Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
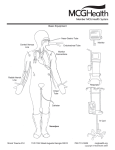
St. Luke’s College of Medicine-William H. Quasha Memorial Batch 2012 ER Block III Lecture Trans Common Emergency Department Procedures Gloria, MD 22 September 2009 Emergency Medicine Procedures for Clerks Intravenous Cannulation Urinary Catheterization Nasogastric Intubation Bag-Valve Mask Ventilations Intravenous Cannulation Indications Access to venous circulation Administer blood products, fluids or drugs Obtain samples of blood for laboratory evaluation Preparation: Apply universal precautions (BSI on!) Catheter gauge depends on clinical scenario o G22 – routine maintenance fluids (ateneo blue) o G18 or G20 – blood product administration (la salle green) o G16 – suggested for resuscitation (pink) Site Selection Depends on: Intended use of the catheter Accessibility of the vein given the position of the patient Patient’s age & comfort (esp px’s handedness) Urgency of the situation Best starting place is the hand (most accessible). In s/p MRM patients, AVOID arm on the same side Circulation may be impaired You want to avoid the arm of the same side for the simple reason that in MRM there is dissection of the lymph nodes. Possibleng natamaan ‘yung mga blood vessels. You are unsure of the drainage of that area. Your circulation might be impaired. Equipment Needed Gloves Eye Protection Non-latex Tourniquet Antiseptic Solution Sterile Gauze Saline Flush Tape Transparent Occlusive dressing Catheter of appropriate size IV Fluid bag with tubing Sharps container Topical Anesthetic Procedure: 1. Insert spiked end of IV tubing into IV bag 2. Pinch drip chamber to fill bulb halfway before infusing fluid Krista & Doms Steps 1 and 2 3. Flush IV tubing 4. Flush saline lock 5. Apply tourniquet 3-4 cm proximal to the insertion site 6. Cross tourniquet ends & apply tension 7. Tuck middle portion or one end snugly under opposite end to make a loop 8. Distal portion of tucked end is left free for one-hand release of tourniquet 9. Prep the insertion site with alcohol 10. Grasp skin & pull taut to apply traction 11. Take catheter between thumb & forefinger in dominant hand Bevel up, Angled 5-30°, aligned parallel to the vein 12. Puncture vein 13. Once flash is seen, advance catheter several mm more to ensure it has entered the vein & not just the wall 14. Occlude vein using the fingers anchoring the vein at the tip of the catheter 15. Remove needle & connect Syringe for phlebotomy Saline lock/IV line ER: Common Emergency Department Procedures page 1 of 6 St. Luke’s College of Medicine-William H. Quasha Memorial Batch 2012 16. Release the tourniquet 17. Anchor the device Use adhesive tape (1/2 in dia), adhesive up under the hub of the catheter Fold it over like a bow 18. Clear polyurethane dressing can be used with or instead of tape 19. Secure loose saline lock or IV tubing with tape to prevent accidental dislodgement 20. Sign & date dressing to assure timely changes Complications Pain Bruising Bacterial Infection Phlebitis Extravasation Thrombosis Nerve Injury Air embolism CDC Recommendations for IV Care: Record and date the time of the catheter insertion in an obvious location near the insertion site Do NOT palpate insertion site after skin has been cleansed with antiseptic Palpate insertion site for tenderness daily through an intact dressing Visually inspect the site if the patient reports tenderness Wash hands before and after palpating, inserting, replacing or dressing any intravascular access site Replace dressing when they are damp, loose, or soiled Urethral Catheterization Indications Bladder drainage in urinary retention Instill local intravesical therapy or irrigation to remove clots from urinary bladder Obtain sterile urine samples Instill contrast media for imaging procedures Measuring residual volumes after voiding Urine output monitoring in any critically ill or injured patient Absolute Contraindication Trauma patient with suspected urethral injury o Blood at urethral meatus o Abnormal-feeling or high-riding prostate on rectal examination o Penile, scrotal or perineal hematoma Equipment: Povidone iodine Sterile cotton balls Water-soluble lubrication gel Sterile drapes Sterile gloves Krista & Doms Lecture Trans Urethral catheter Prefilled 10-mL saline syringe Urinometer connected to a collection bag Female Urethra Short (≈4cm) straight tube Wide caliber Lying on top of the vagina Occasionally hidden Male Urethra Approximately 20 cm long o From external meatus to the bladder neck Posterior prostatic urethra is approximately 3.5 cm long Procedure: Females Non-dominant thumb & index finger are used to separate the labia & expose the urethral meatus Urethra is approached between the double labia Clean exposed meatus with antiseptic solution Lubricate catheter Slowly & gently pass the catheter Only half the total length of the catheter has to be inserted before it is safe to inflate the balloon Slowly withdraw catheter until approximation of the bladder neck precludes further withdrawal Secure the catheter using tape Procedure: Males Foreskin should be retracted to its fullest extent proximal to the glans penis Establish sterile field Secure penis between the long & ring fingers of the non-dominant hand The non-dominant index finger & thumb will then manipulate the catheter Procedure: Males The penis should be held taut & upright o Downward traction kinks the penis & promotes urethral folding at the level of the penile suspensory ligament Catheter must be fully inserted to the ballooninflating side arm before it is safe to inflate the balloon Nasogastric Intubation Indications Decompression of the gastrointestinal tract o Small bowel obstruction o Gastric emptying in intubated pxs to prevent aspiration Administration of oral agents o activated charcoal, oral radioactive contrast media Gastrointestinal hemorrhage Contraindications Maxillofacial trauma ER: Common Emergency Department Procedures page 2 of 6 St. Luke’s College of Medicine-William H. Quasha Memorial Batch 2012 Esophageal abnormalities -eg strictures, diverticula perforation Altered mental status and impaired airway defenses Equipment Nasogastric tube o Adult - 16-18F o Pediatric - In pediatric patients, the correct tube size varies with the patient’s age. To find the correct size, add 16 to the patient’s age in years and then divide by 2 (eg, [8 y + 16]/2 = 12F) Viscous lidocaine 2% Oral analgesic spray (Benzocaine spray or other) Oral syringe, 12 mL Glass of water with a straw Water-based lubricant Toomey syringe, 60 mL Tape Emesis basin or plastic bag Wall suction, set to low intermittent suction Suction tubing and container Procedure 1. Position the patient seated upright. 2. Examine the patient’s nostril for septal deviation. To determine which nostril is more patent, ask the patient to occlude each nostril and breathe through the other. 3. Instill 10 mL of viscous lidocaine 2% (for oral use) down the more patent nostril with the head tilted backwards, and ask the patient to sniff and swallow to anesthetize the nasal and oropharyngeal mucosa. In pediatric patients, do not exceed 4 mg/kg of lidocaine. Wait 5-10 minutes to ensure adequate anesthetic effect. 4. Estimate the length of insertion by measuring the distance from the tip of the nose, around the ear, and down to just below the left costal margin Lecture Trans 8. At this time, ask the patient to sip on the water through the straw and start to swallow 9. Continue to advance the nasogastric tube until the distance of the previously estimated length is reached. 10. Verify proper placement of the nasogastric tube by auscultating a rush of air over the stomach using the 60 mL Toomey syringe or by aspirating gastric content 11. Ideally, obtain a chest radiograph in order to verify correct placement, especially if the nasogastric tube is to be used for medication or food administration 12. Tape the nasogastric tube to the nose to secure it in place. If clinically indicated, attach the nasogastric tube to wall suction after verification of correct placement Complications Patient discomfort o Generous lubrication, the use of topical anesthetic, and a gentle technique may reduce the patient’s level of discomfort o Throat irritation may be reduced with administration of anesthetic lozenges (eg, benzocaine lozenges [Cepacol]) prior to the procedure Epistaxis o May be prevented by generously lubricating the tube tip and using a gentle technique Respiratory tree intubation Esophageal perforation Bag-Valve Mask Ventilation Indications Respiratory failure (but breathing) Complete apnea General anesthesia, neuromuscular blocking agents, narcotic overdose, cerebrovascular accidents, cardiopulmonary resuscitation Other situations in wc spontaneous breathing fails Contraindications RARELY contraindicated Caution is advised in: o Severe facial trauma o Eye injuries 5. Position the patient sitting upright with the neck partially flexed 6. Lubricate the distal tip of the nasogastric tube 7. Gently insert the nasogastric tube along the floor of the nose and advance it parallel to the nasal floor (ie, directly perpendicular to the patient's head, not angled up into the nose) until it reaches the back of the nasopharynx, where resistance will be met (1020 cm) Krista & Doms Equipment Face mask Bag-valve Suction Oxygen Rescue Breathing Using Bag Mask: Single Rescuer Position yourself directly above the patient’s head Place mask on victim’s face, using bridge of nose as guide for correct position E-C Clamp Technique ER: Common Emergency Department Procedures page 3 of 6 St. Luke’s College of Medicine-William H. Quasha Memorial Batch 2012 Lecture Trans Use thumb & index finger of one hand to make a “C”, pressing edges of mask to the face NPA insertion Remaining 3 fingers form an “E” E-C Clamp Technique Remaining fingers (forming an “E”) lift angles of the jaw & open airway Squeeze bag to give breaths (1 sec each) Rescue Breathing Using Bag Mask: Two Rescuers Provides more effective ventilation 1 rescuer opens airway with head tilt & jaw lift & opens mask to the face 2nd rescuer squeezes the bag 1. 2. 3. 4. Oropharyngeal Airway If patient is unconscious & has no gag reflex, oral airway may be used Cricoid Pressure (Sellick Maneuver) May be applied if 3rd rescuer is present Done ONLY in the unconscious patient Minimizes gastric inflation OPA Insertion 1. Sellick Maneuver: 1. Locate thyroid cartilage with the index finger 2. Move down neck to first cartilage ring (cricoid cartilage) 3. Apply modest pressure (5-10 lbs) using thumb & index finger 4. Nasopharyngeal Airway 5. Nasopharyngeal airway may initially establish & maintain airway patency in the conscious patient Krista & Doms 2. ER: Common Emergency Department Procedures page 4 of 6 St. Luke’s College of Medicine-William H. Quasha Memorial Batch 2012 Lecture Trans 3. Alternative Methods: OPA procedure Insert the airway sideways and rotate it 90O Oral Pharyngeal Airway Definitive airway should be established if there is any doubt about the patient’s ability to maintain integrity Advantages of tracheal intubations: Airway patency Protects the airway Maintains patency during positioning Insertion of OPA using a tongue depressor Complications Corneal abrasions and blindness in the presence of eye injury Soft-tissue injuries, including injuries to the nose and lips, may result when excessive pressure is applied Airway Procedures A. Nasopharyngeal Airway Control of ventilation Ventilation over a long period of time without intubation can lead to gastric distention and regurgitation Advantages of tracheal intubations: Route for inhalation anesthesia and emergency medications : N – Narcan A – Atropine V – Valium E – Epinephrine L – Lidocaine Complications of tracheal intubation: Trauma to the lips, teeth, and soft tissues of the airway. Awareness Meticulous technique Bronchial intubation Frequent complication Auscultation of the chest bilaterally Airway If patient is unconscious & has no gag reflex, oral airway may be used Complications of tracheal intubations: Laryngospasm o common when extubation is done when the patient is in a semiconscious state o extubation should be done in a relatively deep anesthesia or when the protective laryngeal reflex has returned Post-intubation hoarseness and sore throat o Due to mechanical presence of the tracheal tube Oral Pharyngeal Airway Measure Confirm patient is unconscious Insert, rotate 180 degrees as inserting Preparation of Equipment Assemble pharyngeal airways in assorted sizes Inspect laryngoscope for serviceability o Batteries 1. 2. 3. 4. 5. Lubricate ! Insert along floor of nasal cavity If resistance met, use back-and forth motion Don’t Force – Use other nostril If patient gags, withdraw slightly Krista & Doms ER: Common Emergency Department Procedures page 5 of 6 St. Luke’s College of Medicine-William H. Quasha Memorial Batch 2012 o Light bulb o Blades; curved/straight (Macintosh or Miller) Selection of laryngoscope blade (preference) Macintosh is a curved blade whose tip is inserted into the vallecula (the space between the base of the tongue and the pharyngeal surface of the epiglottis). Selection of laryngoscope blade (preference) Miller is a straight blade that is passed so that the tip of the blade lies beneath the laryngeal surface of the epiglottis o The epiglottis is then lifted to expose the vocal cords Tube size o adult male 8 mm to 9 mm tube o adult female 7 mm to 8 mm tube Preparation of Equipment -Inspect endotracheal tubes Tube length – extend from the lower incisor to a point midway between the cricoid cartilage and Louis's angle (the sternal angle) on the patient Endotracheal tube cuff Malleable stylet (should not extend past Murphy's eye) Lubrication Laryngeal sprays Inspect resuscitator (AMBU bag) for serviceability Bag Mask Intake valve Valve body with relief valve Intubation Technique Ventilate with 100 percent oxygen for approximately 1 min Position bed height to bring the patient's head to a mid-abdominal height Flex the cervical spine and extend the head at the atlanto-occipital joint Long axis of the oral cavity, pharynx, and trachea lie almost in a straight line Introduce the blade into the right side of the patient's mouth Move the blade posteriorly and toward the midline, sweeping the tongue to the left and keeping it away from the visual path with the flange of the blade Ensure the lower lip is not being pinched by the lower incisors and laryngoscope blade Advance the laryngoscope until the epiglottis is in view Lift the laryngoscope upward and forward Insert the endotracheal tube from the right with its concave curve facing downward and to the right side of the patient Maneuver the endotracheal tube into the larynx, midway between the cricoid cartilage and the sternal angle Krista & Doms Lecture Trans Inflate the cuff and apply positive pressure ventilation while the assistant auscultates Secure the endotracheal tube in position Confirmation of tracheal intubation: Direct visualization of the ET tube passing through the vocal cords CO2 in exhaled gases Confirmation of tracheal intubation: Bilateral breath sounds Absence of air movement during epigastric auscultation Confirmation of tracheal intubation: Others Condensation (fogging) of water vapor in the tube on exhalation Refilling of reservoir bag during exhalation Maintenance of arterial oxygenation Chest X-ray: the tip of the ET tube should be between the carina and thoracic arc or approximately at the level of the aortic arch Additional notes: (recall lang. alam nyo na ‘to.) CPR with Advanced Airway Compression rate is about 100 bpm 1 breath every 6-8 sec Avoid hyperventilation Do no pause compressions to provide breaths If the adult patient is not intubated, you would want to give him how many breaths? 10 to 12 breaths per minute. Pag pedia, ilan? How many per minute? 12 to 20. ER: Common Emergency Department Procedures page 6 of 6