Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
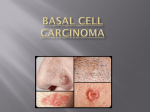
Residents Day Academy 2012 Phoenix: Case Report Clinical Findings and Management of Basal Cell Carcinoma The Importance of Addressing the Patient’s Chief Complaint Treat the Patient, Not the Disease Amy Slama 225 Cleveland Ave. W. Winnebago, MN 56098 507-382-1331 [email protected] Abstract Basal cell carcinoma (BCC) is a malignancy of the basal cell layer of the epidermis. It most commonly presents as a shiny, firm pearly nodule with superficial telangiectasia. Progression of the BCC lesion can result in a rodent ulcer (central ulceration), which can be induced by a number of environmental and genetic factors1. Most eyelid malignancies rarely metastasize, but they can be locally destructive. This case report reviews the importance of assessment and treatment of a patient’s presenting chief complaint. Remarkable sight threatening findings cannot result in the overlooking of a patient’s chief complaint. It also stresses the importance of clinicians to accept and appreciate a patients right to decline recommendation and referral. The case reviews clinical findings, the course of a disease, and the weighing of treatment options for a patient under hospice care. This case report reviews the management of a patient with BCC, primary open angle glaucoma, dry eye syndrome, and an epi-retinal membrane through discussion of clinical findings and treatment options as they relate to the case presented. Key words: Basal Cell Carcinoma (BCC), metastasize, biopsy Page 1 of 8 Introduction Basal Cell Carcinoma is the most common skin cancer in humans, yet it results in only 0.1% of patient deaths due to cancer 2. It is a malignant tumor that affects the cells of the basal layer of the epidermis, frequently of the eyelid margins resulting in 85-90% of all eyelid malignancies 3. It typically presents on sun-exposed skin, rarely metastasizes (0.028-0.55%), and is slow growing2. The epidemiology of BCC is more common in males, whites, light skinned individuals, and people between the ages of 40 and 79 years of age 3. BCC can present in a nodular form: shiny, firm, pearly nodule with blood vessels that easily bleed. If not recognized or treated at an early stage, progression occurs and central ulceration can develop (rodent ulcer) 4. Basal cell carcinoma has been associated with ultraviolet exposure, ionizing radiation, arsenic exposure, and scars. Diagnosis of BCC can be made initially from its clinical appearance, but definitive diagnosis is through biopsy. Treatment can result in 5-FU, surgery, radiation therapy, cryotherapy, chemotherapy, and photodynamic therapy1,4. The etiology of BCC remains obscure, but genetic and environmental factors are proven to predispose patients to BCC. Recent studies are showing that the pathophysiology of BCC results in signaling pathways, specifically the patched/hedgehog intracellular signaling pathway. There is known relationship between BCC and pilosebaceous unit because tumors are often observed in hair-bearing areas. Radiation, immunologic origins, and DNA mismatch repair proteins are also proven to be causative factors for BCC 2. Case Report Date: 5/25/11 Clinic Location: BVA, Tulsa, Oklahoma Case Report: Patient #1 Age: 59 Sex: M Race: Middle Eastern Subjective Patient #1 is a 59-year-old Middle Eastern male that presented to BVA Advanced Eye Care on May 25, 2011 for a consult on his left eye with a chief complaint of decreased vision for the past several months that ranges from six months to a year. Patient #1 feels the decreased vision is moderate. He reports that he has no pain or discomfort out of the left eye and sees better some days more than others. He was presently taking 0.004% Travatan (2.5ml bottle) two times a day with no other associated symptoms. Patient #1 states that his right eye had progressively lost vision since he was diagnosed with basal cell carcinoma of his superior right eyelid twenty years ago. He has never received treatment or had surgery to address the basal cell carcinoma. Patient #1 presented to BVA Advanced Eye Care with bandages and gauzes covering his head and right eye (see attached photo). He states Page 2 of 8 he has no pain in the right eye, and the bandages are applied for cosmetic purposes. The patient states, “the right eye is just dead, it just went bad.” Patient #1 is currently living in a nursing home under hospice care. He was currently on a list several systemic medications, which he was unable to report specific names. The nursing home was going to be contacted for a fax of his medication list. The patient was on an ocular drop, 0.004% Travatan (2.5ml bottle). In the past he was put on Travatan, due to increased pressures. He is not on any other ocular medications or drops. Patient #1 has no known drug allergies or seasonal allergies. He has an ocular history of blurred distance vision, eye infections, and loss of vision. His medical history consists of skin cancer to the face, convulsions, constipation, altered mental status, hypertension, anemia, and esophageal reflux, with unremarkable family medical and ocular history. Patient’s social history was that he wanted to keep the remaining vision he has in his right eye so he’s able to watch the T.V. He is currently under hospice care in a local nursing home. Objective During the examination, patient #1 was fully conscious, alert, oriented in time and space, however, he did get upset and appeared stressed when we wanted to discuss his right eye. Patient #1 states, “stop worrying about his right eye and focus on the left eye’s vision.” Upon presentation, testing and measurements of his right eye were not applicable due to the bandages. Vision unaided was measured to be count fingers out of the left eye. Extra-ocular motilities were full range of motion, with no pain or diplopia, and there was poor cooperation due to fixation losses on confrontation visual fields. Intraocular pressure using one drop of 0.5% proparacaine hydrochloride ophthalmic solution through goldmann applanation measured 32mmHg. Pupillary reaction was present in the left eye, measuring five millimeters in diameter in dim illumination to a size of four millimeters under bright illumination. Bandages were pulled back to observe the right eye. Observation of basal cell carcinoma damage was noted to include and affecting the right side of the face, eye socket, forehead, right globe, right side of skull, and all surrounding tissue. Tissue and bone necrosis was observed with exposed meninges, and ocular globe. A visible optic nerve with a swollen and clouded over right eyeball was observed. The depth and extent of tissue and bone necrosis were not observable due to patient’s lack of cooperation in removal of bandages. Patient #1 reported that he was diagnosed with BCC of the upper eyelid twenty years ago and chose not to treat. He did not vocalize reasoning’s for not pursing treatment but he did say that he has been evaluated and educated on treatment and management options for his cancer. Page 3 of 8 Anterior segment evaluation using slit lamp biomicroscope of patient #1’s left eye revealed dermatochalasis of the superior lid margin with eyelid ptosis and brow ptosis. Bulbar and palpebral conjunctiva presented as clear. His cornea revealed 1+ diffuse superficial punctate keratitis. The patient’s anterior chamber was deep and quiet, with the iris being round and reactive to light. Lenticular evaluation revealed a clear, well centered posterior intraocular lens, and present vitreous syneresis of the left eye. Anterior segment evaluation through slit lamp biomicroscope was not attempted. Upon presentation of dilated fundus examination using one drop of 1% tropicamide ophthalmic solution and one drop 2.5% phenylephrine hydrochloride ophthalmic solution, a cup-to-disk ratio of 0.6 round with paleness temporally was revealed. The macula was positive for an epi-retinal membrane and negative for macular pucker. The retinal vessels exhibited 1+ attenuation and an increase in arterial light reflex of one-half. The periphery of the fundus was flat with no holes, tears, or detachments of the left eye. Page 4 of 8 Assessment 1. Dry Eye Syndrome, left eye 2. Primary Open Angle Glaucoma, left eye 3. Epi-retinal Membrane, left eye 4. Basal Cell Carcinoma, right eye, right side of the face, and right forehead a. Metastasis and necrosis of the lids, globe, orbits, and meninges Plan 1. Patient Educated was done concerning the examination findings. 10mL/0.3 fl oz/30 sterile Oasis Plus nonpreservative artificial tears were prescribed with instructions to place one drop in the left eye every two hours daily. Monitor in two weeks for an improvement in superficial punctate keratitis and a reduction in irritating symptoms. 2. Discontinue use of Travatan. Rx/Prescribed 0.5% Combigan ophthalmic solution with instructions to place one drop two times a day in the left eye. Monitor in two weeks with an intra-ocular pressure check or sooner should there be an increase in pain, decreased or blurry vision, or redness. Order an optic nerve head OCT scan at two week follow up for review glaucomatous damage. 3. Monitor Epi-retinal membrane for progression. No signs of edema. Perform a macular OCT scan at two week follow up to confirm epi-retinal membrane and rule out any macular traction or pucker. 4. Explained and educated to the patient the significance of basal cell carcinoma. Educated and recommended patient referral to specialist for possible enucleation, skin graft, treatment, and plastic surgery. Patient clearly declined a referral to specialist for evaluation of his right eye. Documented that patient clearly declined referral and was in a sane state of mind. Return to Clinic: two weeks or PRN Reason for referral: Biopsy, treatment options, cosmetic concerns all on our recommendations not the patient concern Expected outcomes: Biopsy, enucleation of the eyeball, skin graft over the exposed area, no treatment The differential diagnosis considered in this case include: Patient confirmed basal cell carcinoma diagnosis, however, differentials of BCC include: squamous cell carcinoma, actinic keratosis, radiation dermatitis, Page 5 of 8 keratancanthoma, amelanotic melanoma, glomus tumor, lymphoma, malignant melanoma, metastatic oat cell carcinoma, sebaceous cell carcinoma, Follow Up Patient #1 returned to BVA Advanced Eye Care on 6/8/11 for a follow up visit concerning his visual acuities and eye comfort from his dry eye syndrome after using one drop of 10mL/0.3 fl oz/30 sterile Oasis Plus non-preservative artificial tears every two hours for two weeks in his left eye. He reported adequate compliance and improved symptoms using10mL/0.3 fl oz/30 sterile Oasis Plus non-preservative artificial tears. His visual acuities tested at five feet measured count fingers. This patient’s intra-ocular pressure in his left eye was also checked using one drop of 0.5% proparacaine hydrochloride ophthalmic solution through goldmann applanation to see how one drop 0.5% Combigan twice a day in the left eye is working. His measured pressure was 16mmHg; a 16mmHg decrease of pressure in the left eye using one drop 0.5% Combigan twice a day. Anterior segment evaluation using slit lamp biomicroscope of patient #1’s left eye revealed similar findings with resolved superficial punctate keratitis. Observations of the fundus through undilated ninety indicated a new splinter hemorrhage near the optic nerve head. There was continued patient education explaining his decreased vision was due to primary open angle glaucoma and the presence of an epi-retinal membrane of the macula of the left eye. An OCT of the macula and optic nerve head was ordered, read, and reviewed with the patient, verifying the epi-retinal membrane of the macula. The OCT of patient #1’s optic nerve head showed significant decrease in RNFL thinning in the superior and inferior quadrants with an increased C/D ratio of 7.9. He was scheduled for a three-month intra-ocular pressure check. Recommend continued use of 10mL/0.3 fl oz/30 sterile Oasis Plus non-preservative artificial tears four times a day in his left eye until three-month exam for dry eye syndrome. Continue using one drop 0.5% Combigan twice a day in the left eye. Monitor epi-retinal membrane and basal cell carcinoma of the right side of the face, forehead, orbit, eye socket for any progression at three-month exam. Discussion Rarely does basal cell carcinoma spread or metastasize, let alone cause death. However, with patient #1 it has metastasized and will unfortunately take his life. This is a great case to educate doctors and patients of how skin cancer can result if left untreated. It can grow to surrounding areas and nearby tissue and bone. Page 6 of 8 BCC is a slow-growing form of skin cancer. This patient reported that he was first diagnosed twenty years ago. It is hard to believe someone would not want to treat the skin cancer especially since it has a high success rate in removal, a low recurrence rate, and low rate of metastasis. The pathogenesis of basal cell carcinoma results from ultraviolet light exposure, fair skinned individuals, and blue and green-eyed individuals. The invasion of the tumor is proposed to result from an enhancement of the tumor cell motility and collagenase content2. It can present as a sore that won’t heal, bleeding nodule, or a sunken ulcer. As an optometrist it is important to report on the size, shape, color, and texture of any suspicious lesion. BCC can be classified as nodular-ulcrative, pigmented, morphea or sclerosing, superifical, linear basal cell nevus, follicular basal cell nevus, or fibroepithelioma2,3. Differentials of BCC include: actinic keratosis, squamous cell carcinoma, malignant melanoma, nevi, molluscum conagiosum2,3. Patient #1’s site of origin was on his superior lid that started out as a nodule the progressed to an ulcerative nodule. It continued to spread and necrose the skin, eyelid, bone, muscle, etc… resulting in the picture above. BCC’s ocular manifestations effect the upper lid 50-60% of the time with the lower lid of 25-30% prevalence3. A skin biopsy is required to confirm the diagnosis of BCC. Cytology is and can also be done with distinctions in histological findings of specific BCC types. Treatment options for BCC include: surgical excision, radiation therapy, curettage, electrodesiccation, cryotherapy, all non-Mohs modalities, and Moh’s micrographic surgery3. These different approaches depend on the extent of progression. Other treatment and management options consist of topical 5-fluorouracil 5%, interferon, imiquimod, tazarotene, GDC-0449, radiation therapy, photodynamic therapy, and systemic retinoids2. With this case presentation recommendation of enucleation of the eyeball, surgical excision of the affected tissue, and a skin graft were discussed with Dr. Jason Ellen. Although early BCC can be treated adequately with local excision, patient #1’s advanced case would be best managed by a multidisciplinary approach involving head and neck surgical oncologists, Mohs micrographic surgeons, reconstructive plastic surgeons, pathologists, prosthetics, and radiation oncologist. Due to the patient’s prerogative and desire not to treat we documented thoroughly in the chart; refusal of referral and respected his wishes. Focus was directed toward his primary open angle glaucoma of the left eye and persevering his remaining sight. This man made me think about how important it is to treat the patient, not the disease! Page 7 of 8 Once diagnosed and treated, BCC can reoccur; recurrence rate averages around 5%2. Patients need to be educated on prevention, recurrence, and how it BCC can spread. The use of hats, sunglasses, sunscreen, etc… can help prevent and reduce the risk of BCC. Self-examinations are recommended and suspicious lesions should be addressed1,4. Conclusion It is important for clinicians to not only observe the eye, but also be aware of the surrounding tissues. Examine the lumps, bumps, nodules, scabs, and freckles in more detail so any malignancies are caught at an early stage. This will help avoid potential complications in the future. Although the prognosis for patients with BCC is favorable, you can see from this case report that it can result in greater destruction and metastasis affecting the patient’s overall health. This case demonstrates the role of a patient’s chief complaint, along with their wishes in not following recommendations and referrals for treatment. It stresses the importance of saving the remaining sight and making the patient comfortable through compassion and respect of his prerogative. The initial instinct is to address the right eye, but due to this patient’s systemic health and wishes, BVA is continuing to work with patient #1 to preserve the remaining sight of his left eye. It was a pleasure to work with this patient and I hope he has stable vision in his left eye for years to come. Bibliography 1. Ehlers JP, Shah CP. 2008. The Wills Eye Manual. Philadelphia, PA: Lippincott Williams & Wilkins. 2. “Basal Cell Carcinoma.” Medscape Reference. Web. 15 January. 2012. <http://emedicine.medscape.com/article/276624-overview.>. 3. Yanoff, Myron, Duker, Jay S. Ophthalmology, 2nd Ed. London Mosby International Ltd. 2004. 4. Friedman, N, Kaiser, P. The Massachusetts Eye and Ear Infirmary, 3rd ed. Elsevier, 2009. Page 8 of 8