Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
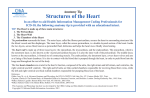
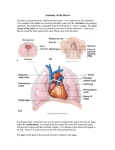
PATHOPHYSIOLOGY AND NATURAL HISTORY MYOCARDIAL ISCHEMIA Myocardial oxygen consumption, oxygen supply/demand heterogeneity, and microvascular patency in regionally stunned myocardium LLOYD D. STAHL, M.D.,* HARVEY R. WEISS, PH.D., AND LEWIS C. BECKER, M.D. Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 ABSTRACT Although oxygen consumption closely parallels mechanical work in the normal heart, previous studies have found that stunned myocardium may have normal or even increased oxygen consumption despite depressed function. In this study we used microspectrophotometry to measure the oxygen saturations within arteries and veins of less than 100 ,um diameter in quick-frozen biopsy samples from normal and regionally stunned myocardium of 10 open-chest anesthetized dogs. Regional myocardial blood flow, measured by radioactive microspheres, was similar in stunned and normal regions, as was mean arteriolar oxygen saturation. However, mean venous oxygen saturation was lower in the stunned region (epicardium 38.0% vs 43.8%, p < .02; endocardium 36.2% vs 39.5%, p = .12), indicating increased oxygen extraction and consumption, despite a marked reduction in mean systolic segmental shortening from 14.4% to 0.5%. In addition, there was greater vein-to-vein heterogeneity of oxygen saturation in the stunned region, with an excess of veins having low saturations (statistically significant in epicardium, nonsignificant trend in endocardium). Microvascular injection studies with Microfil or drafting ink revealed filling of over 95% of arterioles and 85% of capillaries in the stunned region, similar to the findings in the normal region. Our results are consistent with an inefficient transfer of energy into myocyte contraction or an increased use of energy for noncontractile activities in stunned myocardium. In addition, the finding of increased heterogeneity of oxygen extraction suggests that the injury to stunned myocardium may not be uniform to all contractile elements, but instead may be focally and irregularly distributed. Circulation 77, No. 4, 865-872, 1988. REPERFUSION after a brief episode of mycardial ischemia may result in prolonged dysfunction without necrosis, a phenomenon now known as "myocardial stunning."''3 Since myocardial oxygen consumption closely parallels energy production and mechanical work in the normal heart 4-6 one would anticipate that stunned myocardium should exhibit reduced oxygen consumption. Although several abstracts have appeared describing reduced,7 8 normal,9' 10 or even increased1' oxygen consumption in stunned myocardium, the only published study bearing on this issue From the Division of Cardiology, Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, and Department of Physiology and Biophysics, Heart and Brain Circulation Laboratory, UMDNJ-Robert Wood Johnson Medical School, Piscataway, NJ. Supported by a Research Fellowship fronm the American Heart Association, Maryland Affiliate, and by U.S. Public Health Service grants 17655-12 (SCOR in Ischemic Heart Disease) and 26919 from The National Heart, Lung, and Blood Institute. Address for correspondence: Lewis C. Becker, M.D., Johns Hopkins University School of Medicine, 600 N. Wolfe St., Halsted 500, Baltimore, MD 21205. Received Aug. 17, 1987; revision accepted Dec. 30, 1987. *Present address: Menorah Medical Center, 4949 Rockhill Rd., Kansas City, MO 64110. Vol. 77, No. 4, April 1988 indicates that postischemic myocardial oxygen utilization may be increased above normal.'2 Following reperfusion after 2 hr of hypothermic cardioplegic ischemia, canine hearts demonstrated normal pressurevolume curves, but a 40% increase in oxygen utilization at matched levels of developed pressure.'2 Although the cause of myocardial stunning is unknown, it has been suggested that calcium overload may represent a major factor.13 Intracellular sodium, which accumul4tes during ischemia, may rapidly exchange for calcium during reperfusion, as acidosis (an inhibitor of sodium-calcium exchange) resolves. Hoerter et al. 14 have shown that increased myocellular calcium content, induced by sodium-calcium exchange via manipulations of perfusate composition, can result in reduced systolic function, while myocardial oxygen consumption is paradoxically increased. The recent finding by Kusuoka et al.13 that reperfusion with low calcium-containing perfusate eliminates myocardial stunning provides further support for the calcium overload hypothesis. Inappropriately high oxygen consumption, if present, could reflect an increased utili865 STAHL et al. Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 zation of energy for movement of calcium in stunned myocardium. Virtually nothing is known about the homogeneity of abnormalities within stunned myocardium. It is unclear whether the dysfunction of a stunned myocardial segment represents uniform depression of all contractile elements, or patchy, focally distributed injury. Information on this issue is critical for an understanding of the pathophysiology and pathogenesis of stunned myocardium. In this study we used the technique of microspectrophotometry to compare oxygen extraction and consumption in stunned and normal myocardium by determining the oxygen saturation of blood in small arteries and veins less than 100 ,um in diameter in quick-frozen myocardial biopsy samples taken from regionally stunned dog hearts. The microscopic nature of this technique allowed us to measure the vein-to-vein uniformity of oxygen extraction within the stunned and normal myocardial segments. In addition, we assessed the patency of the microvasculature in stunned and normal myocardium by microscopic analysis of hearts infused in situ with Microfil or drafting ink. Methods Animal preparation. Fifteen mongrel dogs of either sex (20 to 25 kg) were anesthetized with intravenous sodium thiamylal (12.5 mg/kg) and intramuscular cx-chloralose (100 mg/kg) in urethane, intubated and ventilated with room air at a constant volume with a piston respirator. After a left thoracotomy, the lungs were retracted and the heart was exposed through a peri- cardiotomy. Pairs of 5 MHz cylindrical piezoelectric crystals (0.06 inches outside diameter, 0.06 inches in length, 0.015 inches thick; Vernitron, Columbus, OH) were implanted in the myocardium served by the anterior descending coronary artery and the anterolateral basal region within the circumflex artery territory. The crystals were implanted in the midwall of the left ventricle, 10 to 15 mm apart, and were oriented parallel to the minor axis. Segmental lengths were measured with a pulse transit sonomicrometer (model Sono-1-XB, James Davis Consultants). Left ventricular pressure, and its first derivative with respect to time, left ventricular dP/dt, were measured with a catheter-tipped pressure transducer (Millar) that was inserted through an implanted silicone rubber left atrial catheter and advanced across the mitral valve. Aortic pressure was measured by inserting a catheter-tipped pressure transducer (Millar) into the aortic root from the right carotid artery. Catheters were placed in the descending aorta for withdrawal of microsphere reference samples, the left atrium for microsphere injections, and the femoral vein for infusion of fluids. Aortic and left ventricular pressures and regional segmental lengths were recorded continuously on a direct-writing recorder (Gould Brush 200). Experimental protocol. A pneumatic occluder was placed around the left anterior descending coronary artery just distal to the first diagonal branch. Stunning was produced by ten 5 min occlusions alternating with 10 min reflow periods, followed by a 90 min recovery period. Blood flow to stunned and normal myocardium was determined by radioactive microspheres (15 ,im diameter, New 866 England Nuclear Co.) labeled with 141Ce or 13Sn. Three to five million microspheres were injected into the left atrium after a 3 min mechanical agitation, while reference arterial samples were withdrawn at a constant rate of 2.16 ml/min by a calibrated pump. Blood flow was calculated from the radioactivity in the tissue and reference blood samples determined in a well-type gamma scintillation counter (Packard model 5986) by standard methods after correction for overlap of the energy peaks. In each dog, flows to stunned and normal zones represented measurements in single tissue blocks weighing 1 to 3 g, divided into endocardial and epicardial halves. Flows were measured at baseline and 90 min after the last ischemic episode. Hemodynamic and ultrasonic crystal measurements were made at end-expiration during the baseline state and 90 min after the final occlusion. In the first group of 10 dogs, after the stunning protocol, 3 to 5 g transmural biopsy samples were taken with use of a scalpel from the area of the stunned and normal regions encompassed by the sonomicrometer crystal pairs and were immersed immediately in liquid nitrogen. The time from initiation of the biopsy to immersion in liquid nitrogen was less than 10 sec in all cases. The samples were coded and stored in liquid nitrogen for future blinded analysis. The animals were then killed by intra-atrial injection of potassium chloride. The hearts were cut into five to six short-axis slices from apex to base, each of which was incubated at 370 C in triphenyltetrazolium chloride for 20 min and photographed in color. After this the site of each crystal pair was excised, weighed, and counted for radioactivity for measurement of blood flow. The fresh tissue and photographs were inspected to identify unstained areas that represented myocardial necrosis. A second group of five dogs underwent the identical instrumentation and repetitive coronary occlusion protocol. Ninety minutes after stunning was produced the sonomicrometer crystal pairs were removed and their locations were marked by loosely tied epicardial purse-string sutures. A 1/4 inch Teflon catheter was inserted through the left subclavian artery and advanced into the aortic root just above the aortic valve. The main pulmonary artery was ligated and the right atrium was vented to a reservoir. After approximately 3 to 5 sec, the ascending aorta was ligated proximal to the great vessels. In three dogs 50 ml of heparinized normal saline followed by 50 ml of Microfil silicone rubber compound (MV-122 Yellow, Canton Biomedical Products, Inc., Boulder, CO) was infused into the aortic root under 120 mm Hg constant pressure. In two other dogs, 8000 units of intravenous heparin was given before ligation of pulmonary artery. After ligation of the ascending aorta, 50 ml of heparinized normal saline was infused into the aortic root followed by 300 ml of black drafting ink (Pelikan, Hannover, West Germany) at a pressure of 120 mm Hg. All hearts continued to beat through the injection period. The hearts were excised below the atrioventricular ring, frozen immediately in liquid nitrogen, and then stored at 700 C for future analysis. Analysis of function. Signals from the ultrasonic crystals, left ventricular and aortic pressure, and left ventricular dP/dt were routed to a microcomputer (North-Star Horizon) at selected times during the experiment, digitized at 150 Hz by a Tecmar 12-bit analog-to-digital converter, and recorded on floppy disk for later computer analysis. The end-systolic segment length was measured 20 msec before peak negative left ventricular dP/dt15; end-diastolic length was measured just before the onset of positive left ventricular dP/dt. Percent systolic segmental shortening was calculated as segmental shortening (end-diastolic minus end-systolic length) divided by end-diastolic length times 100, and represented the average of 5 heartbeats. Analysis of oxygen extractions. The quick-frozen biopsy samples from the stunned and normal regions of the dogs in the first group were prepared as follows. Thirty micrometer thick CIRCULATION PATHOPHYSIOLOGY AND NATURAL HISTORY-MYOCARDIAL ISCHEMIA Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 frozen tissue sections were cut on a Slee automated microtomecryostat set at - 350 C in a nitrogen atmosphere. Each section was then transferred to a precooled slide, covered with degassed silicone oil, and rapidly transferred to the microspectrophotometer cold stage flushed with nitrogen gas. Arteries and veins less than 100 Km in diameter were located and absorbances at 560, 523, 506 nm were obtained to give oxygen saturation of the blood contained within the vessels. 16 Only vessels seen in transverse section were studied, so that the light path was only through blood. Between seven and 10 arterioles and seven to 10 venules in the endocardial and epicardial segments of the stunned and normal regions were analyzed for each dog. Regional oxygen extraction (ml 02/100 ml blood) was calculated as the difference between mean arteriolar and venous oxygen saturation, multiplied by the arterial hemoglobin concentration, times the maximal oxygen-combining capacity of 1.36 ml O2/g hemoglobin. Hemoglobin concentration was determined with a Fisher hemophotometer (Fisher Scientific Co., Pittsburgh) from blood samples obtained at the end of the study. The oxygen consumption for each segment of interest was calculated as the product of oxygen extraction and regional blood flow. Microscopic evaluation of the microvasculature. To identify perfused microvessels (both Microfil and drafting ink), samples were prepared as follows: 2 pum thick sections were cut from the hearts on a Slee automated microtome-cryostat set at - 350 C. Eight to twenty sections from the endocardial and epicardial segments of both the normal and stunned regions were cut for each animal. Each section was at least 150 to 200 pum from the previous one. As described previously,17 19 the slides were photographed through a Zeiss microscope equipped for automated photography. A 40 x planapochromat objective was used to photograph the capillary fields and a 10 x objective was used to photograph the fields used for observation of arterioles. The slides were then stained for alkaline phosphatase, as described previously.'9 Briefly, they were fixed in a sucrose-formalin buffer for 1 min, washed twice in distilled water, and then placed in an incubation mixture for 30 min at 370 C. The incubation mixture consisted of 3.8 g/liter of Fast blue RR, 0.5 g/liter of cL-napthylphosphate, 3.8 g/liter of sodium metaborate, and 1.7 g/liter of magnesium sulfate. The slides were postfixed and dried. Various stereologic determinations were made, counting each field twice, once for the total and once for the perfused microvasculature. The system used was a Dapple image analyzing device. We placed the slides that were stained for alkaline phosphatase under a microscope and the image analyzer evaluated the field for total morphometric indexes of microvascularity. The image was obtained from a Panasonic television camera attached to the microscope and digitized with the Dapple image analyzer. The number of microvessels per square millimeter was estimated from the number per unit test area. The diameter of the microvessels was determined by measurement of the minimum diameter of any vessel cut in transverse sections such that the maximum diameter was no more than 1.5 times the minimum. After the total microvasculature was studied, the perfused portion was obtained by analysis of photographs of the field for the presence of either microfil or the carbon particles of the drafting ink. Data analysis. Data are presented as the means + SD. Comparisons between the means were by paired t test. Comparisons of proportions in the stunned and normal regions were performed by chi-square analysis. Results Hemodynamic changes after repeated brief coronary occlusions. Comparing baseline and 90 min after repeated brief coronary occlusions, there were no sigVol. 77, No. 4, April 1988 nificant differences in heart rate (128 ± 20 vs 133 + 26 beats/min), peak left ventricular pressure (124 + 18 vs 131 ± 13 mm Hg), or mean aortic pressure (100 ± 13 vs 105 ± 10 mm Hg). The effects of repeated coronary occlusions on regional function. Systolic segmental shortening in the left anterior descending region decreased from 14.4 ± 3.3% at baseline to 0.4 + 4.6% after the repeated 5 min coronary occlusions (p <.001; table 1). The end-diastolic segmental length increased from 12.2 ± 2.1 mm at baseline to 14.6 ± 2.9 mm after stunning (p < .05). The control region showed no change in systolic segmental shortening (11.0±2.2% at baseline vs 10.7± 1.7% after repeated occlusions) or end-diastolic segment length (11.7 ± 1.9 vs 11.5 ± 2.1 mm). Myocardial necrosis. No areas of necrosis were observed on visual inspection of the triphenyl tetrazolium chloride-stained left ventricular slices from any of the 15 animals. Regional arterial and venous oxygen saturations and oxy- gen extraction. The mean arterial and venous oxygen saturations in the stunned and control regions are shown in table 2. One hundred fifty-eight arterioles were sampled from the control regions of the 10 dogs (79 in the endocardial region and 79 in the epicardial region). One hundred sixty-one arterioles were sampled from the biopsy specimens from the stunned region (79 in the endocardial region, 82 in the epicardial region). Values for mean arterial oxygen saturation were somewhat low, ranging from 83.4% to 85.7%, probably reflecting the fact that the dogs were ventilated with room air in the right lateral decubitus position. However, there were no significant differences in the mean arterial oxygen saturation or in the frequency distribution of the arterial saturations in the stunned and control regions. With respect to venous saturations, a significantly lower mean epicardial venous oxygen saturation was TABLE 1 Regional function and blood flow in stunned and control regions Systolic End-diastolic Endocardial Epicardial flow flow shortening length (%) (mm) (ml/g/min) (mlg/mi) Stunned region Baseline 90 mm after ischemia Control region Baseline 90 mm after ischemia 12.2±2.1 1.1±+0.2 1.2±0.2 14.6 ± 2.9B 1.0±0.1 1.3±0.2 11.0±2.2 11.7± 1.9 1.0±0.2 1.4±0.3 10.7±1.7 11.5±2.1 0.9±0.1 1.3±0.2 14.4±3.3 0.5 ±4.6A Ap < .001 compared with baseline value; Bp < .05 compared with baseline value. 867 STAHL et al. TABLE 2 Mean oxygen saturations, extraction, and consumption in stunned and control regions Stunned Arterial saturation (%) Venous saturation (%) 02 extraction (ml O2/100 ml blood) 02 consumption (ml]2/zmin/lOO g) Control Endo Epi Endo Epi 83.9 ± 3.4 36.2±14.6A 7.1 ± 1.OA 6.9± 1.5 85.7 ± 4.0 38.0± 13.9 7.1 0.9B 8.8+1.5B 83.4± 2.9 39.5+ 15.3 6.6± 1.0 6.4±1.9 85.4 ± 4.2 43.8±11.8 6.3 ± 0.8 7.8±1.3 ± Endo = endocardium; Epi = epicardium. Ap = .12 compared with control value. Bp < .05 compared with control value. Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 observed in the stunned region compared with control (38.0 ± 13.9% vs 43.8 ± 11.8%, p < .02, paired t test). There was also significantly greater vein-to-vein heterogeneity in the epicardium of the stunned region (figure 1). The proportion of veins with low oxygen saturations (<20%) was higher in the stunned than normal epicardium (14.9% vs 4.5%, p<.05). In the endocardium of the stunned region, the mean venous oxygen saturation was also lower (36.2 ± 14.6% in the stunned region vs 39.5 + 15.3% in the control region), although the difference did not reach statistical significance. The frequency distribution showed a tendency toward more veins with lower oxygen saturations in the stunned region (figure 2). Oxygen extraction was higher in the stunned region (7.1± 1.0 vs 6.6± 1.0 ml 02/100 ml blood in the endocardium and 7.1±9 vs 6.3±.8 ml 02/100 ml blood in the epicardium), although the difference reached statistical significance only in the epicardium (p<.05; figures 3 and 4, table 2). Regional myocardial oxygen consumption, calculated from regional oxygen extraction and blood flow, was about 10% higher in the stunned region (statistically significant in the epicardial segment; figures 3 and 4, table 2). The values for mean oxygen consumption (6.4 to 8.8 ml 02/min/100 g) were somewhat low, based on both the low arterial oxygen saturation and the low arterial hemoglobin concentration (average 11.25 mg/dl), but were within the range previously reported for open-chest dogs.20 There was no difference in the diameters of the vessels identified and used to obtain oxygen saturations in the stunned (mean arterial diameter 29.1 ± 21.2 gm with 87% of the vessels having a diameter of less than 60 ,um; mean venous diameter 25.2 ± 21.1 gm with 91% less than 60 ,um) and the control regions (mean arterial diameter 29.4 ± 24.6 ,um with 89% less than 60 ,im; mean venous diameter 24.7 + 19.3 ,um with 91% less than 60 ,im). Evaluation of microvascular patency. To determine whether the shift in venular oxygen saturations toward lower values in stunned myocardium was due to focal microvascular obstruction with heterogeneously impaired perfusion, hearts were injected in situ with either Microfil or drafting ink and evaluated microscopically (tables 3 and 4). In three hearts injected with Microfil IL -J J CL n LU :J TF 30 -4 E STUNNED U)2 40 T U) U) 40 0 NORMAL o LL 30 - 4 20 -J 0 NORMAL U STUNNED + z 0. 20 -j p< 05 LL a o -4 LL 10-_- L) O-1 z L) a: LU a. 0-J <20J 02 SATURATION (X) -30 30-40 40- 02 SATURATION t%) FIGURE 1. Histogram representing frequency of occurrence of different venous 02 saturations in the epicardial segments of stunned and normal regions. There were significantly more venules with oxygen saturations of less than 20% in the stunned region. 868 FIGURE 2. Histogram representing the frequency of occurrence of different venous 02 saturations in the endocardial segments of stunned and normal regions. There was a trend toward proportionally more venules with lower oxygen saturations in the stunned region, with 32% having saturations less than 30% in the stunned region vs 22% in the normal region (p= .15). CIRCULATION PATHOPHYSIOLOGY AND NATURAL HISTORY-MYOCARDIAL ISCHEMIA 10 7T 12 --F 10- z 8-]- z 0 o _ H cn - H-4 H ^ ±+ t* 6- L) E X LOZOoE0 -9 Z -O lll 0Cu ,WNf- 4- ZX X - f1 I1 6+ 4+ W a 2±_ 2+ *p<.05 0j z STUNNED *p<.05 E V S STUNNED NORMAL NORMAL FIGURE 3. The mean epicardial oxygen extraction and consumption for each dog, comparing results from the stunned and normal regions. The overall mean extraction and consumption was higher in the stunned than in the normal epicardial region. Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 to visualize arterioles, similar numbers of vessels were identified in stunned and control myocardium (epicardium, 0.92 vs 1.03 vessels/mm2; endocardium, 1.79 vs 2.10 vessels/mm2). Approximately twice as many vessels were observed in endocardial samples as in epicardial samples in both regions. The percent of vessels patent (i.e., filled with Microfil) was 96% or more and did not differ in stunned and control myocardium. In two hearts injected with drafting ink to visualize capillary filling, similar numbers of vessels were again identified in stunned and control specimens (epicardium, 3950 vs 4123 vessels/mm2; endocardium, 3411 vs 3455 vessels/mm2). Approximately 85% of vessels were patent (i.e., filled with carbon particles), without any difference between stunned and control regions. Discussion The major findings of this study were that despite reduced systolic function, regionally stunned myocardium exhibited higher mean oxygen extraction and consumption in the presence of normal mean myocardial blood flow. The stunned myocardium also demonstrated a significantly greater vein-to-vein heterogeneity of oxygen saturations, especially in the epicardial segment, with proportionately more venules demonstrating low oxygen saturations, suggesting that the stunned region contained microregions of either increased oxygen extraction or reduced flow. Microscopic examination of normal and stunned regions, however, revealed the microvasculature to be equally patent without evidence of occlusion or plugging. The microspectrophotometric analysis of arterial and 127 10 --- 8+ z 0 H z H 1-4 Cm qu cc0 H0 zo D 6 + Z O OE 4- 8- 6- 4- E Xn-i X 0 HO Z- 0 2 nl o - - T STUNNED 2±_ 0 NORMAL 1 i STUNNED FIGURE 4. The mean endocardial oxygen extraction and consumption for each dog and the overall normal regions. Vol. 77, No. 4, April 1988 NORMAL means for stunned and 869 STAHL et al. TABLE 3 Patency of arterioles in stunned and control regions as assessed by nilcrofil inJection Vessels identified Control Epicardium Endocardium Stunned Epicardium Endocardium Number Percent Vessel concentration patent patent (vessels/mm2 tissue) 128 282 122 271 95 96 1.03 2.10 122 236 119 234 98 99 0.92 1.79 Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 venous oxygen saturations has been detailed in previous publications and is accurate to approximately ±3%.21 The biopsy samples were frozen in liquid nitrogen within 10 sec of removal and stored in a liquid nitrogen container until microspectrophotometric measures were made. It has previously been shown that oxygen saturations in small arteries and veins, even those less than 50 ,u m in diameter, are not altered if the samples are frozen within 15 to 30 sec, and that the oxygen saturations are stable for weeks at this temperature.22' 23 All samples were coded and the microspectrophotometric analyses were performed without knowledge of location within the heart. The accuracy of our determination of regional oxygen consumption depends not only on the arterial and venous saturations, but also on the measurements of regional blood flow. We used mean blood flow values in endocardial and epicardial samples weighing about 1 g each. Based on the number of spheres injected, the estimated measurement error was less than 5%.24 In addition, the calculation of mean regional oxygen consumption from the individual venular and arteriolar oxygen saturation data involves the implicit assumption that perfusion is homogeneously distributed. If flow were diminished to microregions of high oxygen extraction and replaced by an equal increase in flow to regions of low extraction, mean oxygen extraction would actually be lower than the result obtained by TABLE 4 Patenty of capillaries in stunned and control regions as assessed by injection of drafting ink Total identifiedA PerfusedA % perfused 4123±423 3455 ±t416 3533±365 2894±+ 372 86 84 3950±382 3411±281 3306±310 2872±269 84 84 Control Epicardium Endocardium Stunned Epicardium Endocardium ANumber of vessels/mM2 tissue ± SD. 870 simple averaging of all of the individual extraction values. In previous studies,'16 25 the validity of the use of averaged microscopic values to obtain mean oxygen extraction has been established both for the heart and gracilis muscle by demonstrating comparability of the microspectrophotometric method and mean extraction obtained from measurements in large arteries and veins. Unfortunately, the distribution of perfusion cannot be examined directly, since methods are not available to measure flow with sufficiently high spatial resolution in the beating heart. Our finding that oxygen extraction and consumption were higher in stunned myocardium could theoretically be incorrect if the microvascular distribution of perfusion were grossly different in stunned and normal regions. However, the differences involved would have to be extreme. For example, we found a 13% increase in oxygen extraction and consumption in stunned epicardium. To lower this excess oxygen consumption to normal, flow would have to be absent from veins with the lowest saturation (< 20%) and replaced by flow to veins with the highest saturation (>50%; figure 1). Furthermore, if flow in normal myocardium were not completely homogeneous and also had a tendency to be distributed more to veins with higher saturations, the maldistribution in stunned myocardium would have to be even greater. Preliminary results from Dean et al.,9 who used regional coronary venous oxygen sampling, support the notion that oxygen consumption in stunned myocardium is at least equal to normal. There are a number of questions that arise from the results of this study. First, how does one interpret the finding in stunned myocardium of increased oxygen consumption and normal regional blood flow in the face of markedly depressed regional systolic shortening? Given what appears to be decreased mechanical work being performed by the stunned segment, the measurements of regional oxygen consumption are in marked excess of the metabolic demands attributable to muscle contraction. This suggests an impairment of aerobic metabolic efficiency, or a defect in the conversion of aerobicly derived metabolic energy into contractile work. Other investigators have recently reported normal or increased myocardial oxygen consumption in regionally9' 10 or globally8' 11 12 stunned models, consistent with an impairment of aerobic efficiency. Possible explanations for this phenomenon include uncoupling of oxidative phosphorylation, resulting in inefficient mitochondrial ATP production, or an increase in the cellular energy requirement for processes other than contraction. Mitochondrial uncoupling is CIRCULATION PATHOPHYSIOLOGY AND NATURAL HISTORY-MYOCARDIAL ISCHEMIA Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 unlikely, since Edoute et al.26 have shown that mitochondrial oxidative dysfunction occurs only after a relatively long ischemic exposure, well after the appearance of mitochondrial morphologic changes or postischemic mechanical dysfunction. An increase in noncontractile energy requirements seems a more likely possibility, perhaps related to an increase in ion pumping (i.e., extrusion of calcium from the mitochondria in calcium overloaded myocytes) or an increase in the activity of the calcium ATPase to maintain normal sequestration of calcium by the sarcoplasmic reticulum. Krause and Hess27 have demonstrated that after only 15 min of normothermic global ischemia in the dog, there is significant depression of sarcoplasmic reticulum function, with reduced calcium transport and depressed Ca + ++ Mg++ -ATPase activity. Importantly, the coupling between calcium transport and ATPase activity is also impaired, consistent with a need for greater utilization of ATP to move calcium into the sarcoplasmic reticulum. The finding of normal rather than depressed flow in stunned myocardium is of interest, since one might have anticipated that flow would autoregulate downward in concert with an assumed reduction in metabolic demands. However, our finding of increased oxygen extraction in stunned myocardium suggests that the metabolic demands are actually increased rather than decreased, although the energy produced is not translated into contractile work. Viewed in this light, normal levels of flow in stunned myocardium may actually represent an appropriate level of autoregulation. A second important question concerns the interpretation of our finding of greater heterogeneity of venous oxygen saturations in stunned myocardium, with proportionately more venules having very low oxygen saturations. In principle, this finding should reflect foci of increased oxygen extraction due to either focally impaired microvascular perfusion or microregions of increased oxygen consumption. In either case, our observation suggests that stunned myocardium may not be affected uniformly. Instead, dysfunction of an entire segment may be related to injury of focal microscopic regions. If stunned myocardium is caused by generation of oxygen free radicals upon reperfusion, as has been suggested by the beneficial effects of free radical scavengers, 28-30 our data suggest that radical formation may be patchy, possibly related to nonuniform generation within the microvasculature. Based on Engler and Covell's finding that leukocyte depletion results in an attenuation of myocardial stunning,31 a patchy distribution of leukocytes within the microvasculature may be Vol. 77, No. 4, April 1988 responsible for a heterogeneous pattern of free radical production and myocyte injury. The vascular injection studies were performed to gain further insight into the finding of a greater proportion of venules with very low oxygen saturations in stunned myocardium. Our results appear to exclude anatomic vascular obstruction at either the arteriolar or capillary levels as an important mechanism. Because the microfil or drafting ink was injected under physiological pressures in vivo while the heart was still beating, it is unlikely that the injection process per se caused a significant artifactual reopening of previously obstructed vessels. In addition, microvascular patency is supported by our previous finding of normal maximal flow reserve in stunned myocardium.32 Hori et al.33 demonstrated that during progressive occlusion of the microvasculature with microspheres, resting flow initially remained normal due to compensatory focal vasodilation, but the maximal vasodilating capacity of the bed fell progressively. Although anatomic obstructions were not identified, our methods were not designed to exclude functional heterogeneity of perfusion. Although the injections of drafting ink were made "semiphysiologically" and carbon particles were seen in nearly all capillaries, the actual numbers of carbon particles present in each vessel were not quantified. In addition, because the ink was injected over several minutes, even vessels with very slow flow should have been filled. In conclusion, our results provide new data concerning postischemic regionally stunned myocardium in the open-chest anesthetized dog. We found a significant increase in mean oxygen extraction and consumption despite an apparently marked decrease in contractile function. Although mean perfusion of the stunned myocardium was normal and the microvasculature was normally patent, microspectrophotometry revealed increased heterogeneity with an excess of very low venous oxygen saturations, implying either focally impaired perfusion or increased metabolic activity. These results suggest that stunned myocardium is injured in a nonuniform, patchy fashion, although the precise type of injury incurred and the mechanisms responsible remain to be determined. We gratefully acknowledge the assistance of the technicians in our research laboratories, Anthony F. DiPaula, Jr., Alexander (Skins) Wright, and Elizabeth Rodriguez, and of Christine G. Holzmueller in the preparation of this manuscript. References 1. Kloner RA, DeBoer LVW, Darsee JR, Ingwall JS, Braunwald E: Recovery from prolonged abnormalities of canine myocardium salvaged from ischemic necrosis by coronary reperfusion. Proc Natl Acad Sci USA 78: 7152, 1981 871 STAHL et al. Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 2. Braunwald E, Kloner RA: The stunned myocardium: prolonged, post-ischemic ventricular dysfunction. Circulation 66: 1146, 1982 3. Nicklas JM, Becker LC, Bulkley BH: Effects of repeated brief coronary occlusion on regional left ventricular function and dimension in dogs. Am J Cardiol 56: 473, 1985 4. Sarnoff SJ, Braunwald E, Welch GH Jr, Case RB, Strainsby WN, Macruz R: Hemodynamic determinants of oxygen consumption of the heart with special reference to the tension time index. Am J Physiol 192: 148, 1958 5. Braunwald E, Graham TP Jr, Covell JW, Sonenblick EH, Ross J Jr: Control of myocardial oxygen consumption: relative influence of contractile state and tension development. J Clin Invest 47: 375, 1968 6. Whalen WJ: The relation of work and oxygen consumption in isolated strips of cat and rat myocardium. J Physiol 157: 1, 1961 7. Schaper W, Buchwald A, Hoffmeister HM, Ito BR: "Stunned" myocardium is a problem of energy utilization and not of energy supply. Circulation 72 (suppl III): 111-119, 1985 (abst) 8. Laster SG, Becker LC, Ambrosio G, Jacobus WE: Reduced aerobic metabolic efficiency in the stunned myocardium. Circulation 74 (suppl II): 11-354, 1986 (abstr) 9. Dean EN, Annesley T, Underwood T, Nicklas JM: The oxygen consumption paradox of stunned myocardium. Clin Res 33: 176A, 1985 (abst) 10. Laxson D, Homans DC, Bache RJ: Myocardial blood flow and oxygen consumption in stunned myocardium. J Am Coil Cardiol 9: 125A, 1987 (abst) 11. Sako EY, Kingsley-Hickman PB, St. Cyr JA, Andreone PG, From AHL, Ugurgil K, Foker JE: Effect of ischemia and dobutamine on myocardial ATP production. Circulation 74 (suppl II): II-68, 1986 (abst) 12. Krukenkamp IB, Silverman NA, Sorlie D, Pridjian A, Feinberg H, Levitsky S: Characterization of post-ischemic myocardial oxygen utilization. Circulation 74 (suppl III): 111-125, 1986 13. Kusuoka H, Porterfield JK, Weisman HF, Weisfeldt ML, Marban E: Pathophysiology and pathogenesis of stunned myocardium. Depressed Ca2+ activation of contraction as a consequence of reperfusion-induced cellular calcium overload in ferret hearts. J Clin Invest 79: 950, 1987 14. Hoerter JA, Miceli MV, Renlund DG, Jacobus E Gerstenblith G, Lakatta EG: A phosphorus-31 nuclear magnetic resonance study of the metabolic, contractile, and ionic consequences of induced calcium alterations in the isovolumic rat heart. Circ Res 58: 539, 1986 15. Theroux P, Ross J Jr, Franklin D, Covell JW, Bloor CM, Sasayama S: Regional myocardial function and dimensions early and late after myocardial infarction in the unanesthetized dog. Cire Res 40: 158, 1977 16. Weiss HR, Neubauer JA, Lipp JA, Sinha AK: Quantitative determination of regional oxygen consumption in the dog heart. Circ Res 42: 394, 1978 17. Grover GJ, Tierney MA, Weiss HR: Beta adrenoceptor control of 872 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. the microvascular reserve in rabbit myocardium. J Pharmacol Exp Ther 238: 868, 1986 Weiss HR, Conway RS: Morphometric study of the total and perfused arteriolar and capillary network of the rabbit left ventricle. Cardiovasc Res 19: 343, 1985 Weiss HR, Buchweitz EB, Murtha TJ, Auletta M: Quantitative regional determination of morphometric indices of the total and perfused capillary network in the rat brain. Circ Res 246: 494, 1982 Cohan G, Gewertz BL: Measurement of myocardial oxygen consumption. J Surg Res 38: 305, 1985 Conway RJ, Weiss HR: Role of propranolol in improvement of the relationship between 02 supply and consumption in an ischemic region of the dog heart. J Clin Invest 70: 320, 1982 Weiss HR, Sinha AK: Regional oxygen saturation of small arteries and veins in the canine myocardium. Circ Res 42: 119, 1978 Sinha AK, Neubauer JA, Lipp JA, Weiss HR: Blood 02 saturation determination in frozen tissue. Microvasc Res 14: 133, 1977 Buckberg GD, Luck JC, Payne BD, Hoffman JIE, Archie JP, Fixler DE: Some sources of error in measuring regional blood flow with radioactive microspheres. J Appl Physiol 31: 598, 1971 Vinten-Johansen J, Weiss HR: Oxygen consumption in subepicardial and subendocardial regions of the canine left ventricle. The effect of experimental acute valvular aortic stenosis. Circ Res 46: 139, 1980 Edoute Y, van der Merwe E, Sanan D, Kotze JCN, Steinman C, Lochner A: Normothermic ischemic cardiac arrest of the isolated working rat heart. Effects of time and reperfusion on myocardial ultrastructure, mitochondrial oxidative function, and mechanical recovery. Circ Res 53: 663, 1983 Krause S, Hess ML: Characterization of cardiac sarcoplasmic reticulum dysfunction during short-term, normothermic, global ischemia. Circ Res 55: 176, 1984 Myers ML, Bolli R, Lekich RF, Hartley CJ, Roberts R: Enhancement of recovery of myocardial function by oxygen free-radical scavengers after reversible regional ischemia. Circulation 72: 915, 1985 Przyklenk K, Kloner RA: Superoxide dismutase plus catalase improve contractile function in the canine model of the "stunned myocardium". Circ Res 58: 148, 1986 Gross GJ, Farber NE, Hardman HF, Warltier DC: Beneficial actions of superoxide dismutase and catalase in stunned myocardium of dogs. Am J Physiol 250: H372, 1986 Engler R, Covell JW: Granulocytes cause post-ischemic dysfunction following 15 minutes of myocardial ischemia. Circulation 74 (suppl II): 11-373, 1986 (abst) Stahl LD, Aversano TR, Becker LC: Increased flow selectively enhances function of post-ischemic stunned myocardium. Circulation 74: 843, 1986 Hori M, Inone M, Kitakaze M, Koretsune Y, Iwai K, Tami J, Ito H, Kitabatake A, Sato T, Kamada T: Role of adenosine in hyperemic response of coronary blood flow in microembolization. Am J Physiol (Heart Circ Physiol) 19: H509, 1986 CIRCULATION Myocardial oxygen consumption, oxygen supply/demand heterogeneity, and microvascular patency in regionally stunned myocardium. L D Stahl, H R Weiss and L C Becker Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017 Circulation. 1988;77:865-872 doi: 10.1161/01.CIR.77.4.865 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1988 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/77/4/865 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/