Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
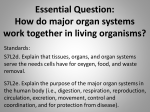
Urachaladenocarcinoma with multiple gastrointestinal fistulization SaedM Jaber, MD., Moatamn MSadoun, MD., Hamzah K Alshaikh, MD., Mohsen M Alsaid, MD, FRCS. All Authors from Department of Surgery, King Fahd Medical Military Complex, Dhahran, Saudi Arabia, PO Box 946, Postal code 31932, Telephone 8405142, Mobile 0504231486 Abstract The urachus is the embryological remnant of the urogenital sinus and allantosis. In two-thirds of cases, involution occurs before birth and the urachus exists as a median umbilical ligament. This report describes a rare case of a large urachus associated with fistulization to the cecum and sigmoid colon in addition to the presence of adenocarcinoma of the urachus. Keywords: urachus; urogenital sinus; allantosis; fistulization; adenocarcinoma. Introduction The urachus is a vestigial structure that attaches the bladder to the allantosis during early embryonic evolution (1). Postmortem autopsy research revealed that in one-third of cases the urachus persists at the dome of the urinary bladder (2). One of the consequences of this congenital abnormality is adenocarcinoma with an incidence of 0.17% - 0.34% of urinary bladder cancers (3, 4). Another depressive complication is chronic inflammation of the urachus and urinary bladder in the form of cystitis cystica, as we found that not only adenocarcinoma of the urachus is a rare entity but also has ability of multiple gastrointestinal fistulization. Case presentation A sixty-year-old male presented with history of burning micturation and voiding small flakes of particles of one month’s duration. He had a history of lower abdominal swelling of one year’s duration which was progressively increasing in size. Examination of the abdomen showed the presence of a hypogastric mass measuring 14x10cm with no evidence of lymphoadenopathy (figure 1). Figure 1: A large hypogastric mass The patient had a cystoscopy; a biopsy from multiple sites showed the presence of cystitis cystica. His alpha fetoprotein was 2.08, his carcinoembryonic antigen was 6.37. Urinalysis and urine culture showed no evidence of infection. Cytology of urine showed an absence of malignant cells. An abdominal pelvic computed tomography scan (figure 2) revealed an irregular-shaped large mass lesion resting on the dome of the urinary bladder and extending upwards on the midline. It measured 13x8x8 cm in craniocaudal, transverse, and AP diameters, respectively. It showed peripheral thick contrast enhancement involving the urinary bladder dome and anterior urinary bladder wall, with pockets of air inside. Most of the central parts of the lesion did not enhance, which could be attributed to central necrosis, hemorrhage, or fluid content. Small bowel loops were matted and adherent to the lesion. Fig 2: Abdominal pelvic CT scan(reviewed with radiologist KhaledSaleh MD) revealed an irregular-shaped large mass lesion resting on the dome of the urinary bladder and extending up to the umbilicus with central gas pockets Exploratory laparotomy was performed with introperative finding of three internal fistulization of the mass into the sigmoid colon and the ascending colon. Subsequently we performed an en bloc resection of the mass with umbilictomypartial cystectomy, limited right hemicolectomy, andsigmoidectomy. Gross examination of the mass revealed a solid mass with two clear fistula tracts as described previously (figure 3). Figure 3: A solid mass with fistula tracts. The blue arrow shows the cecum attached to the mass. The orange arrow shows the sigmoid colon attached to the urachus From the pathological standpoint, the fistula was due to malignancy invading the abovementioned organs. The fistula tract lining consisted of well-differentiated mucin-producing adenocarcinoma. Severe ischemic change of tumor with hemorrhage, fistula formation, and granulation tissue were part of the observation in all of the tracts. (figure 4) Figure 4: Slide show well-differentiated mucin-producing adenocarcinoma Discussion The intra-embryonic portion of the allantosis forms a connection from the apex of the urinary bladder to the umbilicus, later called the urachus or the median umbilical ligament, located in the extraperitoneal space within the Retzius space (1). The Retzius space is located between the transversalis fascia and the infraumbilical parietal peritoneum, measuring 2-15cm in length. Postmortem autopsy research revealed that in one-third of cases the urachus persisted at the dome of the urinary bladder (2). The normal epithelium lining the urachus is transitional epithelium. Surprisingly, most cancers developing from the urachus are adenocarcinoma, making up about 90% of thehistopathological findings (3). It is suggested that columnar metaplasia of the normal lining occurs first and subsequently undergoes malignant transformation (4). Another theory claims that adenocarcinoma arises from embryonic rests within islands of mucus containing hindgut epithelium that persist within the urachus. Two staging systems exist. The old staging system is called the Sheldon system (5). Which stage the tumor according to invasion to the surrounding structures and the new system that is based on the Henly system and is called the Mayo system (5).Which stage the tumor according to layers invasion and regional lymph node spread. Previously it was thought that cystitis cystica in an urachus-affected patient could be premalignant, as described by Nesbit (1956) and Kittredge (6, 7). Recently, there is evidence that there is no relation and cystitis cystica is not a premalignant condition (8). The prognosis is often poor due to late presentation, which is associated with local invasion and distant metastasis. The five-year survival rate is 49% as described by the Ashley group’s experience at the Mayo Clinic (9), but in Japan the five-year survival is only 6%. The mainstay management of urachus carcinoma is surgical management, which requires complete resection with umbilictomy to achieve free margins to improve the survival rate (10). Here, we describe a rare case of urachalmucineous adenocarcinoma with fistulization of the urachus adenocarcinoma into the cecum , terminal ileum, and the sigmoid colon with evidence of malignancy of the tracts in the histopathology slides as seen in figure 4. Conclusion Although urachal adenocarcinoma has now become a well-recognized malignancy, its origin and pathophysiology remain unknown. Modern therapeutic regimens have offered minimal benefit, especially when the affected area is unresectable.Urachal adenocarcinoma demonestated that this tumor has the capability to fistulize into adjacent organs.Such a disease best treated with radical surgical resection to improve the outcome and reduce the recurrence. Cited References 1 Begg RC. The urachus: its anatomy, histology, and development. J Anat. 1930; 64: 170end page. 2 Schubert GE, Pavkovic MB, Bethke-Bedurttig BA. Tubular urachal remnants in adult bladders.J Urol. 1981; 127: 40-42. 3 Begg RC. The colloid adenocarcinoma of the bladder vault arising from the epithelium of the urachal canal. Br J Surg. 1931; 18: 422-66. 4 Sheldon CA, Clayman RV, Gonzalez R, Williams RD, Fraley EE. Malignant urachal lesions. J Urol. 1984; 131: 1-8. 5 page. Paras FA Jr., Maclennan GT. Urachal adenocarcinoma. J Urol. 2008; 180(2): 720-end 6 Nesbit R M. Title of article. J Urol. 1956; 75: 433-end page. 7 Kittredge WE, Collett AJ, Morgan C. Title of article. J Urol. 1964; 91: 145-end page. 8 Smith AK, Hansel DE, Jones JS. Role of cystitis cystic etglandularis and intestinal metaplasia in development of bladder carcinoma. Urology. 2008 May; 71(5): 915-8. 9 Ashley RA, Inman BA, Sebo TJ, Leibovich BC, Blute ML, Kwon ED, Zincke H. Urachal carcinoma: clinicopathologic features and long-term outcomes of an aggressive malignancy. Cancer.2006; 107: 712-20. 10 Ravi R, Shrivastava BR, Chadrasekhar GM, et al .Adenocarcinoma of the urachus.J SurgOncol.1992; 50: 201-3. Acknowledgment All authors have no conflicting interests, and are not supported/funded by any Drug Company.