Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
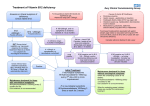
PREVALENCE OF VITAMIN B12 DEFICIENCY AND ITS IMPLICATION IN INDIA ABSTRACT: Vitamin B12 is important for our body to work properly. It plays a crucial role for the normal functioning of brain, nervous system and formation of blood. A person who lacks vitamin B12 may feel tired, lack of energy, fatigue and may suffer from lack of appetite, depression, difficulty in maintaining balance, confusion, poor memory, dementia and soreness of the mouth or tongue. In India the most common cause of vitamin B12 deficiency is vegetarian diet since it is only obtained from animal food. In India, very little appreciation is been given to vitamin B12 deficiency among the Indian medical professionals and policy makers. This may be due to various reasons: 1) it is not routinely measured in clinical practice, 2) despite of low level of circulating vitamin B12, signs for specific neurological or haematological syndrome consistent with vitamin B12 deficiency are rare, 3) the reports of prevalence, majority of them are based on clinical data and, therefore, may not represent community prevalence. This article points out the reason of vitamin B12 deficiency and the population at risk and how to diagnose them and provide proper treatment. INTRODUCTION Vitamin B12 is a water soluble vitamin and it is naturally present in some foods, also available as dietary supplement and as prescription medication.[26; 1-4] It is also known as cobalamin and is important for the body to work properly. It is a cobalt containing compounds which are a biologically active corrinoid with macrocyclic pyrrol rings [2; 3]. Vitamin B12 plays an important role in normal functioning of the brain, nervous system and for the formation of blood [31; 1]. People who are deficient of vitamin B12 may feel tired or have lack of energy.[27] It acts as a cofactor that is integral to methylation processes which are important in reactions related to DNA and cell metabolism, therefore, deficiency of vitamin B12 may lead to disruption of DNA and cell metabolism which may cause serious clinical consequences [7; 1]. Intracellularly vitamin B12 is converted to two active coenzymes, methylcobalamin in the cytoplasm and adenosylcobalamin in the mitochondria. These coenzymes are necessary for the homeostasis of methylmalonic acid (MMA) and homocysteine [7; 2,3]. Vitamin B12 acts as a cofactor in the conversion of methylmalonic acid into succinyl-CoA. Methionine is converted to homocysteine and then homocysteine is further converted to amino acids cysteine or resynthesized into methionine. [7] Deficiency of vitamin B12 also leads to elevated levels of homocysteine and methylmalonic acid. It was found out that MMA concentration were shown to be elevated in nearly every patient with hematologic or neurologic abnormalities due to vitamin B12 deficiency and when treated with vitamin B12, MMA concentration was found to be corrected.[28] Elevated levels of total homocysteine (tHcy) are found to be a risk factor for cardiovascular disease.[20] Homocysteine causes peroxidation and generation of free radicals which causes inflammation and acute endothelial dysfunction, which leads to acceleration of atherosclerotic process predisposing to cardiovascular disease [24; 3]. An elevated level of homocysteine and deficiency of folate and vitamin B12 are risk factor for birth defects, poor pregnancy outcomes, and neurocognitive performances [20; 3-5]. Megaloblastic anemia is commonly seen in vitamin B12 deficient patients. Vitamin B12 deficiency is more common in elderly patients, but it is often not investigated or unrecognized because of subtle clinical manifestation[1; 1-4]. In India, very little appreciation is been given to vitamin B12 deficiency among the Indian medical professionals and policy makers. This may be due to various reasons: 1) it is not routinely measured in clinical practice, 2) despite of low level of circulating vitamin B12, signs for specific neurological or haematological syndrome consistent with vitamin B12 deficiency are rare, 3) the reports of prevalence, majority of them are based on clinical data and, therefore, may not represent community prevalence.[20] PREVALENCE OF VITAMIN B12 DEFICIENCY IN SURVEYS: Vitamin B12 deficiency is widespread in developing countries like Africa, India and South and Central America mostly due to low intake of animal products, particularly among the poor [28; 48]. Various studies have been performed to find out the prevalence of vitamin B12 deficiency in India. The prevalence of vitamin B12 depends on various factors such as age, dietary habits and socio-economic status. So depending upon the different factors various data have been obtained for vitamin B12 deficiency. A study performed on the urban population of Delhi showed to have a prevalence of 43%, this study includes parameters such as age and sex. [18] A Pune study showed the prevalence of 67%, the study was only performed on men and included parameters such as socioeconomic status, lifestyle, dietary habits and medical history.[20] A study done in BhujKutch showed the prevalence of 44.2%, it only included data from the higher socio- economic class.[14] Such a high prevalence of vitamin B12 deficiency indicates that there is immediate need of some action or a policy to prevent it. The prevalence of vitamin B12 deficiency in US population vary with age groups and was found to be 3% in those aged 20-39-year-old, 4% in those aged 40-59-year-old, and 6% in those aged 70-year-old.[10] This shows that compared to the American population, the Indian population is widely prevalent to vitamin B12 deficiency this may be due to more vegetarian population and poor lifestyle. A study performed by Sanket K. et al in Western Maharashtra on 100 patients out of which 33% were vegetarian. The result showed that 6% patients had neuropsychiatric manifestation, 1% patients had depressive illness, 0% patients had dementia, 1% patients had forgetfulness, 0% patients had mania/hallucination and 1% patients had chronic headache [30]. CLINICAL MANIFESTATION OF B12 DEFICIENCY: Vitamin B12 deficiency can be characterized by fatigue, constipation, megaloblastic anemia, weakness, weight loss, loss of appetite. [26;1,3,27] It can also cause some neurological changes like numbness and tingling in the hands and feet.[26;5,28] Other symptoms of deficiency include depression, difficulty in maintaining balance, confusion, poor memory, dementia and soreness of the mouth or tongue[26;29]. The neurological symptoms of Vitamin B12 deficiency can also occur without anemia, so early diagnosis is important to avoid irreversible damage [26,6]. Symptoms of vitamin B12 deficiency in infants includes failure to thrive, developmental delay, megaloblastic anemia and movement disorder[26;30]. CAUSES OF VITAMIN B12 DEFICIENCY: Vitamin B12 is mainly derived from animal foods like milk, fish, and dairy. According to FAO and USFDA 20%-42% of the Indian population are vegetarian since vitamin B12 is mostly obtained from animal food, vegetarian diet becomes the most common cause of vitamin B12 deficiency. Other common causes [7; 5-9]: 1) Impaired gastric absorption Example: Gastrectomy (partial or total), Pernicious anemia, and Impaired intestinal absorption for Eg. Ileal resection or disease like tuberculous ileiris and Crohn's inflammatory bowel disease; Blind loop syndrome, Parasites like bacterial overgrowth, giardiasis, and fish tapeworm; Luminal disturbance like in case of chronic pancreatic disease and gastrinoma 2) Decreased intake Example: Malnutrition, Reduce intake of animal product, strict vegan diet. 3) Pancreatic insufficiency 4) Congenital/ inherited Example: Intrinsic factor receptor deficiency/defect, Cobalamine mutation (C-g-1 gene), Transcobalamin deficiency, Congenital deficiency of intrinsic factor like in the case of "juvenile" pernicious anemia. 5) HIV and Haemolysis 6) Drugs such as Alcohol, Metformin, Nitrous oxide, Proton pump inhibitor (E.g. omeprazole), H2 receptor antagonists (E.g. Ranitidine), Colchicine, Phenytoin, Macrolide may also lead to vitamin B12 deficiency. POPULATION AT RISK OF VITAMIN B12 DEFICIENCY: The main cause that leads to vitamin B12 deficiency is malabsorption from food, dietary deficiency, pernicious anemia and postsurgical malabsorption [26; 12]. However in many cases the exact cause of deficiency is unknown. The following population groups are the one that are most likely to have vitamin B12 deficiency. Vegetarian diet: population who are strict vegetarian or vegan are the one at greater risk than Lacto-ovo vegetarians and nonvegetarians who are having vitamin B12 deficiency because animal products are the main source of vitamin B12 compare to the natural food sources [26; 5]. Fortified breakfast cereals, milk, yogurt, fruits and cheese are some of the dietary sources of vitamin B12 for strict vegans. Women who are pregnant and lactating and follow a strict vegetarian diet and their infants: during pregnancy vitamin B12 crosses the placenta and is present in breast milk. Women who consume no animal products when breastfed their infants may have very limited reserves of vitamin B12 and their infants can develop deficiency within months of birth [26; 5, 43]. If the deficiency is undetected or untreated in infants it can lead to severe and permanent neurological damage. In America, The American Dietetic Association recommends taking vitamin B12 supplements for vegans and Lacto-ovo vegetarians during both pregnancy and lactation. This is to ensure that enough vitamin B12 is transferred to the fetus and infant [26; 44]. Women who are pregnant and lactating and follow strict vegetarian diets should consult with a pediatrician regarding supplemental vitamin B12 for their infants and children [26; 5]. History of gastrointestinal surgery: surgery in the gastrointestinal tract, such as surgery to remove all or a part of stomach, weight loss surgery, often leads to loss of cells that secrete intrinsic factors and hydrochloric acid [26; 5, 39, 40]. This reduces the amount of vitamin B12 absorbed from the food [26; 41]. Removal of the distal ileum by surgery can also result in the reduce ability to absorb vitamin B12. Individual who undergoes such surgical procedures should be monitored preoperatively and postoperatively for vitamin B12 deficiency [26; 42]. Pernicious anemia: it is a condition which is characterized by a lack of intrinsic factors and affects 1%-2% of older adults [26; 11]. In this condition, the absorption of vitamin B12 from the gastrointestinal tract is reduced [26; 3, 5 9, 10]. Intramuscular vitamin B12 is given for treating pernicious anemia. In the absence of intrinsic factor approximately 1% of the oral vitamin B12 can be absorbed passively [26; 11], therefore the high dose of vitamin B12 can also be an effective treatment. Older adult: an older individual who are suffering from atrophic gastritis which decreases the secretion of hydrochloric acid in stomach results in decreased absorption of vitamin B12 [26;5,11,32-36]. The decrease levels of hydrochloric acid promote the growth of normal intestinal bacteria, these bacteria use vitamin B12, further reducing its level.[26;37] Gastrointestinal disorder: Individual who is suffering from disorders of stomach and intestine such as celiac disease and Crohn's disease are unable to absorb enough amount of vitamin B12.[26;12,13] The initial symptoms are cognitive function resulting from early vitamin B12 deficiency followed by megaloblastic anemia and dementia. VITAMIN B12 DEFICIENCY IN CARDIOVASCULAR DISEASES: The most common cause of death in industrialized countries is cardiovascular diseases such as the United States, and it is rising in developing countries. The various risk factors for cardiovascular disease include elevated low-density lipoprotein (LDL) levels, low levels of high-density lipoprotein (HDL), high blood pressure, diabetes and obesity [26;45] Another risk factor identified for cardiovascular disease is elevated levels of homocysteine. Homocysteine is derived from methionine that is normally present in the blood. Its elevated levels are thought to promote thrombogenesis, lipid peroxidation, impair endothelial vasomotor function and induce vascular smooth muscle proliferation [26;46,47,49]. The link between elevated levels of homocysteine with coronary heart disease and stroke has been proof from retrospective, cross-sectional and prospective studies [26;46,49-58]. Metabolism of homocysteine involves vitamin B12, folate, and vitamin B6. In the deficiency of vitamin B12, homocysteine level is increased due to inadequate function of methionine synthase [26;6]. Several randomized controlled trials indicate that combination of vitamin B12 and folic acid supplement with or without vitamin B6 resulted in decreased levels of homocysteine in people suffering from a vascular disease or diabetes and in young adult women [26;56-67]. In another study which was conducted on older men and women who were given multivitamin/ multimineral supplement for 8 weeks experienced a significant decrease in homocysteine levels [26;68]. Atherosclerosis is accelerated due to inflammation and acute endothelial dysfunction which is caused by the presence of free radicals, generated through lipid peroxidation mediated by homocysteine. The theory that there is a positive relation between high homocysteine levels and coronary artery disease (CAD) was first proved in a clinical study by Wilcken and Wilcken in 1976 [24;3]. Low vitamin B12 levels and hyperhomocysteinemia is most common in Indian men and particularly vegetarians and urban residents [24;4] VITAMIN B12 DEFICIENCY IN DEMENTIA AND COGNITIVE FUNCTION: Vitamin B12 deficiency causes accumulation of homocysteine in the blood and also decreases levels of substances which are needed to metabolize neurotransmitters [26;70]. Observational studies have shown a positive relation between elevated levels of homocysteine and the incidence of Alzheimer's disease and dementia [26;6,47,71]. Low vitamin B12 levels have also been positively related with decreased cognitive function. EXCESSIVE VITAMIN B12: An excessive level of vitamin B12 has no harmful impact on health because of its low potential for toxicity. The IOM states that "no adverse effects have been associated with excess vitamin B12 intake from food and supplements in healthy individuals" [26;5]. INTERACTION OF VITAMIN B12 WITH MEDICINS: There are several medications which interact with vitamin B12 and might adversely affect its level. Given below are several examples of interactions: CHLORAMPHENICOL: It is a bacteriostatic antibiotic. Vitamin B12 plays an important role in red blood cell formation and Chloramphenicol can decrease new blood cells. There for Chloramphenicol decreases the effect of vitamin B12. PROTON PUMP INHIBITORS: They are used in the treatment of gastroesophageal reflux disease and peptic ulcer Eg. Omeprazole and lansoprazole. These drugs suppress the production of gastric acid leading to malabsorption of vitamin B12 [26;83-85]. H2 RECEPTOR ANTAGONISTS: These drugs are used in the treatment of peptic ulcers, Eg. Ranitidine, famotidine and cimetidine. They reduce vitamin B12 absorption from foods by slowing the release of hydrochloric acid into the stomach [26;90]. METFORMIN: Metformin is the most commonly used drug for treatment of type 2 diabetes. It has been reported that metformin reduces vitamin B12 level by 25%. [13;10,12]. The possible mechanism through which metformin reduces B12 level includes alterations in intestinal mobility, alteration in the calcium-dependent uptake by ileal cells of the vitamin B12 intrinsic factor and increased bacterial overgrowth. Case reports and small studies ha reported that 10-30% patients taking metformin have reduced vitamin B12 absorption [26;92,93]. Various studies have suggested that if calcium given as a supplement may help to improve B12 malabsorption caused by metformin [26;92,93], but not every researcher agree [26;95]. HOW VITAMIN B12 DEFICIENCY IS DETERMINE: Several tests are available which reflect the physiological, static and functional status of vitamin B12. There is still no perfect test for measuring vitamin B12 deficiency. Measuring the serum cobalamin level remains the favored decision. [7;4]. The other test includes measurement of methylmalonic acid level, consider as the second line test, it helps to clarify the false results of underlying biochemical and functional deficiencies. Measurement of holotranscobalamin level shows an indeterminate “grey area” and therefore should be followed by methylmalonic acid test. Measurement of homocysteine level also shows B12 deficiency but is less accurate than methylmalonic acid [7;4]. Because of various reference ranges are available for B12 deficiency, it results in an inability of final definition for clinical and subclinical deficiency states. Physiological examination: The physiological parameters which reflects vitamin B12 deficiency includes full blood count (mean cell volume and hemoglobin), blood film, reticulocyte count and lactate dehydrogenase. Macrocytosis is the most well-known trigger for checking vitamin B12 level. Bone marrow biopsy can also be done in cases where the diagnosis is unclear or the patient is not responding adequately to the treatment. Patient who are concominantly suffering from iron deficiency may not show morphological features of B12 deficiency until the iron deficiency is resolved. Macrocytosis is absent or masked by thalassaemia trait [7;5-7]. Serum vitamin B12 level or cobalamin level: It is the most common method used to evaluate the level of vitamin B12 in serum. It also includes measurement of both serum holohaptocorrin and serum holotranscobalamin which may mask the actual result or show false deficient state. This method is cheap compare to other methods and uses an automated method and competitive-binding immune chemiluminescene [7; 2, 4, 14-17]. Level of Holotranscobalamin: Decrease level of holotranscobalamin in serum are consider as an early marker for vitamin B12 deficiency in addition to elevated levels of MMA and homocysteine. Holotranscobalamin is made of vitamin B12 attached to a transport protein transcobalamin II. It is an active metabolite of vitamin B12 which is readily taken up by all the cells and represents 6%-20% of total serum vitamin B12 [29;23]. Decrease in level of holotranscobalamin occurs even before elevation in homocysteine and MMA level occurs [29;24]. For vitamin B12 deficiency holotranscobalamin level is been consider as most sensitive marker followed by MMA [29;23,25]. But this test cannot be performed in patients having renal impairment as its increases in them [29;23]. Due to its high cost and lesser availability then MMA and homocysteine test make it difficult to acquire wide clinical acceptance. Level of Methylmalonic acid: Due to deficiency of vitamin B12, methylmalonic acid gets accumulated because vitamin B12 is required for the conversion of methylmalonic acid in to succinyl-CoA. Its elevated level act as the indicator for vitamin B12 deficiency in tissues and remains persistent for several days even after the replacement therapy is started [7;2]. This test is been consider as the most representative marker for metabolic vitamin B12 insufficiency. In older patients (>65years) and those with impaired renal impairment the levels can be falsely increased which me lead to false diagnosis. This method is expensive as methylmalonic acid is measured by gas chromatography and mass spectrometry. Total Homocysteine level: Total homocysteine levels in plasma are also increased in vitamin B12 deficiency at the early course of deficiency. This test is sensitive but cannot be consider as specific test for B12 deficiency as homocysteine levels are also increased in folic acid deficiency, B6 deficiency, renal failure and hypothyroidism. The reference range varied with the different technique used but the most preferred range is >15 μmol/L as high level of homocysteine [7]. Fig 2 shows the algorithm for the diagnosis of vitamin B12 deficiency [30;3,14]. Fig 2: Algorithm for the diagnosis of vitamin B12 deficiency A study done on 406 patients diagnosed with vitamin B12 deficiency showed that 98.4 percent patients had elevated levels of methylmalonic and 95.9 percent had elevated homocysteine levels. Out of 406 patients 1 patient showed normal level of both metabolites resulting in 99.8 percent sensitivity when homocysteine and methylmalonic levels are consider for diagnosing. It was also found that 28 percent patient had normal hematocrit levels and 17 percent had normal mean corpuscular volumes [30;10]. This study suggest that methylmalonic acid and homocysteine levels can be consider as the early marker for tissue vitamin B12 deficiency, even before hematological manifestations occur. TREATMENT: The treatment should be started within the few days of confirmed diagnosis. In case of any neurological conditions the treatment should be started immediately. In case of neurological disturbance and impaired cognitive state a specialist should be concerned. Neurological symptoms are also seen in the absence of haematological changes, so the treatment should be started early to prevent permanent neurological disability. In emergency conditions such as major anemia with cardiovascular compromise can be treated with packed red cell transfusion [7; 24]. Table 1: shows the Parenteral and oral treatment for treating vitamin B12 deficiency in normal and special conditions. ROUTE OF CONDITION DOSE ADMINISTRATION Intramuscular treatment Standard treatment for 1000 µg IM three times a patients without any week for two week [7; 4,25] neurological involvement For treating neurological 1000 symptoms µg IM given on alternate days for up to three weeks or until there is no improvement [7; 4,25] For treating irreversible cases 1000 µg IM should be given for example pernicious for lifelong [7; 26,27] anemia, inflammatory bowel syndrome and deficiency due to malabsorption syndrome Oral treatment Standard treatment neurological for 1000 µg and 2000 µg daily and [7; 28] haematological symptoms Table 1: Parenteral and Oral treatment for vitamin B12 deficiency. During pregnancy the treatment can be reviewed when the patient is fully replete and the causative agent is removed [7; 4, 26, 27]. Oral treatment can be considered when deficiency is mild or subclinical with no clinical symptom or when the absorption and compliance are not a problem [7: 4, 28]. Cyanocobalamin and Hydroxocobalamin are the main drugs used for the treatment of vitamin B12 deficiency. Methylcobalamin is the active form of Hydroxocobalamin. Hydroxocobalamin is well tolerated and have rare side effects such as itching, chills, hot flushes, fever, exanthema, nausea, dizziness and very rarely anaphylaxis [7; 4, 26 27]. Cyanocobalamin is licensed and outlined in the British National Formulary as an oral preparation which is given at a dose of 50-150 µg daily [7; 25] and its active form is Deoxyadenosylcobalamin.