Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
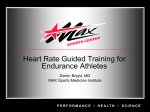
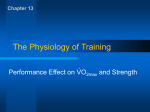
Aerobic Exercise Testing Maximal laboratory measurement & estimation protocols Learning Objectives • • • • Discuss the importance of test characteristics: validity, reliability and applicability in normal populations and in clinical settings. Explain the components of fitness and performance with reference to basic principles of physics and physiology. Explain the rationale of named test protocols and discuss the acute physiological responses to testing. Explain and use fitness testing equipment and apply the principles of quality assurance. Outline • • • • • • • Introduction Terminology Common protocols Exclusion criteria Test termination criteria Interpretation of results Practical and DAI Terminology • • • • • Graded Exercise Test (GXT) Aerobic Power Aerobic Capacity - (VO2max) Aerobic Capacity - (VO2peak) Relative & Absolute (VO2) Terminology • Direct assessment: via pulmonary gas exchange – ‘Measurement’ • Indirect assessment – ‘Estimation’ based on work output What are we testing? What are we testing? Cycle Protocols • Aim: Reach max within 8 – 10 min ? • Predict VO2max: – 0.025(ht) – 0.023(age) – 0.542(sex) + 0.019(mass) +0.15(LEI) - -2.32 L∙min-1. • • • • Predict work rate: VO2 = 10 ml∙min-1 x W-1 + 500 ml Initial W = 100 Increments 50 W∙3 min = 12 min test Treadmill Protocols • • • • • • Bruce Modified Bruce Balke Naughton All incremental and continuous Discontinuous protocols used mainly in athletes The Bruce Protocol (1973) Standard Bruce The Modified Bruce Patient Preparation • Par-Q • Written Informed Consent • Test Briefing – Protocol – RPE – Signals – What to do if things go wrong • Practise treadmill walking The Test • Start – Position feedback – Hand position – Stride, gait and posture • End of each stage – RPE – Signal – Encouragement VO2max Achievement Criteria • A plateau in your VO2 with increased workload. VO2peak Achievement Criteria • • • • HR within 10 beats or 85% of Max-est BLac of 8 or 10 mmol∙l R > 1.15 or 1 Failure of VO2 to increase – Based on estimate from last stage (inappropriate) Recovery • Cool down – 3 to 5 min / HR & BP return to recommended levels – keep subject moving and monitor condition – Caution: problems often occur during recovery • ECG? - Take rhythm strip at the end of each recovery minute • Take blood pressure at 1, 3, 5 minutes into recovery – Note the condition of the patient and abnormalities on the EKG monitor Recovery • Verbally ensure the subject in doing well and has recovered from the test • Disconnect the subject • Advise subject – showering, – daily activity, – avoiding extreme temperatures ACSM Absolute Indications • • • • Suspicion of a myocardial infarction or acute myocardial infarction (heart attack) Onset of moderate/severe angina (chest pain) Drop in SBP below standing resting pressure or with increasing workload accompanied by signs or symptoms Signs of poor perfusion ACSM Absolute Indications • Severe or unusual shortness of breath • CNS (central nervous system) symptoms – ataxia , vertigo, visual or gait problems, confusion) • Serious arrhythmias – second / third degree AV block, atrial fibrillation with fast ventricular response, increasing PVCs, sustained VT) • Technical inability to monitor the ECG • Patient's request (to stop) ACSM Relative Indications • Any chest pain that is increasing • Physical/verbal manifestations of – shortness of breath – severe fatigue • Wheezing • Leg cramps or intermittent claudication (grade 3 on a 4-point scale) • Hypertensive response – (SBP >260 mm Hg; DBP>115 mm Hg) ACSM Relative Indications • Pronounced ECG changes from baseline • >2 mm of horizontal or down sloping STsegment depression, or >2 mm of ST-segment elevation (except in aVR) • Exercise-induced bundle branch block that cannot be distinguished from ventricular tachycardia • Less serious arrhythmias (abnormal heart rhythms) such as supraventricular tachycardia Interpretation and Exercise Prescription • Calculate VO2max and METS. Determine: exercise training intensity heart rate, RPE, or METs • Have physician interpret ECG recordings • Consult subject – review test results – exercise prescription – monitor outcome and behavioural changes Measuring or Estimating VO2max • Measurement - values • Estimation • Males & Male CHD – VO2max = 14.76 - 1.379 (T) + 0.451 (T^2) 0.012 (T^3) • SEE 3.35 ml.kg-1.min-1 • With Handrail Support – VO2max = 2.282 (T) + 8.545 • SEE 4.92 ml.kg-1.min-1 Estimating VO2max • Women: – VO2max = 4.38 (T) - 3.90 • ±2.7 ml.kg-1.min-1 • Prediction equations – http://www.exrx.net/Calculators/Treadmill.html • Full listings: – http://www.exrx.net/Testing/CardioTests.html Foster et al. MSSE, 28(6):752-756,1996. Foster et al. MSSE, 28(6):752-756,1996. Metabolic Equivalents (METs) Calculating MET equivalents • 1 MET = 3.5 ml.kg-1.min-1 • Useful in exercise prescription and prognosis – http://www.exrx.net/Calculators/Treadmill.html Summary • Protocols • Measurement – Direct, gold standard • Estimation – Cost vs. accuracy • Utilisation – Prescription, Assessment and Prognosis References. • Myers et al. The New England Journal of Medicine 346:14:11-16, 2002. • Sui et al. J Am Geriatr Soc 55:1940–1947, 2007.