Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
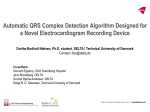
TCA OVERDOSE DANGEROUS DRUGS Tricyclics Amitriptyline Desipramine Imipramine Nortriptyline Doxepin Clomipramine Tetracyclics Mirtazapine Mianserin Trazodone Amoxapine Setiptiline Maprotiline PHARMACOLOGIC CONSIDERATIONS “Dirty Drugs” Block many receptors Serotonin/NA reuptake H1&H2 – sedation Alpha1&2 – hypotension GABA-A – seizures Muscarinic – anticholoinergic Na+ channels – arrhythmias (class Ia) K+ channels Rapid incomplete absorption (decreased by anti-Ach effect – decr gastric emptying& SR preparations) LARGE Vd: Plasma conc incr rapidly – affects heart/brain quickly (before it’s redistributed to fat) PROTEIN BINDING: 10% free, 90% bound Binding decreased by ACIDOSIS, increased by ALKALOSIS (Important in treatment) Increased FREE drug = greater effects, ie ALKALOSIS = LESS FREE DRUG = LESS EFFECT METABOLISM T1/2 Prolonged by: Hepatic metab (overwhelmed in OD) Enterohepatic circulation Active metabolites Minimal renal excretion SYMPTOMS/TOXIDROME “TRI”-cyclics = 3 MAIN EFFECTS 1) CNS 2) ANTICHOLOINERGIC 3) CARDIOVASCULAR 1) CNS Sedation – coma (can be rapid & precede CVS signs) Seizures – treat as per normal 2)ANTICHOLINERGIC (opposite of DUMBELS) Mydriasis (dilated pupils) Dry mouth/skin Tachycardia Urine retention Ileus Delirium 3) CARDIOVASCULAR a) ECG Can’t rule in or rule out TCA OD “Suggestive” changes Can have SERIOUS OD WITH NORMAL ECG a) STRONGLY SUGGESTIVE of TCA OD i) aVR: terminal 40msec >3mm ii) Deep S in I and aVL b) PREDICTORS i) QRS > 100msec = PREDICTS “Serious Toxicity” - RISK: Seizures Arrhythmias Hypotension Coma/Intubation ii) QRS > 160msec = PREDICTS VT - No VT with QRS < 160msec b)HYPOTENSION i) direct myocardial depression ii) vasodilation (alpha block) Treat with fluid INOTROPES OK AS LONG AS ADEQUATE BICARB GIVEN 4) OTHER: Pulmonary – APO/ARDS (direct effect on pulmonary vessels) Hyperthermia Rhabdomyolysis COMPLICATIONS ACIDOSIS – mixed metabolic & resp Respiratory depression – Incr CO2 Metabolic – seizures BAD BECAUSE: 1) pKa 8.5 pKa – pH = (protonated/unprotonated) RNH3+ <==> RNH2 + H+ Protonated Unprotonated Ionised Non-ionised <----- Acidic pH Alkaline pH ------> ACIDOSIS Bad because acidosis encourages drug to be in IONISED/PROTONATED FORM Alkalinisation pushes pH closer to pKa = more drug in non-ionised form NON-IONISED DRUG Less affinity for Na+ channels Increased lipid solubility = redistributes to fat 2) ACIDOSIS – increases FREE drug Alkalinisation – increases protein binding SPECIFIC INVESTIGATIONS/LEVELS TCA Levels do not correlate with severity DECONTAMINATION Activated charcoal if < 1hr ANTIDOTE = BICARBONATE INDICATIONS FOR NaHCO3i) ACIDAEMIC: pH < 7.35 ii) QRS > 100msec iii) aVR R wave > 3mm iv) WIDE COMPLEX TACHYCARDIA ABNORMAL ECG (as above) Defib unlikely to work 2nd line: lignocaine 1.5mg/kg (once pH >7.5) CPR: may need PROLONGED CPR (hours) ALSO: Intubate & HYPERVENTILATE NB: Ia drugs Contraindicated (Amiodarone/B-blockers/Procainamide) Hypotension Crystalloid Bicarb Inotropes: NA/Adr infusion OK as long as “adequate bicarb given” (ie pH > 7.50) Seizures/coma Not clearly an indication for HCO3Usually treat as for normal seizure (BZD’s) Dose: 2 mEq/kg IV Repeat every 1-2 mins until restoration of perfusing rhythm Or pH > 7.5 Once pH > 7.5 can try Lignocaine if still in VT SPECIFIC TREATMENT ALKALINISATION 1) HCO32) Hyperventilate Aim for pH 7.50-7.55 pCO2 30mmHg SEIZURES: TREAT WITH BENZODIAZEPINES DIALYSIS HELPFUL? No – Large Vd NB CARDIAC ARREST: = INDICATION FOR PROLONGED CPR INTUBATE & HYPERVENTILATE BICARB To pH > 7.50 GOOD OUTCOME IS POSSIBLE WITH THESE MEASURES TAKE HOME POINTS: Normal ECG does not exclude serious toxicity DON’T GIVE AMIODARONE/B-BLOCKERS TO WIDE COMPLEX TACHY IF TCA OD SUSPECTED