Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
1698
Evaluation of Contractile State by Maximal
Ventricular Power Divided by the Square
of End-Diastolic Volume
David A. Kass, MD, and Rafael Beyar, MD, DSc
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
Background. Maximal ventricular power (PWRIUOX) reflects contractile state and has the
potential to be noninvasively determined. However, its sensitivities to preload, afterload
resistance, and inotropic state are incompletely defined. The present study determines these
dependencies and proposes a novel power-based contractile index that is little altered by load.
Methods and Results. Seven open-chest, autonomically blocked dogs were instrumented with
a proximal aortic flow probe, central aortic and ventricular micromanometers, and a
conductance catheter for ventricular chamber volume. Preload was transiently reduced by left
atrial hemorrhage, and afterload was increased by intraortic balloon inflation. Inotropic state
was pharmacologically altered by lidocaine, dobutamine, propranolol, or verapamil. PWRK
was highly preload sensitive, altering 1.7±0.1-fold a given percent change in end-diastolic
volume (EDV). This preload dependence was reduced by dividing PWRDI.a by EDV but was
virtually eliminated when PWRmaX was divided by EDV2. This latter index also displayed little
change in response to as much as 60%So increases in afterload resistance. PWRaI,X/EDV2 varied
directly with inotropic state, correlating to both the slope (Ees) of the end-systolic pressurevolume relation (PWRm. * 1,000/EDV2=0.31 * E,s-0.04, r=0.82, p<0.001) and the slope (A) of
the dP/dt.-EDV relation (PWRMt. 1,000/EDV2=0.025 * A+0.02, r=0.86, p<0.001). PWRm.
values determined from the product of ventricular pressure and flow versus central aortic
pressure and flow were nearly identical over a broad loading range, indicating that PWR,., may
be noninvasively assessed (i.e., without requiring left ventricular chamber pressure).
Conclusions. PWRU, divided by EDV2 provides a measure of contractile function that is little
influenced by loading conditions and has potential for noninvasive clinical use. (Circulation
_
1991;84:1698-1708)
V entricular contractile state is most effectively
assessed by indexes derived from pressurevolume relations. Examples such as the
end-systolic pressure-volume relation (ESPVR),1,2
stroke work or dP/dtmax (maximal rate of pressure
rise) -end-diastolic volume (EDV) relation,2-5 or the
ejection fraction-afterload stress relation67 are each
obtained by measuring a pump function variable over
a loading range to generate an index that incorporates load and is therefore more specific to contracFrom the Division of Cardiology (D.A.K), Department of
Internal Medicine, The Johns Hopkins Medical Institutions, Baltimore, Md.; and the Department of Biomedical Engineering and
the Division of Cardiology (R.B.), Technion IIT, Haifa, Israel.
Supported by National Heart, Lung, and Blood PhysicianScientist Award HL-01820 (D.A.K) and by USA-ISRAEL Binational Science Foundation grant 84-00380/2. D.A.K. is an
Established Investigator of the American Heart Association.
Address for correspondence: David A. Kass, MD, Carnegie
565B, Division of Cardiology, The Johns Hopkins Hospital, 600
North Wolfe Street, Baltimore, MD 21205.
Received September 17, 1990; revision accepted May 21, 1991.
tile state change. However, these relations require
measurement of ventricular chamber pressure in
combination with dimensions (or volume); thus, their
use has been primarily limited to invasive clinical and
experimental studies. Although a noninvasive assessment of contractility has clear practical and clinical
benefits, it remains elusive.
A group of contractility indexes with potential for
noninvasive use are those based on ventricular
power. Power is the instantaneous product of pressure and flow and thus is the rate of ventricular work.
Maximal ventricular power (PWRmax) is an ejection
phase index occurring early after the onset of aortic
flow when central arterial and ventricular pressures
are similar. Thus, in the absence of aortic valve
disease, central arterial pressure could substitute for
ventricular pressure in the determination of power.
The power indexes (in particular, maximal power and
rate of power rise) were studied 15-20 years ago by
several groups.8-12However, when these studies were
conducted, methods for power measurement were
Kass and Beyar LV Contractility and Ventricular Power Index
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
both invasive and not very precise. Because the
indexes did not offer clear advantages over other
more general and conceptually powerful approaches,
they were in large part abandoned. However, recent
developments in pressure, flow, and dimension recording techniques may now enable PWRma, to be
noninvasively determined, rekindling interest in
these measurements.
In the present study, we examined the preload,
afterload resistance, and inotropic sensitivity of
PWRmI. Invasive pressure-volume and pressure-flow
data were obtained in reflex-blocked anesthetized
dogs to accurately assess each dependency. Based on
recent studies of the load and inotropic sensitivities
of stroke work,4 we anticipated that PWRm, would
display marked preload sensitivity but minimal
change from afterload resistance. We further hypothesized that normalization of PWRmax to the square of
EDV (PWRmax/EDV2) would in large part eliminate
the preload dependence and thus generate a reasonably specific index for contractile state. Our results,
based on both experimental data and theoretical
model analysis, are consistent with these predictions.
Methods
Preparation
Seven adult mongrel dogs (25-30 kg) were anesthetized with intravenous pentobarbital (20 mg/kg)
and fentanyl (0.3-0.5 mg/kg), intubated, and ventilated on a volume respirator. The chest was opened
via a lateral thoracotomy at the fourth intercostal
space, and the pericardium was incised. The proximal
periaortic fat was dissected free, and a 12- or 16-mm
ultrasound flow probe (Transonics, Ithaca, N.Y.) was
placed around the root. Two micromanometertipped catheters (Millar, Houston, Tex.) were positioned - one in the central aorta via the right brachial
artery, and the other in the mid left ventricular
chamber via a femoral artery. A large intravascular
balloon occlusion catheter (Meditech, Billerica,
Mass.) was placed in the proximal descending aorta.
A large-bore cannula was introduced into the left
atrium and attached to a reservoir primed with
dextran and normal saline. Animals underwent autonomic reflex blockade before study (20 mg/kg hexamethonium, bilateral vagotomy).
An 11-electrode volume (conductance) catheter
was placed in the left carotid artery and advanced to
the ventricular apex. This catheter provided an online volume signal for pressure-volume loop analysis.13,14 The principles, design, use, and limitations of
the conductance catheter have been reported elsewhere.1516 All catheters were placed with the use of
fluoroscopic guidance. In addition to inspection of
volume catheter position, segmental volume signals
from the catheter were individually displayed to
determine those electrode segments within the ventricular chamber compared with those at or above the
aortic valve. An electronic switch device enabled only
those segments within the chamber to be used in the
1699
total volume signal. Volume catheter calibration was
performed by determining the parallel conductance
offset (average value of at least four separate estimates) using the hypertonic saline technique validated previously15 and a mean gain obtained from
the ratio of integrated flow (stroke volume) from the
ultrasound flow probe to catheter-derived stroke
volume.
Pressures, volume, and flow data were digitized at
200 Hz using custom-designed analog-digital acquisition and signal display software. Raw data were stored
on removable hard disks for subsequent analysis.
Protocol
Preload and afterload sensitivity. Preload was transiently reduced by gradual left atrial hemorrhage into
a reservoir yielding an average of 27±3 sequential
loops for analysis. Preload was defined by the diastolic volume obtained from each pressure-volume
loop. Afterload resistance was transiently increased
by inflation of the intra-aortic balloon, yielding an
average of 13 differently afterloaded beats for each
heart. Afterload resistance was quantified by the
effective arterial elastance (Ea)'18"9 equal to the ratio
of end-systolic pressure to stroke volume. At a constant heart rate, this ratio primarily reflects total
vascular resistance. This can be seen by approximating mean arterial pressure with end-systolic pressure.18 Mean resistance (R) is equal to the following
equation:
R=MAP/CO=MAP/(HR SV)=(MAP/SV) . T (1)
where MAP is mean arterial pressure, CO is cardiac
output, HR is heart rate, SV is stroke volume, and T
is the cardiac cycle length (seconds). Therefore,
Ea=end-systolic pressure/SV ~MAP/SV= R/T. Thus
at constant T, which occurred in the present study
because of autonomic blockade, Ea primarily reflects
total resistance (sum of peripheral resistance and
characteristic impedance).
All data were collected with ventilation held at end
expiration. Preload reduction data were obtained in
all seven animals at two different contractile states
(control and reduced via 4 mg/kg i.v. lidocaine). In
two animals, additional preload reduction data were
obtained with enhanced contractile state (dobutamine, 10-15 g/kg/min). Afterload increase data
were determined at one contractility level in a total of
six animals.
Contractile sensitivity. The seven animals described
above provided a total of 16 different contractile
states. To supplement these data and thereby better
define power index sensitivity to contractile state, we
reanalyzed data from a previously published study
(six dogs) of contractility effects on pressure-volume
relations.20 In this prior investigation, inotropic state
was altered over a wide range by intravenous administration of propranolol and verapamil. Aortic flow
had not been directly determined in these experiments; therefore, flow and thus power were calcu-
Circulation Vol 84, No 4 October 1991
1700
correlation (y=0.98x- 0.02, r=0.96, SEE=0.2,
n =484, p<0.0001) that was not significantly different
from the line of identity.
Combining both present and prior data sets yielded a
total of 43 different contractile conditions that were
used to assess power index inotropic sensitivity. Power
index values were compared with the slope of the
ESPVR (Ees) and the slope of the relation between
dP/dtmax and EDV. Both of these relations (one, an
end-ejection phase; the other, an isovolumic phase)
have been extensively studied and found to be loadinsensitive measures of contractile function. 2,4,5
A
y = 0.98x-.02
r = 0.96 SEE = .2
n = 484
5
4.
6
A
3.
x
2
0
E
LI
Calculations
Ventricular power [PWR(t)] is the product of
instantaneous left ventricular pressure [PLv(t)] and
rate of volume change [dV/dt]:
1*
0~a.
2
POWERmaX
3
4
( FLOW PROBE )
5
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
B
y = 1.03x - .09
r = 0.99 SEE = , 1 1
n = 484
5s
LJ 4
Li
a-
m 3.
2
E
3:
CL&
0
0-
PWR(t)-PLV(t). FAOW
PWRmax=[PAO(t) FAO(t)]max
0
1
2
POWERmOx
4
3
5
(LVP * FLOW)
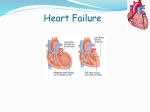
FIGURE 1. Panel A: Scatterplots comparing maximal ventricular power (PWR,,) determined from aortic probe vs. the
derivative of the conductance catheter volume signal (dV/dt).
Data (n=486) obtained by both techniques were well correlated and fell near the line ofidentity (y=0.98x-0.02, r=0.96,
p<O.0001). Panel B: Scatterplots comparing PWR,, determined from the product ofleft ventricular pressure (LVP) and
flow (abscissa) vs. central aoriic pressure and flow (ordinate).
PWR,,nX was virtually identicalfor both calculations, with data
(n=486) falling along the line of identity (y=0.95x+0.12,
r=0.99, p<0.0001).
lated by differentiating the volume [V(t)] signal. V(t)
first filtered with a five-point Hanning window,
and then dV/dt was digitally calculated using a fivepoint weighted slope. To verify the results of this
approach, PWRmax values obtained from the directflow signal versus d(V)/dt were compared over a wide
preload range in the present principal study group
(n=7) for which both measurements were obtained.
The results (Figure 1A) demonstrated an excellent
was
(2)
In the absence of mitral regurgitation (accepting a
small error from ignoring coronary blood flow), dV/dt
during systole,-aortic flow [FAO(t)]; thus:
(3)
PWRmax is determined as the peak value of PWR(t),
which is digitally calculated from the instantaneous
pressure-flow product.
An important consideration for noninvasive applications of PWRmax is the accuracy of its measurement
from central arterial (versus ventricular) pressure. To
test this, we compared PWRmax obtained from Equation 3 (i.e., [PLV(t) * FAO(t)]max) with the maximal
product of central aortic pressure and flow:
0
X
PWR(t)=PLV(t) * dV/dt
(4)
The comparison is shown in Figure 1B with individual points obtained from beats during transient
preload and afterload resistance change. The two
PWRma values were highly linearly correlated
(p<0.0001), falling along the line of identity.
Therefore, for the present study, PWRma, was calculated by using Equation 4.
In addition to PWRmaX, pressure-volume data were
used to obtain other measures of systolic function
such as ESPVR. The locus of points of maximal
(P/[V-VO]) for the multiple loops during preload
change were fit by linear regression to yield the endsystolic elastance (Ees), the slope of the ESPVR.
Another contractility index,5 the slope of the relation
between maximal pressure derivative and preload
volume, was also determined from these beats.
Statistical Analysis
The data were primarily in the form of multiple
points from each heart relating load (or contractility)
alteration to power index change; therefore, analysis
employed linear regression. To combine data from all
dogs and derive meaningful group statistics, a multivariate regression model was used that factored in
other condition variables as well as provided for
Kass and Beyar LV Contractility and Ventricular Power Index
A
1701
B
IL~A
0
X
l -
it
110
7~~~~~~~~13-
154
L46
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
-JliJD___UUuafri
Lit
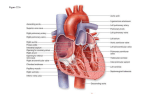
FIGURE 2. Panel A: Time plots showing preload dependence of maximal ventricular power (PWR>) (data obtained duing left
atrial hemorrhage). Left ventricular pressure and volume (LVP and LW), aortic pressure and flow (ABP and FLOW), and
ventricular power (POWER) (equals ABP multiplied by FLOW). Power units are converted to watts (mm Hg - mll
sec 1.333 10`4). PWR,,,, demonstrated the greatest percent reduction with decrease in volume, as it resulted from the product of
pressure and flow. Panel B: Time plot showing effect of increased afterload (data during balloon occlusion of descending aorta).
Recording channels are the same as in panel A. Although ventricular and aortic pressures rose, FLOW (both mean and peak) was
reduced, resulting in little net change in PWR",,,.
interanimal variation.21 For preload (EDV) dependence, the regression model was the following equation:
PWRindex=bo+bl * EDV+b2 Ea+b3 * LIDO
eiDi EDV
+b4* DOB+ 2 diDi+
i
Ea.
6
6
included. To assess the correspondence between
and contractility indexes (i.e., ESPVR and
dP/dtmaj-EDV relations), terms were included to
account for heart rate, preload volume, and afterload
power
(5)
i
where LIDO and DOB are dummy variables coding
for lidocaine or dobutamine (0 for control, and 1 for
drug), Ea is the afterload parameter obtained at
steady state before preload change, and Di represents dummy variables for each dog [Di= 1 for dog=i
and Di=0 for dog.i (for i=1-6), and Di=-1 for
dog=7]. The regression output provided the mean
regression of power index on EDV (bo and bl),
allowing for individual variation in each animal's
regression (di, ei) as well as for effects of afterload
(b2) and contractility (b3 and b4). The model was
simplified for afterload analysis because only one
contractile state was used, and Ea and EDV covaried
during transient aortic occlusion; thus, only one was
Statistical analyses were performed on an ATcompatible 286 computer using the SYSTAT (Evanston, Ill.) software package.
Results
Preload Sensitivity
A typical recording (signal versus time) obtained
during transient preload reduction is shown in Figure
2A. Power was digitally calculated from the aortic
pressure-flow product (measured in watts); all of the
other channels were obtained on-line. These data
demonstrate a strong dependence of PWRmax on
preload, a consequence of combined changes in
arterial pressure and peak flow.
The relation between PWRmaX and EDV is displayed directly in Figure 3 (left upper panel), showing data for a representative dog. Dividing PWRmax
1702
Circulation Vol 84, No 4 October 1991
PRELOAD CHANGE
AFTERLOAD CHANGE
*
S
X
4]
XW
4
0
z 5.
a.
0
140 bo
3
z
£y
2.
4-0-I.**1,#
0
10
20
0
ui
s0
,,,&4 la)*
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
o.6
0
S
4
5
o x 1.5
"qup
v.v v
W
2.0,
g1.5,
2' 0.5
O
AFrERLOAD (C0 - mmHg/Ml)
2-°r
z
2
2
END-DIASTOUC VOWME (m)
W
PWRMX
CLJ
g
U
-
o - PWRmax/EDV2. 1000
'* f#*0* % :g
**40010
4r**
**
:3z
fik
h **
ss
:
0
0
2 W5
z 2 .5.
_
0.6
o
-
1.0
C
o.o
t.o
NORMALIZED END-DIASTOLIC VOLUME
1.2
NORMALIZED
1.4
TERLOAD (40)
c
1.6
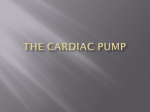
FIGURE 3. Scatterplots of maximal ventricularpower (PWR,.,,j) (*) and PWR,,jend-diastolic volume (EDV)2 (o) vs. preload
(EDV) and afterload (Ea) relations from a single dog. Upper panels: Raw data (P"WRm,,IEDV2 is multiplied by 1,000 to allow
plotting on the same axis), and the corresponding lower panels show the same data nornalized to the respective starting baseline
value for both power index and load parameter. PWRma. displayed a far greater dependence on altered preload vs. afterload
resistance, whereas PWR,,/EDV2 showed little change with either load intervention. Normalized plots enable relative percent
changes in power index vs. load to be discemed.
by EDV (not shown) reduced the preload dependence; however, dividing PWRmaX by EDV2 virtually
eliminated it (see figure; note PWRmax/EDV2 is multiplied by 1,000 so it can be displayed on the same
axis). The left lower panel of Figure 3 shows the same
data but with each index (and EDV) normalized to
its respective baseline value; thus, all start at 1.0. This
reveals that PWRmax is reduced by nearly 60% for a
30% decrease in EDV. Dividing PWRmax by EDV2
yields an index that deviates little from 1.0 despite
EDV change, which is consistent with minimal preload dependence.
Individual regressions for normalized PWRmx versus EDV (as in Figure 3, left lower panel) are
provided in Table 1. Each relation revealed strong
preload dependence, with an average slope of
1.71+0.48 and r2 of 0.981. Data from all 16 runs were
graphically combined by averaging values over
equally spaced normalized volume ranges (Figure 4).
Dividing PWRmaX by EDV reduced the preload dependence of PWRmaX but did not eliminate it. In
contrast, PWRmaX/EDV2 was only minimally influenced by marked preload change.
Multiple regression analysis of preload dependence (using the raw data) is provided in Table 2.
EDV significantly influenced both PWRmaX and
PWRmax/EDV (p<O.OOl for both), whereas this was
not so for PWlRmax/EDV2 (p=0.624). Contractile state
TABLE 1. Preload Dependence of Maximal Ventricular Power
r2
SEE
Intercept
n
1.61
-0.68
0.967
0.04
21
2.60
-1.63
0.978
0.04
15
1.27
-0.24
0.994
0.02
13
1.40
-0.42
0.977
0.04
14
1.80
-0.77
0.994
0.02
44
2.36
-1.35
0.992
0.02
38
0.87
+0.12
0.973
0.02
14
1.17
-0.16
0.994
14
0.02
1.61
Sa
-0.61
0.993
0.01
27
b
2.45
-1.43
0.985
0.02
37
6a
1.19
-0.16
0.987
0.01
49
b
1.95
-0.91
0.971
0.04
13
c
1.92
-0.79
0.955
0.06
19
7a
1.93
-0.91
0.982
0.03
33
b
1.76
-0.75
0.984
0.03
40
c
1.42
-0.47
0.974
0.03
40
Mean
1.71
-0.70
0.981
0.03
27
±SD
0.48
0.48
0.012
0.012
13
Results of linear regression analysis of individual maximal
ventricular power (PWR,,a)-end-diastolic volume (EDV) relations are for each dog at varying contractility (a, b, c). Data were
first normalized so that both PWRma,x and EDV started at 1.0
before preload reduction. Slope, intercept, correlation index r2,
SEE, and number of points per regression (n) are provided.
Dog
la
b
2a
b
3a
b
4a
b
Slope
Kass and Beyar LV Contractility and Ventricular Power Index
1.5
PWR .,/EDV 2 i
W
-
NORMALIZED
POWER INDEX
PWR mx/EDV
0.5
PWR mm
1 i
0.6
I
0.7
0.8
0.9
NORMALIZED END-DIASTOLIC VOLUME
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
independently influenced each power index (increasing
with dobutamine and decreasing with lidocaine),
whereas Ea did not. Applying the same regression
model to the normalized data yielded a mean slope of
1.72+0.032 (p<0.001) for the PWRmax_-EDV relation
versus
0.11+0.064 (p=0.09) for the PWRmax/
EDV-EDV relation. In other words, for a 20%
decrease in EDV, PWRmax declined by 34%, whereas
PWRma/EDV changed by only 2%.
Afterload Sensitivity
Figure 2B displays signal-versus-time plots during
acute descending aorta balloon inflation. Despite an
TABLE 2. Multivariate Regression Analysis of Preload Dependence of PWRM1,, PWRmSXJEDV, and PWRmax/EDV 2
Coefficient SEE Two-tailed p Multiple r
PWRmax
0.893
<0.05
0.560 0.101
Constant (bo)
<0.001
0.063 0.006
EDV (bl)
0.08
-0.019 0.011
Ea (b2)
<0.001
-0.827 0.064
LIDO (b3)
1.588 0.080
<0.001
DOB (b4)
PWRmaR/EDV
0.926
<0.001
1.945 0.547
Constant (bo)
<0.001
0.131 0.020
EDV (b1)
0.127
-0.055 0.036
Ea (b2)
<0.001
-2.777 0.217
LIDO (b3)
<0.001
6.203 0.269
DOB (b4)
PWRmaR/EDV 2
0.951
<0.001
2.223 0.211
Constant (bo)
0.624
0.004 0.008
EDV (b1)
0.080
-0.025 0.014
Ea (b2)
<0.001
0.084
-0.968
LIDO (b3)
<0.001
2.491 0.104
DOB (b4)
PWRm,ax maximal ventricular power; EDV, end-diastolic volume; Ea, arterial elastance; LIDO, lidocaine; DOB, dobutamine.
See "Methods" (Equation 5) for a description of regression
model. A total of 419 points (16 runs from seven animals) were
used. Partial regression coefficients and their respective standard
errors (SEE) and probability values are provided. The overall
regression correlation coefficient (multiple r) is also provided.
^
I U .U
1.0
1703
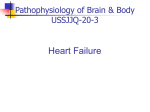
FIGURE 4. Plots of group data for
preload dependence of maximal venticularpower (PRmax), PWR,,enddiastolic volume (EDV), and PWR,n,j,/
EDV2. Data from each run (n=16)
were normalized to baseline (as in Figure 3, left lower panel), so each started
at the point (1,1). Data were then
averaged for every 0.05 change in normalized volume, and mean +SEM values are shown. Lines shown connect
the mean points. For a 30% reduction
in EDV (i.e., 1.0 to 0.7), PWR,mx decreased by more than 50%. Dividing
PWR,,WX by EDV reduced the load dependence, but dividing it by EDV2
essentially removed preload variation
over a broad range.
increase in systolic pressure and Ea, PWRmax was little
altered. This occurred because there was a small but
significant decrease in peak flow as pressure increased. Because PWR=P * F, it is proportional to
R F2, where R is resistance, P is pressure, and F is
flow. For the group data, resistance increased by
57%, whereas peak flow decreased by 24%. Heart
rate was not significantly altered. Thus, the net power
change during aortic occlusion could be predicted as
(1.57 0.762)=0.91, or 91% of baseline power with
an almost 60% increase in afterload resistance. In the
observed data, PWRmax actually increased slightly
with aortic occlusion; however, this was more likely
due to simultaneous increases in EDV during aortic
occlusion (see Figure 2B). Figure 3 (right panels)
also shows an example (from the same dog) of the
PWRM.-afterload relation (panel C shows raw data,
and panel D shows the same data normalized to
baseline). Again, dividing PWRI,T,x by EDV2 minimized load dependence.
Group data, with PWRm. indexes and afterload
resistance (Ea) normalized to their respective baseline control values, are shown in Figure 5. None of
the indexes displayed much change for an initial 20%
increase in afterload. However, with further resistance increase, concomitant EDV increase led to
significant increases in PWRmax. Normalization to
EDV reduced this effect, but the changes were in
large part eliminated by dividing by EDV 2. Multiple
regression results for the afterload change (again,
based on the raw data) are provided in Table 3 and
were consistent with the graphic analysis.
Contractile State Sensitivity
Although PWRmax/EDV 2 was relatively insensitive
to preload and afterload resistance change, it correlated well with several standard measures of contractility. Comparisons were made to two indexes: the
slope of the ESPVR (Ees), and the slope of the
dP/dtmax-EDV relation (A). Both relations were derived using multiple pressure-volume loops obtained
during preload reduction under each contractile
Circulation Vol 84, No 4 October 1991
1704
1.5
X
FIGURE 5. Plots of average afterload dependence of power indexes. Data were normalized
PWRmOx/ EDV in a manner analogous to that shown in Figure
PWR mox/ EDV2 3 (right lower panel). Spacing between means
was less constant due to an attempt to include
each animal's data at each point despite variation between responses. Although maximal
PWR mox
x
z
W
0
1 .0
0
w
aJ
0.5
0
z
1.2
1.6
1.8
1.4
NORMALIZED AFTERLOAD (Ea)
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
state. PWRmax/EDV2 (y) correlated with both slopes
(y=0.025 * A+0.02, 2=0.86, p<0.001 for dP/
dtmax-EDV; y=0.31 Ee,-0.04, r=0.82,p<0.001 for
Ee.) Figure 6 shows the results of these comparisons
as well as the 95% prediction intervals for the
regressions.
To test whether simultaneous changes in heart rate,
preload, or afterload resistance that could accompany
drug-induced alterations in contractility influenced
the relation between PWRhaX/EDV 2 and Ee, or A, we
again used a multivariate regression model that included these variables. The only factor with a significant influence on PWRmax/EDV2 was EDV, and this
was true only for the regression of PWVRma/EDV2
versus Ees. In this instance, the dependence had a
small negative slope (-0.036+0.014) (i.e., power index decreased with increasing EDV), which is consistent with higher volume at low contractilities but
opposite to a direct preload effect as defined earlier.
Discussion
The purpose of the present study was to assess the
load and inotropic sensitivity of PWRmax and to determine whether a reasonably load-independent contracTABLE 3. Multivariate Regression Analysis of Afterload Dependence of PWR,, PWRDI. /EDV, and PWRIIJEDV2
Coefficient
SEE
Two-tailed p
Multiple r
1.006
0.100
0.049
0.008
<0.001
<0.001
0.993
4.846
0.093
0.223
0.035
<0.001
0.009
0.990
PWRmax
Constant (bo)
E. (bl)
PWRmaJ/EDV
Constant (bo)
Ea (bl)
PWRmax/EDV 2
Constant (bo)
2.139
0.145
<0.001
0.982
-0.010
0.022
0.673
PWRmax, maximal ventricular power; EDV, end-diastolic volume; Ea, arterial elastance.
See "Methods" for full description of regression model. Because
afterload data were obtained at one contractility level, this variable
was not included in this regression.
Ea (bl)
2.0
ventricularpower (PWRmn,Z) and PWRm,Jenddiastolic volume (EDV) each showed a slight
increase with aortic occlusion (due primarily to
simultaneous preload increase along with afterload resistance change), PWRm,J/EDV2 displayed less dependence.
tile index could be obtained by dividing PWRm,, by
EDV 2. These data revealed a very strong dependence
of PWRmSX on preload volume with much less effect
from varied afterload resistance. Dividing PWRmSX by
EDV2 minimized both load effects over a broad range;
however, PWRmaJEDV2 was sensitive to inotropic
change, directly correlating with Ees and the slope of
the dP/dtm,_-EDV relation. Finally, PWRma,, values
obtained from central aortic versus ventricular pressures (or aortic flow versus chamber volume derivative)
were very similar, supporting potential noninvasive
applications of this index.
Load Dependence of PWRn: Prior Studies
PWRmax incorporates many aspects of ventricular
performance, including magnitude and rate of pressure development, ejection rate, and ventricular
work. However, prominent preload dependence limits its usefulness. Previously, investigators have addressed normalization of PWRm.X in several ways. In
an early clinical study of patients with a wide variety
of disease conditions, Russell et a19 found a good
correlation between PWRmSIx/EDV and ejection fraction. However, this study did not systematically test
loading sensitivity, nor did it compare this ratio with
other load-insensitive measures.
Stein and Sabbah10 reported in a canine study that
the maximal instantaneous rate of power rise
[d(PWR)/dt]max was preload and afterload independent, despite the fact that PWR.SX itself varied with
load. However, although preload increase (dextran
infusion) led to little change in d(PWR)/dtm, systolic
pressure also changed little in this study and actually
decreased as much as 25 mm Hg in some cases. This
is opposite to what is expected from a pure preload
increase, suggesting that complex loading and/or
reflex activation occurred. Furthermore, the previously documented preload dependence of stroke
work4 as well. as PWRmaX shown in the present study
strongly suggest that d(PWR)/dtma should also be
volume sensitive. We confirmed this by determining
the maximal average rate of power rise for each beat
during the preload reduction runs. This mean rate
Kass and Beyar LV Contractility and Ventricular Power Index
80 T
O0 Flow by flow probe
* Flow by d(Volume)/dt
0C
CL
Cd4
1705
604
>
E
LUI
".J0X
C:]
0
0~
40-
rl*_
20-
C-
, A-
15
5
10
Ees (slope of ESPVR) mmHg/mi
('4
20
81
0
-e
20
40
60
END - DIASTOLIC VOLUME (ml)
FIGURE 7. Scatterplot of preload dependence of mean rate
of maximal ventricular power (PWRma,) increase. Maximal
power was divided by time to peak power (ttPP) (from onset of
aortic flow). Although prior studies had suggested this measure
to be preload independent,10 these data revealed as much
preload influence as observed with PWRmWC
0
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
W
"I
30
0~
150
50
100
200
SLOPE OF dP/dt,,-,, EDV RELATION
FIGURE 6. Scatterplots comparing maximal ventricular
power (PWRmax)/end-diastolic volume (EDV)2 vs. an ejection
phase index [slope of end-systolic pressure-volume relation
(ESPVR) (EeJ (upper panel)] and an isovolumic phase
index [slope of dP/dtr,-EDV relation (lower panel)]. Open
symbols show data from the seven animals in which aortic
flow was determined directly, and closed symbols show data
from the six animals in which flow was derived by differentiating the volume signal. Linear regression (solid line) and
95% prediction interval (dotted line) are shown. Power index
correlated well to both contractile state indexes.
was calculated by dividing PWRmax by the time interval from onset of flow to PWRmax. The data (Figure 7)
show nearly the same preload sensitivity observed
with PWRmax. Furthermore, d(PWR)/dtmax has the
disadvantage of requiring further differentiation,
which can amplify signal noise.
Last, another study normalized mean power (versus PWRma) to estimated diastolic wall stress.12
Incorporation of wall mass and geometry considerations via a stress formula may be useful for contrasting absolute values of power between subjects with
markedly different heart sizes or thicknesses; however, this requires modeling assumptions. The present data were obtained in normal canine hearts with
a fairly narrow range of cardiac masses, but in clinical
disease states, particularly those with substantially
increased chamber volume or mass, heart geometry
could be important. Stress normalization would be
less critical for predrug and postdrug intervention
measurements in the same patient or for studies
combining power measurements with exercise.
Why PWR,j/EDV2?
The notion that PWRmax/EDV2 should be fairly
free from load dependence yet sensitive to inotropic
state can theoretically be supported on several
grounds. Mean power is the product of mean pressure and flow and thus resistance multiplied by flow
squared. Power divided by volume squared is therefore proportional to resistance divided by seconds
squared. Mean arterial resistance is only minimally
altered (in the absence of reflexes) with steady-state
changes in circulating volume.22,23 Thus, at a constant
heart rate and contractile state such as during preload reduction in our protocol, PWRmax/EDV 2
should be little changed.
Another way to consider the preload dependence
of PWRmaX is to express power in terms of a timevarying elastance [E(t)]:
Power=P(t) * F(t)=P(t) * dV/dt
(6)
=E(t) * [V(t)-VO] . dV/dt
where P(t) is instantaneous ventricular pressure and
F(t) is instantaneous flow. Thus, power divided by
volume squared has units of elastance divided by
seconds. At a constant heart rate, it can be shown
that PWRmax/EDV2 should be proportional to Ees
(see "Appendix 1").
It is somewhat more difficult to predict the afterload dependence of PWRm, with a simple equation.
Because PWRmax occurs early in systole ("Appendix
2"), one might expect it to be more influenced by
changes in characteristic impedance (1Zci) than peripheral resistance. However, these two parameters
are difficult to vary independently in vivo. Therefore,
we assessed this issue by computer simulation. In our
model, the ventricle was represented by a timevarying elastance, and the arterial system was repre-
1706
Circulation Vol 84, No 4 October 1991
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
sented by a three-element windkessel. The simulation calculated both PWRmaX and PWRmIX/EDV2 for
pure changes in preload (EDV), peripheral resistance (Ra), and IZjI. Model output was obtained
(using typical values for Ees, Ra, IZJ, compliance,
EDV, and heart rate taken from our experimental
data) and then normalized to baseline so that the
results could be compared with the experimental
data shown in Figures 4 and 5.
The results (Figure 8) were remarkably similar to
those obtained experimentally. For preload (top panel), the model predicted a strong EDV dependence
of PWRmax but little-to-no dependence for PWRm,,/
EDV 2. Changing only peripheral resistance (middle
panel) over a twofold range altered both power
indexes only slightly (model outputs are superimposable as EDV was held constant and the data normalized to baseline). PWRma, eventually declines to zero
at either extreme of load (flow, and thus PWRmax,
equal 0 when Ra is o, and pressure, and thus PWRmaX,
equal O when Ra is 0), but plateaus in the physiological loading range, which is similar to that previously
reported for stroke work.19
Change in IZcl (lower panel) led to a somewhat
larger change in PWRmaX compared with pure change in
peripheral resistance; however, this effect was still fairly
small. Furthermore, as IZci is relatively difficult to vary
acutely pharmacologically or with exercise,24 this factor
is somewhat less critical. Aging alters IZ,1,25 and one
might anticipate differences in PWRmaX values as a
function of increased proximal aortic dimension and
stiffness due to age; this is under investigation.
MODEL SIMULATION
2.01
ts
-
* -
0
POWER
PE
PEAK POWER/EW2
1.5z
m
1.0 0...........................0 .......
0...........0.........0..
0.51
W
z
li'
W u.u0 i
0.7
0.6
0.8
0.9
1.C
NORMALIZED END-DIASTOLIC VOLUME
z
C3
2.0.
N
0
x
1.51
0.
1.0*_
0
N
0.5.
0
z
0.0
0.0
,
i
i
i
0.5
1.0
1.5
2.0
I
2.t5
NORMAIZED PERIPHERAL RESISTANCE
2.0
X
W
0
z
0
1.5.
1.01
N
0.5.
Limitations
Several experimental limitations should be considered. Aortic flow was measured by flow probe at the
aortic root; therefore, a small error was incurred in
not including coronary flow in this measurement.
Heart rate was maintained constant in these studies,
and as with dP/dtma, heart rate change alone could
alter PWRma,. For studies in which heart rate significantly changed, multiplying PWRmax/EDV2 by cardiac cycle length (seconds) should help normalize for
pure rate effects. These studies were conducted in
autonomically blocked animals to prevent reflex activation from interfering with the interpretation of
load or contractility dependency relations. Reflexes
that stimulate (or lower) the inotropic state of the
heart would be expected to alter PWRma/EDV 2, or
any contractile index, for that matter. It is generally
impossible to separate out this factor in an integrated
system unless reflexes are expressly blocked. This
should be remembered when studies are performed
in intact animals or a clinical setting.
The conclusions presented here for both experimental and theoretical model data depend on VO, the
volume at zero chamber pressure, being relatively
small compared with EDV (see "Appendix 1"). In
conditions in which VO may increase, such as with
chronically dilated hearts with chamber remodeling,
PWRmaX/EDV 2 may not be as load insensitive. It is in
*
*..--
0
z
1
^
^
..
V._ ",.
0.0
|
,
0.5
1.0
1.5
2.0
2.5
NORMALIZED CHARACTERISTIC IMPEDANCE
FIGURE 8. Plots of computer estimation of preload (upper
panel), peripheral resistance (middle panel), and characteristic impedance (lower panel) influence on maximal ventricular power (PWRm,X) and PWRma/end-diastolic volume
squared (EDV)2. The simulation used a time-varying
elastance heart model (Ees, 6.0 mm Hg/ml; V0 =0 ml) coupled
to a three-element windkessel vascular model [baseline peripheral resistance (Ra=4.0 mm Hg/ml sec-1), characteristic
impedance (IZcI =0.2 mm Hg/ml * sec-'), and compliance
(Ca,=1.4 ml/mm Hg)] at a heart rate of 100 beatslmin and
baseline EDVof 45 ml. These modelparameters were derived
from and typical of the experimental data. To compare model
with group experimental results, model data were also normalized as in Figures 4 and 5. The modelpredicted a dependence
of PWRm,x on EDV (upper panel) and a minimal effect of
EDV on PWRX.JEDV2 that were very similar to the actual
experimental data (compare with Figure 4). In response to
either 50% reductions or 100% increases in either Ra or r IZlI
(middle and lower panels), PWR,,,, and PWRma,/ changed
relatively little (latter response indentical to PWR, due to
constant EDV and normalization). Of these two afterload
parameters, IZcI change had a slightly larger effect, which is
consistent with the fact that PWR, occurs early in ejection.
Kass and Beyar LV Contractility and Ventricular Power Index
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
these instances, as noted above, that additional consideration of mass or wall stress would probably be
needed.
All prior studies of loading influences on power or
PWRmax examined steady-state data at one or two
loading states. In this regard, the present study is
unique by assessing load dependence on a beat-by-beat
basis over a broad range of loads within each heart and
among hearts. It is always possible that a component of
the observed response stems from the specific type of
load intervention used. It is impractical to test all
possible load maneuvers; however, the similarity between our experimental and model results (the latter
representing idealized load changes) suggests this was
not a significant limitation. Although the influence of
right heart loading itself (via right ventricle-left ventricle interaction) was not directly tested, it should be
noted that left atrial hemorrhage rapidly leads to
lowered right heart filling pressures, so interaction
effects were not eliminated.
Clinical Implications
Recent advances in noninvasive recording technology have renewed interest in power indexes. Doppler
echocardiography and nuclear ventriculography can
each provide reasonable estimates of aortic outflow
and volumes.26-28 Central aortic pressure has been
estimated using tonometers29,30 applied to either the
carotid or subclavian pulse and calibrated with peripheral cuff pressures.
A more recent and quite promising pressure-recording technique uses an automated cuff device.31
By appropriate recording of cuff pressure and time to
the onset of flow at the cuff (by ultrasound sensor)
gated off the electrocardiogram, the calibrated ascending portion of the central aortic pressure waveform can be determined. The pressures obtained by
this device compare favorably with invasive micromanometer measurements.31 Because power occurs
early in ejection, it is only the ascending aortic
waveform that is required to determine maximal
power. Power estimation using this device and simultaneous nuclear gated scintigraphy was recently reported in a human exercise study of normal and
postinfarction patients.32 Certainly, a practical advantage of PWRmna/EDV2 lies in its assessment at
steady state rather than requiring loading interventions as for ESPVR and related measures.
Our data should encourage future studies testing
the ratio of PWRmax to EDV 2 for noninvasive clinical
systolic function assessment. Although absolute values may be influenced by complex adaptive changes
that often accompany chronic disease states, this
index should be useful as an adjunctive measurement
for assessing relatively acute drug responses and for
exercise testing where relative changes at preset
levels of exertion are important. Future clinical studies are needed to define the ultimate clinical usefulness of this index.
1707
Appendix 1
Modeling the heart by a time-varying elastance, we
obtain:
P(t)=E(t) * [V(t)-Vo]
(7)
Substituting into Equation 2 for power, we obtain:
PWR(t) =P(t) * dV/dt
=E(t) . [V(t)-VO] . dV/dt
(8)
Because PWRmaX [=PWR(tmax)] occurs early into
ejection, we can approximate V(t) at tmax by EDV. If
V0 is small relative to EDV, Equation 8 becomes:
PWR(t)aE(t) . EDV * dV/dt
(9)
PWRmax also occurs very near dV/dtmax (see Figures 3
and 6), and dV/dtma directly varies with preload
volume at a constant heart rate (i.e., dV/dtmaxadV/
dtmax). Thus,
PWR(t)aE(t). EDV AEDV
(10)
aE(t) . EDV2
PWR/EDV2 will be proportional to chamber
elastance; thus, it is not surprising that there is a
correspondence between PWRma, and Ees.
Appendix 2
Maximal power occurs just after flow deceleration.
This can be shown as follows:
(11)
PWR(t)=P(t) . dV/dt=P(t)* F(t)
PWRma, occurs when d[PWR(t)]/dt=0. Thus:
(12)
dP/dt * F(t)+P(t) dF/dt=0
Early in ejection (until Pm.a), dP/dt, P(t), and F(t) are
all greater than zero. Thus, PWRm. occurs when
dF/dt is less than 0 or when flow is starting to
decelerate. This is important because systolic pressure wave reflections generally occur after this time
and thus would not influence PWRmax.
Acknowledgments
The authors gratefully thank Drs. Alon Marmor
and Tali Sharir for stimulating our interest, Dr. Paolo
Marino and Richard Tunin for assisting in the study,
and Dr. Daniel Burkhoff for providing the cardiovascular computer simulation.
References
1. Suga H, Sagawa K, Shoukas AA: Load independence of the
instantaneous pressure-volume ratio of the canine left ventricle and effects of epinephrine and heart rate on the ratio. Circ
Res 1973;32:314-322
2. Little WC, Cheng CP, Mumma M, Igarashi Y, VintenJohansen J, Johnston WE: Comparison of measures of left
ventricular contractile performance derived from pressurevolume loops in conscious dogs. Circulation 1989;80:1378-1387
3. Misbach GA, Glantz SA: Changes in the diastolic pressurediameter relation after ventricular function curve. Am JPhysiol
1979;237:H644-H648
4. Glower DD, Spratt JA, Snow ND, Kabas JS, Davis JW, Olsen
CO, Tyson GS, Sabiston DC, Rankin JS: Linearity of the
1708
5.
6.
7.
8.
9.
10.
11.
12.
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
13.
14.
15.
16.
17.
18.
19.
Circulation Vol 84, No 4 October 1991
Frank-Starling relationship in the intact heart: The concept of
preload recruitable stroke work. Circulation 1985;71 :994-1009
Little WC: The left ventricular dP/dtm:-end-diastolic volume
relation in closed-chest dogs. Circ Res 1985;56:808-815
Mirsky I, Tajimi T, Peterson KL: The development of the
entire end-systolic pressure-volume and ejection-fractionafterload relations: A new concept of systolic myocardial
stiffness. Circulation 1987;76:343
Mirsky 1, Aoyagi T, Crocker VM, Fujii AM: Preload dependence of fiber shortening rate in conscious dogs with left
ventricular hypertrophy. JAm Coll Cardiol 1990;15:890-899
Snell RE, Luchsinger PC: Determination of the external work
and power of the left ventricle in intact man. Am Heart J
1965;69:529-537
Russell RO, Porter CM, Frimer M, Dodge HT: Left ventricular power in man. Am Heart J 1971;81:799-808
Stein PD, Sabbah HN: Rate of change of ventricular power:
An indicator of ventricular performance during ejection. Am
Heart J 1976;91:219-227
Stein PD, Sabbah HN: Ventricular performance during ejection: Studies in patients of the rate of change of ventricular
power. Am Heart J 1976;91:599-606
Unterberg RH, Korfer R, Politz B, Schmiel K, Spiller P:
Assessment of left ventricular function by a power index: An
intra-operative study. Basic Res Cardiol 1989;79:423-431
Baan J, Van der Velde E, De Bruin H, Smeenk G, Keeps J,
Van Dijk A, Temmerman D, Senden J, Buis B: Continuous
measurement of left ventricular volume in animals and man by
conductance catheter. Circulation 1984;70:812-823
Kass DA, Yamazaki T, Burkhoff D, Maughan WL, Sagawa K:
Determination of left ventricular end-systolic pressure-volume
relationships by the conductance (volume) catheter technique.
Circulation 1986;73:586-595
Lankford EB, Kass DA, Maughan WL, Shoukas AA: Does
volume catheter parallel conductance vary during a cardiac
cycle? Am J Physiol 1990;258:H1933-H1942
Burkhoff D, Van der Velde E, Kass DA, Baan J, Maughan
WL, Sagawa K: Accuracy of volume measurement by conductance catheter in isolated, ejecting canine hearts. Circulation
1985;72:440-447
Applegate RJ, Chang CP, Little WC: Simultaneous conductance catheter and dimension assessment of left ventricle
volume in the intact animal. Circulation 1990;81:638-648
Sunagawa K, Maughan WL, Burkhoff D, Sagawa K: Left
ventricular interaction with arterial load studied in isolated
canine ventricle. Am J Physiol 1983;245:H773-H780
Sunagawa K, Maughan WL, Sagawa K: Optimal arterial
resistance for the maximal stroke work studied in isolated
canine left ventricle. Circ Res 1985;56:586-595
20. Kass DA, Beyar R, Lankford E, Heard M, Maughan WL,
Sagawa K: Influence of contractile state on curvilinearity of in
situ end-systolic pressure-volume relations. Circulation 1989;
79:167-178
21. Glantz SA, Slinker BK: Primer of Applied Regression and
Analyses of Variance. New York, McGraw-Hill Book Co, 1990,
pp 381-391
22. Alexander J, Burkhoff D, Schipke J, Sagawa K: Influence of
mean pressure on aortic impedance and reflections in the
systemic arterial system. Am J Physiol 1989;257(Heart Circ
Physiol 26):H969-H978
23. Sagawa K, Kass DA, Sugiura S, Burkhoff D, Alexander J:
Contractility and pump function of in vivo left ventricle and its
coupling with arterial load: Testing the assumptions, in Hori
M, Suga H, Baan J, Yellin E (eds): Cardiac Mechanics and
Function in the Normal and Diseased Heart. New York/Tokyo,
Springer-Verlag, pp 81-90
24. Gundel W, Cherry G, Rajagopalan G, Tan LB, Lee G, Schultz
D: Aortic input impedance in man: Acute response to vasodilator drugs. Circulation 1981;63:1305-1314
25. Merrillon JP, Fontenier GJ, Lerallut JF, Jaffrin MY, Motte
CA, Genain GP, Gourgon RR: Aortic input impedance in
normal man and arterial hypertension: Its modification during
changes in aortic pressure. Cardiovasc Res 1982;16:646-656
26. Calafiore P, Stewart WT: Doppler echocardiographic quantitation of volumetric flow rate. Cardiol Clin (Rev) 1990;8:
191-202
27. Al-Khawaja IM, Lahiri A, Raftery EB: Measurement of
absolute left ventricular volume by radionuclide angiography:
A technical review. Nucl Med Commun 1988;9:494-504
28. Stein PD, Sabbah NH, Albert DE, Snyder JE: Continuouswave Doppler for the noninvasive evaluation of aortic blood
velocity and rate of change of velocity: Evaluation in dogs. Med
Instrum 1987;21:177-182
29. Kelly R, Hayward C, Avolio A, O'Rourke M: Noninvasive
determination of age-related changes in the human arterial
pulse. Circulation 1989;80:1652-1659
30. Kelly R, Hayward C, Ganis J, Daley J, Avolio A, O'Rourke M:
Non-invasive registration of the arterial pressure pulse waveform using high-fidelity applanation tonometry. J Vasc Med
Biol 1989;3:142-149
31. Marmor AJ, Blendheim DS, Gozlan E, Navo E, Front D:
Method for noninvasive measurement of central aortic systolic
pressure. Clin Cardiol 1987;10:215-221
32. Marmor A, Sharir T, Shlomo B, Beyar R, Frenkel A, Front D:
Radionuclide ventriculography and central aortic pressure
change in noninvasive assessment of myocardial performance.
J Nucl Med 1989;30:1657-1665
KEY WoRDs * ventricular function * hemodynamics * contractility
* ventricular volume * aortic flow
Evaluation of contractile state by maximal ventricular power divided by the square of
end-diastolic volume.
D A Kass and R Beyar
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
Circulation. 1991;84:1698-1708
doi: 10.1161/01.CIR.84.4.1698
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1991 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on
the World Wide Web at:
http://circ.ahajournals.org/content/84/4/1698
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally
published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further
information about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/