed, and the patient should avoid talking while the pressure is being measured. The first measurement is a palpation at the wrist to estimate the systolic pressure. Since the average heart rate is 60 to 70 beats per minute, the mercury needs to fall about at least 70 points. That should take about 20 seconds to deflate the cuff until all sounds are gone. If this is done faster, it is not accurate. Consider the cuff size The usual size cuff is accurate for arms up to about 11 inches in circumference. If the cuff is too small, the pressure will be overestimated. Blood pressure changes significantly in response to several different things. It varies in a fairly regular manner during the daily cycle, lowest during sleep, and rising an hour or so before waking to its highest in mid-morning. Activities of daily living, work, exercise, and emotion further influence blood pressure, as do the seasons of the year. Consequently, an individual’s pressure may move from well below to far above 140 in the same day. Some patients only have an elevated pressure in the doctor’s office, so-called “white coat hypertension”. Most studies indicate that they do not require drug treatment (1). 3. Pulse Rate A pulse can be taken on any part of the body that a pulse can be felt. However, most pulse rates are obtained on the wrist or arm. To obtain a pulse, a gentle touch or pressure is applied over the area. Use the pads of your index and middle fingers to find the pulse on the patient’s wrist. Feel for the base of the thumb with your fingers. Move your fingers to just about an inch below the thumb base and press down lightly until you feel an intermittent "throbbing" sensation - that's the pulse. You can also take a pulse by placing a stethoscope over the patient’s heart and listening for the beat (left side of the upper portion of the chest). Once you've found your pulse, look at a clock or watch with a second hand and count the number of beats for a period of 15 seconds. Multiply the number of beats by 4 to find out your "heartbeats per minute (4)." - 18 - 4. Respiratory Rate To obtain a respiratory rate, you need to watch and count as the patient breathes. Simply count the number of times the patient’s chest rises and falls and multiply the number by 4. This is the respiratory rate for one minute. Keep in mind that most people will breathe differently when they know someone is watching. Try to not allow the patient to know you are counting their breaths. Many health-care professionals will hold a patient’s wrist when counting breaths as if they were taking a pulse. This may help to defocus the patient. 5. Arterial Pressure This is the pressure used to pull the blood from the patient’s access. Ideally you’ll want to use as little pressure as possible to pull the blood. Too much pressure can damage the red blood cells and ultimately destroy them, hemolyzed them. Therefore, the arterial pressure during a hemodialysis treatment should be kept –260 or less. How is that done? Causes of Lower Arterial Pressure Separation of blood tubing from the arterial access Stop the blood pump Clamp bloodline and access line Alert the nurse Evaluate patient blood loss Restart dialysis if ordered Inadvertently opened saline administration line Clamp saline administration line Alert the nurse Adjust UFR to remove the additional fluid Opening in the arterial blood tubing that allows air to enter Locate and eliminate source of air entrance Remove air from the system by withdrawing using a syringe Decrease in blood pump speed - 19 - Restore blood pump rate to prescribed setting Causes of Increased Negative Arterial Pressure Blood flow problems Arterial needle infiltrated Arterial needle is clotted Arterial needle is poorly positioned Kinking of the arterial blood tubing Hypotension 6. Stop the blood pump. Re-establish arterial blood flo Resume Rx blood flow rate Alert nurse to problem Straighten blood tubing Verify hypotension by obtaining a blood pressure Treat hypotension per protocols Venous pressure is also monitored. Potential concerns are: Causes of Lowering Venous Pressure Separation of blood tubing from the arterial access The venous blood tubing is kinked. Straighten blood tubing Clotting of the dialyzer Evaluate extent of clotting Replace dialyzer Resume dialysis Decrease in blood pump speed Verify that the blood pump rate is at the Rx rate Stop the blood pump Clamp bloodline Alert the nurse Evaluate patient blood loss Restart dialysis if ordered Causes of Increased Venous Pressure Kinking of the venous blood tubing between the monitor and the patient Blood flow problems Arterial needle infiltrated Arterial needle is clotted Arterial needle is poorly positioned Increase in blood pump speed Straighten the blood tubing Stop the blood pump Restore venous blood flow Resume Rx blood flow rate Verify that the blood pump rate is at the prescribed setting - 20 -