Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
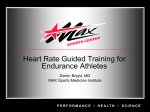
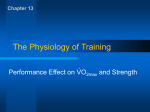
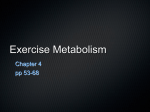
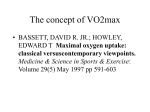
Lab II Maximal Oxygen Consumption (VO2max) In the previous lab we collected expired gas samples and evaluated them for their volume and their percent oxygen and carbon dioxide. We used these values, along with the environmental conditions, to calculate VO2 and a number of other, related variables (e.g. VCO2, RER, ventilator equivalent ratios, etc.). We also measured oxygen consumption during moderate intensity, steady state exercise in order to observe and calculate the O2 deficit and EPOC. In this lab we will measure oxygen consumption continuously during graded exercise tests performed on a variety of ergometers (mostly treadmill and cycle). In order to get good results, it will be necessary for all subjects to give a maximal effort. It is very important to tell your lab instructor if you have health conditions why you should not perform high intensity, maximal exercise. Maximal oxygen consumption and aerobic capacity The term VO2max is used to refer to the maximal rate at which oxygen can be consumed during maximal metabolic stress (exercise). VO2max correlates well with endurance performance (although there are other physiological measures that are better indicators of endurance performance). It also correlates well with many measures of physical fitness. There are a number of clinical conditions that compromise VO2max (e.g. heart failure, pulmonary disease) and thus compromise these patients’ exercise tolerance. VO2max values tend to be greatest if the exercise performed requires a large muscle mass; the great demand for oxygen by the large active muscle mass will also require great increases in cardiac output and ventilation, as well as a redistribution of blood from inactive to active tissues. Thus, exercises that use a smaller muscle mass will yield a smaller VO2max. This is one reason why one might use the term VO2peak rather than VO2max (it may not actually be a true maximal value due to the use of a small muscle mass). Review appendix pages 33-37, 4651, and 54 as you read and complete this lab. The term VO2peak is used for a number of other reasons. For example, if the test was not of progressively increasing exercise intensity, if the test was not performed until the subject’s maximal effort, or if VO2 was still increasing when the test was stopped, then the highest VO2 value recorded should be considered VO2peak not VO2max. In each of these scenarios there is no way to know if the subject reached their maximum possible value for VO2 , and that is why the term VO2peak is frequently used in these situations. As previously mentioned, VO2max is a good predictor of endurance performance (although anaerobic threshold and mechanical efficiency are also very important, see appendix page 51). The highest absolute VO2max values are typically observed in large endurance athletes (e.g. rowers), whereas the highest relative VO2max (when VO2 is reported relative to body mass) values are usually found amongst smaller endurance athletes (e.g. marathon runners). Are elite endurance athletes naturally endowed with high VO2max values, or are their high VO2max values due to their intense, high volume, training regimens? The answer is probably some of both. Most research suggests that VO2max can increase, on average, 10-20% with training. However, it appears that there is a great deal of variability in how much VO2max increases with training. Genetics may play a role in determining VO2max (and other physiological variables) by one of two general mechanisms: 1) an individual’s genetic composition may directly dictate their VO2max, or 2) an individual’s genetic composition may dictate how much they can increase VO2max with training. This may partly explain why there are such varying abilities to increase VO2max with training. Responders (people who respond well to training) can achieve up to 50% increases in VO2max with training. Non-responders, on the other hand, may not increase VO2max at all (0% increase) with training; even with a good training regimen and good compliance (it is worth noting that there are health benefits of Lab II - 1 exercise regardless of whether or not VO2max increases). Thus, it appears that heredity plays a major role in determining VO2max; most studies suggest that 25-50% of the general population’s variability in VO2max is due to genetic differences. Put another way, your VO2max is 25-50% determined by your genetic composition. If you want to be an outstanding endurance athlete, it is important that you choose your parents wisely! What sets the “limits” of VO2max for an individual? To answer this question it would be very helpful to consider two formulas from the previous lab: VO2 = VEstpd(NF x .2093 - FEO2) VO2 = Q x a-vO2difference (Fick Equation) Clearly, there are multiple possible answers, depending upon the individual. For example, a patient with a severe restrictive pulmonary disease may fail to increase VE as high as a subject without a pulmonary disease. Likewise, a patient with heart failure would have very low stroke volumes, which would reduce cardiac output and, thus, VO2max. Maximal heart rate, and thus maximal cardiac output tend to decrease with age, and thus tend to reduce VO2max with age. In each of these cases, there are, of course other contributions to the reduced VO2max values. These are just some of the clearest examples. What effect do you think anemia would have on VO2max? Could you explain your answer using the formulas above? These formulas can also help us understand why other species may have exceptionally good, or poor, VO2max values. For example, a dog has a very large heart relative to their body size (compared to humans) and they have maximal heart rates in the range of 260-300 bpm. Clearly they would have a very large cardiac output relative to their body size. Horses also have exceptionally large cardiac outputs and ventilations, but they have another neat mechanism that helps them increase VO2 during exercise. Horses have a large spleen that constricts during exercise, which increases their circulating hemoglobin concentration appreciably. This would increase their maximal a-vO2 difference and also increase their ability to extract oxygen from the air that they breathe. Hummingbirds can achieve heart rates in excess of 1,000 beats per minute, and their flight muscles have small fibers that are packed with a very large volume of mitochondria (perhaps exceeding 30% of the area of the fiber) and a large number of capillary contacts. How do you think absolute and relative VO2max values would compare for humans, horses, dogs, and hummingbirds given the information above? Can you relate your answers to the formulas above? What limits VO2max under more “normal” circumstances? Well, it is generally agreed that if an exercise bout requires greater than 50% of a subject’s muscle mass, then the ability of the muscles to dilate blood vessels and use the oxygen are greater than the ability of the heart and circulatory system to deliver the oxygen. Thus, oxygen delivery to the muscle, which is dependent upon cardiac output, an adequate blood pressure, hemoglobin concentration, and oxygenation of that hemoglobin are all candidates. It is also telling that inter-individual differences in VO2max appear to largely reflect differences in maximal cardiac output. Any two subjects of a similar age would be expected to have similar maximal heart rates, so interindividual differences in maximal stroke volume explain much of the difference in VO2max between subjects. Furthermore, exercise training tends to increase blood volume (which increases venous return) and ventricular chamber size, which increase end diastolic volume, and thus stroke volume. This is a, if not the, major mechanism by which young, healthy subjects increase VO2max with exercise training. Increases in capillarity, mitochondria, and oxidative enzyme content also facilitate improvements in VO2max with training. Lab II - 2 Testing Aerobic Capacity/Maximal Oxygen Consumption (VO2max) When designing a "VO2max test”, several factors should be taken into account. First, the test must be of progressively increasing exercise intensity (e.g. a graded exercise test), and the test should last until the subject can not maintain the required workload (fatigue). Second, the test should utilize a large muscle mass and/or be as sport specific as possible. Sport specificity is very important when testing athletes and sport-specific tests will provide the best and most important information to the athlete and coach. Thus, for most people the focus should be on using an ergometer that utilizes a large muscle mass, but for athletes a sport specific test is more important. Third, the test should ideally last 8-12 minutes, although valid results have also been attained using shorter or longer tests. Tests longer than 12 minutes will often end due to fatigue, without attaining maximal values for VO2. Once the test is complete, how do you know if you can consider the test a valid test for the determination of VO2max? In order for the highest VO2 recorded during an incremental (graded) exercise test to be considered VO2max, certain criteria should be met. Different labs may set different criteria because different labs may have different circumstances. The following is a list of commonly used criteria for determining if the test can be considered valid for the determination of VO2max . In this lab, if three of these five are met, then the greatest VO2 recorded can be recorded as a "maximal" value (VO2max). Otherwise, the greatest VO2 recorded should be considered a "peak" value. Criteria for a Valid VO2max test 1) A "plateau" in VO2 with an increase in workload. Because VO2 does not usually plateau for all subjects, it has been suggested that if VO2 increases by 0.15L/min with an increase in workload, this can be considered a "plateau", or leveling off, of oxygen consumption. Even though this criteria is not always it, it is the ideal criteria for considering the test valid for the determination of VO2max. 2) An RER of 1.1 or greater. This indicates that the exercise intensity was great enough to require some respiratory buffering of the blood, and thus suggests that the test was not ended due to lack of subject motivation. This does not rule out the possibility that the subject quit before reaching their true maximal intensity, rather, it just demonstrates that the subject was "working hard". 3) A blood lactate concentration 8.0 mmol/L. This also is used to demonstrate that the exercise was of sufficient intensity that you can rule out poor subject motivation as a reason for stopping the test. Resting blood lactate is around 1mmol/L. 4) Attainment of age predicted HRmax within 10 beats/min. This also indicates sufficient intensity, and is probably a better indicator of maximal effort than lactate or RER, because HRmax correlates very well with VO2max (for example the age related decline in VO2max correlates well with, among other variables, the decline in HRmax). 5) An RPE of 18 or greater. This is highly subjective, but it also indicates that the subject "felt" like they were near their maximum effort. Because VO2max is used so frequently as an indicator of fitness, there are a number of field tests for estimating VO2max. This is noteworthy also because not every facility has the equipment needed to measure oxygen consumption. A few examples of these tests are the YMCA cycle ergometer test, the Astrand-Rhyming test, and the Cooper Aerobic Tests. These tests for estimating VO2max mostly depend upon a few important relationships: a positive linear relationship between heart rate and VO2, between VO2 and Workload, and between workload Lab II - 3 and heart rate. Each of these tests also may require other assumptions, such as a predicted maximal heart rate based on age (e.g. HRmax = 220-age). While not as accurate, these tests do allow for an estimate of VO2max without expensive equipment, frequently more than one person can be tested at a time, many do not require a maximal effort (so there is less risk if working with patient). These tests are usually sensitive to changes in fitness with training and thus can be used to update your subject’s exercise prescription in a timely and safe, but still scientific, manner. Figure 1. Pulmonary & metabolic responses during a graded exercise test. Lab II - 4 Pulmonary and Metabolic Response to Exercise During a graded exercise test, oxygen consumption (VO2) goes up linearly with increases in exercise intensity. In order to increase VO2, it is necessary to increase pulmonary ventilation (VE). In the transition from rest to exercise we also tend to extract more oxygen from the air that we breathe (FEO2 decreases), which also helps to increase oxygen consumption. The increase in oxygen consumption during exercise reflects an increase in the metabolic demand of the activity. When fats and carbohydrates are being oxidized, some amount of CO2 is produced, and needs to be removed from the tissues and body. Thus VCO2 also increases during exercise. However, increases in VCO2 during high intensity exercise are also quite great in order to help buffer the blood (see discussion of ventilator threshold below). Pulmonary or minute ventilation (VE) is the product of TV and the respiratory frequency: VE = F x TV. The regulation of pulmonary ventilation at rest is dependent on a complex interaction of physical and chemical factors. Any changes in PCO2, PO2, pH and many other factors affect respiration either through direct stimulation of the respiratory control centers in the lower brain or by specialized receptors found in the large arteries. Proprioreceptors, thermoreceptors, nocireceptors, and lung stretch receptors also send information to the respiratory control centers and can play a role in modulating ventilation during exercise. The rate and strength of respiratory muscle contraction, and therefore the rate and depth of respiration, are controlled by medullary respiratory centers (dorsal and ventral respiratory groups) located in the medulla oblongata at the base of the brainstem. The dorsal respiratory group functions as the primary controller of inspiration, although the pre-Bötzinger complex is now generally thought to be the breathing “pacemaker” under resting conditions. The dorsal respiratory group stimulates initiates inspiration by stimulating the phrenic nerve, which, in turn stimulates the diaphragm. The ventral respiratory group functions in control of both inspiration and expiration; especially when there is a great ventilatory demand (e.g. exercise). In addition to the medullary respiratory centers, there are also two pontine centers: the pneumotaxic and apneustic centers located anterior to the medulla in the pons, which help control both the rate and pattern of breathing. The primary centers in the medulla are inherently rhythmic. Their activity alternates to produce inspiration and expiration. During normal quiet breathing at rest, the inspiratory center (dorsal respiratory group) acts to produce an active inspiration. The expiratory center limits and then inhibits the inspiratory center to produces a passive expiration. During exercise or other situations when the respiratory depth increases, both inspiration and expiration are active processes controlled by their respective medullary centers. The cerebral cortex also plays a couple of important roles in the regulation of respiration. For example, prior to and at the onset of exercise ventilation increases very rapidly, in part because of information from the motor cortical regions being sent to the medullary respiratory centers. During certain activities one may also need to subject rate and depth of breathing to voluntary control, such as during swimming. This is only possible because of motor cortical involvement in the regulation of respiration. Respiratory rate (frequency) and depth are adjusted according to the body's needs. The respiratory centers receive inputs from the higher brain centers (e.g. pons, cerebellum, cerebral cortex) and from peripheral receptors such as chemoreceptors in the aortic and carotid bodies, proprioreceptors in the joints, muscles, and tendons, and somatic sensory receptors for pain and thermal stimuli. Cerebral cortical control (voluntary) of the medullary centers can be observed when there is a modification in the respiratory cycle (change in breathing) as one attempts to perform a precise movement with the hands. Other modifications of the respiratory cycle involve feedback excitation of respiratory center activity in response to a variety of stimuli, such as changes in the chemical composition of the blood, especially its concentrations of carbon dioxide, hydrogen ions, and to a much lesser extent, oxygen. Lab II - 5 Both the depth and the rate of breathing contribute to the increase in ventilation during exercise (see appendix), and are necessary in order to increase oxygen consumption during exercise (as are several cardiovascular adjustments that occur during exercise). Most of the increase in VE that occurs at the onset of exercise is a result of increased tidal volumes. As you learned previously, increasing tidal volume has a greater impact on increasing alveolar ventilation than increasing respiratory rate. At higher intensities when tidal volumes are about as high as they can go, further increases in ventilation need to be accomplished by increasing respiratory rate. What are the benefits of increasing tidal volume vs. increasing respiratory rate? Lets take a look at an example to help us answer this question. Both subjects have the same VE, so what is the difference? Subject 1. TV 1000 ml, RR 50 br/min, DS 150 ml VE = TV x RR = 50 L/min VA = (TV-DS) x RR = 42.5 L/min Subject 2. TV 2000 ml, RR 25 br/min, DS 150 ml VE = TV x RR = 50 L/min VA = (TV-DS) x RR = 46.25 L/min Looking at the data for subject's 1 and 2 above, it is clear that VA will be greater if the subject increases their ventilation by increasing depth of breathing rather than by increasing breathing frequency. Furthermore, a greater VA would allow for better gas exchange. Thus, oxygen extraction would be better and we would not need to ventilate as much for a given oxygen consumption. Thus, at the onset of exercise it makes sense that we usually see a rapid increase in TV (depth of breathing) and only small increases in respiratory rate to increase ventilation. It is usually only at higher intensities that we need to rely on large increases in breathing frequency to increase ventilation. It is worth noting that ventilation increases even before the onset of exercise (anticipatory rise in ventilation). This is a result of greater cortical stimulation of the respiratory centers as the subject prepares to exercise. The rapid increase in ventilation at the onset of exercise precedes significant changes in chemical composition of the blood, so it is not mediated by chemical changes in the blood. This rapid increase in ventilation has two principal sources: receptors in the muscle, and the motor regions of the cortex both sending information to the medullary respiratory centers. Finally, at low and moderate intensities the subject will reach a relatively steady (steady state) ventilation. Fine tuning of the ventilation once it is relatively steady is modulated by the various chemoreceptors. During high intensity exercise, ventilation will never reach a steady state, even if the intensity is constant. Instead the ventilation will have a continuous, slow increase in VE. This is because there will be continuous changes in the chemical composition of the blood (especially CO2, pH, K+, and depending on the conditions, O2) and the temperature in the body. It is important to begin learning typical resting and exercise ventilation values. Normal resting tidal volumes are reported to be 300-800ml/breath (usually around an average of 500ml/breath) and resting breathing frequencies usually vary between 12-20 breaths per minute. Thus resting VE is usually 4-16 liters/min. Respiratory rate is a sensitive indicator of approaching exhaustion. For most people a respiratory rate over 50 breaths/min indicates a severe physical stress. Some endurance athletes, however, most notably large elite oarsman, are able to attain and maintain respiratory at rates above 75 breaths/min for several minutes. Combine this with tidal volumes in excess of 3500ml and they are able to achieve maximal Lab II - 6 exercise VE values that are well over 250 liters/min. On the other hand it is extremely difficult for many normal people to reach a VE of 100 liters/min. Fig 2. Pulmonary responses during a graded exercise test. At rest, FEO2 is somewhat high as we do not need to extract a lot of oxygen to adequately saturate hemoglobin with oxygen and meet the body’s oxygen demands. However, as we make the transition from rest to exercise, we begin to extract O2 better and FEO2 decreases. This is because of increases in alveolar ventilation (especially large increases in TV) and because of better gas exchange in the tissues (better extraction of oxygen by the tissues), resulting in a more favorable concentration gradient for oxygen diffusion in the alveoli. Because Lab II - 7 these changes are generally improving gas exchange, FECO2 also increases at this time. As we make the transition from moderate intensity exercise to high intensity exercise, however, FEO2 will eventually begin to increase and FECO2 will begin to decrease. The total volume of O2 consumption and CO2 production are still increasing, but exchange is less efficient. This is likely related to the fact that air is moving very rapidly in and out of the lungs (high VE) and blood is moving very rapidly through the alveolar capillaries (cardiac output is very high), resulting in less time for diffusion of O2 and CO2. Hyperventilation is a common occurrence for most subjects immediately prior to the start of an exercise test (e.g. see anticipatory rise in ventilation above). If the subject is hyperventilating prior to exercise, then VE will, of course, be high. This also means that the subject is blowing off CO2 faster than their cells are producing it, resulting in VCO2 values that are elevated above normal. This also tends to cause a mild degree of respiratory alkilosis. VO2 is influenced a little by hyperventilation in that the respiratory muscles do require oxygen. However, much of the increase in VE is offset by reduced O2 extraction, and FEO2 is somewhat high. The elevated VE and VCO2 values during hyperventilation result in elevated VE, RER, and ventilatory equivalent ratios. Once exercise starts all of these variables tend to normalize. During a graded exercise test, the respiratory exchange ratio tends to start a little high, as the subject is blowing off CO2 faster than their cells are producing it (resulting in relatively high VCO2). After this hyperventilation, VE and VCO2, and thus RER, for the most part normalize for a period of time, and thus RER again provides some insight into fuel substrates being used by the subject. At low intensities a great deal of fats are used to meet the muscle’s energy demands. With progressively increasing intensities, there is a tendency to rely more on carbohydrates. Thus, during a graded exercise test there is a general trend for RER to increase as a function of exercise intensity. However, beyond the anaerobic threshold, the respiratory system plays a role in buffering the blood. This will result in a greater rate of increase in VCO2 and will thus increase RER at an even faster rate. It is fairly common, and even expected, to observe RER greater than 1.1 towards the end of a graded exercise test. Ventilatory Threshold Oxygen consumption increases linearly during exercise of progressively increasing exercise intensity. Oxygen consumption eventually should plateau once the subject reaches their maximal oxygen consumption (VO2max). Minute ventilation also increases in a linear fashion up to approximately 60% of VO2 max (for an average subject). However, beyond this point, VE increases at a relatively higher rate (see appendix). This is because beyond this point ventilation plays an important role in buffering the blood in addition to its role in increasing oxygen consumption. This increase in ventilation allows the subject to blow off more carbon dioxide, and thus maintain pH of the extracellular fluids. The intensity where VE begins to go up out of proportion to the increase in exercise intensity is called the ventilatory threshold, and is considered by many to be a good indicator of the anaerobic threshold. The VCO2 also increases at this time. Because VE is now increasing at a faster rate than VO2, the ventilatory equivalent ratio for oxygen (VE/VO2) is also going up. Because the rate of increase in VE and VCO2 increase at the same time, the ventilator equivalent ratio for CO2 (VE/VCO2) remains constant (at least for a short time). The “anaerobic threshold”, whether it is determined by blood lactate analysis or by the ventilatory threshold, appear to be good predictors of the intensity that can be sustained for long periods of time, and thus are considered good predictors of endurance performance. The anaerobic and ventilatory thresholds will be discussed in greater detail in the anaerobic metabolism labs. Lab II - 8 Other Measures/Indicators of Exercise Intensity: Power Output, Heart Rate, and RPE Maximal power outputs of humans are influenced by several factors, including training, body size, age, gender, and the size of muscle mass being used to perform the exercise. In one study performed here at OU several years ago, maximal power outputs on a cycle ergometer for healthy college age males and females were in the range of 270-360 watts and 180-270 watts, respectively. On the other hand, trained cyclists may have maximal power outputs over 450 watts, which can only be maintained for brief period of time. Elite cyclists, such as those who compete in the Tour de France may average intensities near 400 Watts for several hours. One striking example of how body size and training influence maximal power output is the fact that some elite rowers can maintain over 500 watts for almost 6 minutes during a simulated 2000meter race (that is over 2/3 horsepower!). Most humans, however, can not maintain such high power outputs for a significant period of time. For example, later this quarter we will be performing Wingate tests on a cycle ergometer. It is not uncommon for larger male subjects in our labs to reach over 1,000 Watts! However, these subjects generally only maintain these high values for one or two seconds. Like maximal power output, the power output that subjects can maintain during a workout is dependent on body size, training, gender, and several other factors. The following table shows approximate power values at various intensities for individuals of average fitness and size, assuming that they are performing exercise that uses a moderate to large muscle mass. Table 2. Power output and intensity Low intensity Moderate intensity High intensity Power (Watts) 50-75 Watts* 90-150 Watts* >175 Watts* *It is important that you understand that these values would most likely be higher if the subject were large or well trained and would most likely be lower if the subject were either small or unfit. Additionally, if a subject is using a small muscle mass, such as during arm crank exercise, 50 to 75 Watts would likely be a moderate or even a high intensity depending on the subject. Heart rate is linearly related to work load and oxygen consumption and therefore is a good indicator of the relative stress of the exercise. In an average adult at rest, heart rate is approximately 70 beats per minute (bpm). Resting heart rate may be lower in well trained individuals as a result of higher resting activity of the parasympathetic branch of the autonomic nervous system. The parasympathetic nerves that innervate the SA node, the pacemaker of the heart, release the neurotransmitter Acetylcholine. At rest the parasympathetic branch of the autonomic nervous system is dominant. Exercise is a potent stimulator of the sympathetic branch of the autonomic nervous system. This system is associated with our "fight and flight" reflexes (preparing the body to fight or run away from a potentially harmful situation). The sympathetic nervous system stimulates an increase in heart rate during exercise by releasing the neurotransmitter norepinephrine at the SA node. The reason why we need to increase heart rate during exercise is that there is an overall increase in whole body metabolism, and thus more oxygen is needed by our tissues (especially skeletal muscle). Thus it should not surprise you that heart rate and oxygen consumption during exercise are linearly related. Maximal exercise heart rates can be approximately calculated from the equation HRmax = 220 - age (in years). Thus, a 20 year old would be expected to have an age-predicted maximal heart rate of 200 bpm. Keep in mind this formula provides only a very rough estimate of HR maximum. Lab II - 9 Students may also recall from previous physiology courses that a subject’s cardiac rhythm is called bradycardia if the heart rate is lower than 60 bpm and is called tachycardia if the heart rate is higher than 100 bpm. The RPE, or Rating of Percieved Exertion scale is used as a psychophysiological indicator of the relative intensity of the exercise. It allows the subject to give an indication of how hard the exercise is for them. The scale has a linear relationship with exercise intensity (and therefore a linear relationship with heart rate). During exercise the subject is asked to rate the overall intensity of the exercise according to the written descriptions on the number scale (which goes from 6 to 20 on the Borg Scale). Although the scale may take some practice for the subject to use, it can be useful for exercise testing and training. Additionally, RPE can be used in combination with other data (e.g. heart rate) to determine the appropriate intensity for training. Some expected Normal Values Rest VE 4 -15 L/min Absolute VO2 (men) 0.2 - 0.5 L/min (women) 0.15 - 0.4 L/min Relative VO2 (men) 3.5 ml/kg.min (women) 3.5 ml/kg.min VO2max for average college age: Male: Female: RER 0.7 to 1.0 FEO2 0.15 to 0.18 FECO2 0.025 to 0.06 Lab II - 10 Maximal Exercise 130-250 L/min 2.0 - 7.0 L/min 1.5 - 5.0 L/min 35 - 90 ml/kg.min 25 - 75 ml/kg.min 45 ml/kg.min 35 ml/kg.min 1.0 to 1.5 same as rest range same as rest range VO2max procedures ALL STUDENTS will perform VO2max tests using a semi automated analysis system. However, if the student has any health condition that precludes performing maximal exercise, a submaximal test may be used. If a student has a health condition that increases their risk of adverse events during high intensity or maximal exercise, the student MUST TELL THEIR INSTRUCTOR. Students will be provided with a sheet that states what exercise protocol you will be using. Following the test students will be given a printout of their VO2max test results. ALL STUDENTS will graph the results of their own VO2max test plotted against time (put time on the x-axis) using Microsoft Excel (see appendix for help graphing with MS Excel). These graphs will be due one week after performing their test (see below for details). During the VO2max tests all students will be assigned a job to perform during the test. Some of these important roles include: running the metabolic cart, recording heart rate, changing treadmill speeds or cycle ergometer settings, recording RPE at the end of the test, and coordinating all of these jobs throughout the test (some students will need to play several of these roles simultaneously). Students should familiarize themselves with normal numbers and pulmonary responses during the test. Once your test is complete answser the questions below. Using the data from your VO2max test, Plot the following vs.Time (put time on the x-axis). Put each of the following variables on their own axis, and make sure that each graph is large enough that you can observe trends or changes in the shape of the lines/curves with respect to time during the test (that is, you can not put all 11 variables on the same graph). Data with similar values (e.g. VO2 and VCO2, VE/VO2 and VE/VCO2) can be put on the same graph if you like as long as trends are observable. When you make a graph it is important to label each axis and include what units the data are recorded in. Additionally, if there is more than once data set on the graph, a key must be provided. These graphs are due one week after performing your VO2max test. Variables to graph from your VO2max test: 1) Power in Watts (you will need to calculate these) 2) VO2 3) VE 4) RER 5) VCO2 6) VE/VO2 7) VE/VCO2 8) FEO2 9) FECO2 10) Heart Rate 11) O2 pulse Regarding your VO2max test: 1) Graph all variables of the above listed variables on Microsoft excel. 2) Briefly, explain why these variables follow these trends (increase, decrease, stay the same) as exercise intensity increased throughout the test. Lab II - 11 3) Were your absolute and relative VO2max values in the expected range? How about maximal VE values? (see table from lab 1) 4) What happened to RER during your VO2 max test? What do these trends and values suggest about metabolism, hyperventilation, and buffering of the blood? 5) What happened to FEO2 and FECO2 during the test? What do these trends suggest about gas exchange in the transition from rest to exercise and from moderate to high intensity exercise? 6) Did you have a plateau in VO2? 7) Was your test valid for the determination of VO2max? ? If not give possible explanations why? What criteria did you meet? What criteria didn’t you meet 8) What happened to TV, RR, and VE during the test? Did these values reflect the expected trends? 9) Can you identify your ventilator threshold (VT)? (Note: it will be easier to identify after you have graphed VE, VCO2 and ventilator equivalent ratios). If so, at what time did it occur? What power output, heart rate, and VO2 correspond to this point? 10) At what percent of VO2max (peak) did your VT occur? Lab II - 12 Lab II study questions 1) What happens to FEO2 and FECO2 at the beginning, during the middle, and at the end of a progressive intensity exercise test? Explain why? 2) What are characteristics that should be taken into account when designing a VO2max test? 3) What are the major criteria that can be used to determine if VO2max has been achieved during a test? Why do we use these criteria? 4) What are the differences between VO2max and VO2 peak? 5) What happens to TV, RR, and VE during a graded exercise test? What is the benefit of these responses in TV and RR when considering gas exchange? 6) What factors are involved in regulation of respiration at rest and during exercise? What parts of the central nervous system are responsible for taking in this information and making the appropriate adjustments? 7) What happens to VE/VO2 at the beginning, during the middle, and at the end of a progressive intensity exercise test? Explain why? Lab II - 13 8) What does the ventilator threshold repreent? What other concepts in exercise physiology is it related to? How can you identify it? 9) How is the ventilator threshold related to buffering of the blood? 10) During a graded exercise test, stroke volume usually increases and eventually plateaus. What would you expect to happen to O2pulse during a VO2max test? 11) Endurance athletes usually have higher VO2max values than untrained individuals. Using the formulas from the question above to help you with your answer, what physiological variables do you think are likely to be responsible for the higher VO2max values in endurance trained individuals? Explain your answers. 12) List three clinical conditions that you would expect to influence VO2max and indicate, using the formulas that we have used from the last two labs, why these diseases/conditions influence VO2max. 13) List three animals that either have very high, or very low VO2max values and indicate, using the formulas that we have used from the last two labs, why these animals have very high/low VO2max values. 14) What would you expect to happen to VO2max with aging? Use the formulas that we have used from the last two labs to explain your answer. Lab II - 14