Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
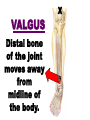
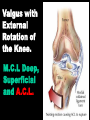
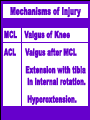
KNEE INJURIES • Review Gross and Functional Anatomy. • Discuss traumatic injuries to the knee. • Discuss overuse injuries in and about the knee. KNEE INJURIES • Discuss the signs and symptoms of the specific injuries. • Discuss causes and treatments. KNEE (Anterior view) BEHAVIORAL CHARACTERISTICS OF STRUCTURES AROUND THE KNEE ANTERIOR CRUCIATE LIGAMENT LOCATION POSTERIOR CRUCIATE LIGAMENT LOCATION STABILIZING ROLE OF THE ANTERIOR CRUCIATE LIGAMENT HEAT SENSITIVE VIEWS OF THE ANTERIOR CRUCIATE IN FLEXION STABILIZING ROLE OF THE POSTERIOR CRUCIATE LIGAMENT HEAT SENSITIVE VIEW OF THE POSTERIOR CRUCIATE IN FLEXION AND EXTENSION A.C.L. and P.C.L. LINKAGE MEDIAL COLLATERAL LIGAMENT DURING FLEXION AND EXTENSION LATERAL VIEW OF KNEE FLEXION and EXTENSION PATELLO-FEMORAL JOINT DURING FLEXION AND EXTENSION NORMAL KNEE MOTION KNEE FLEXION-EXTENSION takes place between the bottom of the femur and the top of the menisci. TWISTING MOTION takes place between the bottom of the menisci and the tibia. MENISCUS OF THE KNEE Purpose: Equalize weight distribution across the knee joint. Shock absorption. Coronary Ligament Medial is tighter than the lateral. Thus, there is less mobility medially. MENISCAL INJURY Medial Meniscus: excessive external rotation of the tibia. Lateral Meniscus: excessive flexion of the knee. MECHANISMS OF INJURY VALGUS VARUS HYPEREXTENSION HYPERFLEXION INTERNAL ROTATION EXTERNAL ROTATION VALGUS Distal bone of the joint moves away from midline of the body. X Medial Support Complex Not Shown: Quads Medial Head of Gastrocnemius Medial Hamstrings X VARUS Distal bone of the joint moves towards the midline of the body Lateral Support Complex Not Shown: Poplitius Tendon Head of the Gastrocnemius Iliotibial Band Biceps Femoris M. ANTERIOR CRUCIATE ANTERIOR CRUCIATE Posterior Cruciate Ligament Impact on anterior tibia. Rotation Affecting Tension Valgus with External Rotation of the Knee. M.C.L Deep, Superficial and A.C.L. Mechanisms of Injury MCL Valgus of Knee ACL Valgus after MCL Extension with tibia in internal rotation. Hyperextension. PCL Valgus after MCL and ACL. Varus after LCL,ACL Hyperflexion with tibial internal rotation. Blunt trauma to tibial tuberosity. FCL Varus of knee. M.M. External rotation of the tibia. Valgus to knee. L.M. Hyperflexion of the knee. SIGNS AND SYMPTOMS OF LIGAMENT INJURY (Not all symptoms have to be present to indicate injury) • Immediate pain ++++ • Feeling of tearing. • Hearing unusual noises. …. 2. .. 2 Signs and Symptoms • Feeling of ‘giving way’. • Loss of function of the joint • Be cautious of the ‘painful’ and then ‘not very painful’ knee. REMOVAL FROM FIELD (Non-weight Bearing) Feeling of a tearing or popping in the knee. If pain, no pain. REMOVAL FROM FIELD (Non-weight bearing) If complaining of ‘not feeling right’ or feeling ‘funny’ REMOVAL FROM FIELD Weight bearing Minor pain with full R.O.M. Stand. Pain? Slowly walk off field with support. Return to play only after the athlete has been evaluated by a physician. Patello-femoral Pain Syndrome. Iliotibial Band Friction Syndrome. Osgoode Schlatter’s Disease. PATELLO-FEMORAL PAIN SYNDROME Causes: . Excessive Q angle. . Excessive pronation. . Weak plantar flexors/inv. . Weak V. Medialis/Tight Ham Q ANGLE (Quadriceps) Two lines; ASIS to MPP; the other from TT to MPP. Angle of intersection called ‘Q angle’. Q The greater the Q angle, the greater the tendency to move the patella laterally against the lateral femoral condyle. A large Q angle plus strong quad contraction can dislocate pat. Equal pressure distribution across the back of the patellae ensures proper nutrition by inbibition. Medial aspect of Patellofemoral Joint has hypopressure. Lateral aspect has hyperpressure. + - - + Signs and Symptoms of Patello-femoral Pain Syn. Painful crepitus of the knee. Locking, catching of knee. Swelling. Loss of strength. Activity worsens symptoms. SUGGESTED TREATMENTS • Strengthen Vastus Medialis. • Reduce Pronation. • Stretch Hamstrings, ITB, and Quads. • Modify activities. The greater the Q angle, the greater the tendency to move the patella laterally against the lateral femoral condyle. A large Q angle plus strong quad contraction can dislocate pat. “ My knee came apart and went back together again”. For example, “I was running forward, planted on my right foot, cut to my left and attempted to push off with my right”. SUBLUXED OR DISLOCATED PATELLA Lateral Medial DISLOCATED PATELLA If the patella is dislocated, slightly flex the hip and slowly extend the knee. Usually the patella relocates. If it does not, do not force the patella medial. There may be some associated fractures (back of the patella, lateral femoral condyle). MEDICAL Iliotibial Band Friction Syndrome I.T.B.F.S. Predisposing Factors Tight Tensor Fascia Lata and weak Gluteus Medius. Genu Varum Downhill Running Training Errors I.T.B.F.S. Treatment • Modification of Activity and shoes. • Stretching. • Icing after activity. • Strengthening. Iliotibial Band And Hip Abductor Stretch OSGOODE SCHLATTER’S DISEASE Osgoode Schlatter’s Separation of the traction epiphysis of the quadriceps muscle. Active pre-pubescent kids. No gender bias. Signs and Symptoms: Pain increase with activity. Tibial tubercle is warm to touch. Pain on squeezing the tibial tubercle from sides. • Inform parents. • Stop irritating activity. • Icing the tibial tubercle. • Stove-pipe casts are sometimes applied to ensure rest. • Return if asymptomatic.