Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
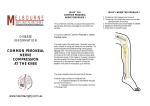
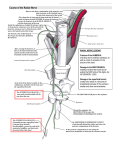
ENTRAPMENT OF THE SUPERFICIAL THREE JAMES From the Royal Entrapment cases cases of the decompression are KERNOHAN, Orthopaedic superficial Hospital, nerve peroneal of the nerve B. at the point REPORTS LEVACK, J. N. London, and is an unusual of exit in the superficial by Mr A. K. Henry nerve entrapment. be reproduced by pressing emerged the from from deep peroneal was nerve” the nerve at the point Case 3. where it fascia. pain, He which was had There incapacitated led him was the lower of pain fascia Hospital, in the Whitechapel ankle will produce and a good foot. In such result. Three A which valgus. Tinel’s sign history diminished leg and and to seek distracted many sensation dorsum was of the right by medical to light foot, strongly peroneal The nerve REPORTS A 39-year-old man presented with a six-year of pain in the right foot below and in front of the malleolus; his symptoms had started after patel- lectomy. The London 33-year-old woman presented with a nineof pain over the right lateral malleolus had developed after manipulation for hallux The pain was severe, but sensation was normal. month in 1945 to describe superficial He noted that the pain could CASE 1. WILSON cause the deep superficial Case history lateral NERVE described. “Mononeuralgia coined peroneal National CASE PERONEAL positive nerve in the was exposed over lower and freed a distance of several centimetres. and complete pain relief. the course of the leg. from There the fascia was for permanent the opinions. touch over with localised tenderness about 10 cm above the lateral malleolus. Percussing the tender area reproduced the pain. The superficial peroneal nerve was dissected and, where incised. it emerged through the deep fascia, This gave immediate and lasting the fascia relief. was Case 2. A 25-year-old woman presented with a 10-month history of pain in her right leg; this pain had developed after she had sprained her right ankle. The pain was mainly over the lateral and the dorsum over the distal about pain. side ofthe lower quarter ankle. There was a slight of the fibula, and percussing third 8 cm above the lateral malleolus Sensation was normal. (The patient been investigated at another hospital biopsy had been performed.) The nerve was explored and found it emerged ofthe of the under Decompression the produced crescent almost shin swelling a point reproduced the had previously where a tibial to be flattened of the immediate deep fascia. total relief of pain. Fig. as lateral J. G. Kernohan, FRCS Ed, J. N. Wilson, ChM. FRCS. Royal National Orthopaedic WIP 8AD. England. B. Levack, The London Requests for reprints should Editorial $2.00 malleolus. divides Registrar Surgeon Street, London As it emerges from into two branches. the fascia it DISCUSSION FRCS, Senior Orthopaedic Hospital, Turner Street, . 1985 British 0301-620X/85/1006 60 FRCS, Senior Orthopaedic Consultant Orthopaedic Hospital, 45-5 1 Bolsover 1 The common peroneal nerve is prominent behind the head of the fibula. The superficial peroneal nerve can be seen in the lateral compartment; it emerges through the deep fascia approximately one-quarter of the way up the leg from the be sent Society Registrar London El to Mr of Bone J. G. and _________________________________ Joint IBB, England. Kernohan. Surgery The superficial peroneal nerve the lateral one-quarter peroneal nerve arises from the common at the neck of the fibula and runs down compartment of the distance THE JOURNAL of the up the OF BONE leg. Approximately leg from the lateral AND JOINT SURGERY ENTRAPMENT malleolus, the nerve pierces into medial and intermediate (Fig. before I). The leaving the deep dorsal OF fascia, and cutaneous nerve may divide into the deep fascia (Romanes THE SUPERFICIAL PERONEAL 1981). divides nerves been these branches 1972). Direct injury ofthe reported (Tibrewal The supplied comprises skin the 61 NERVE nerve and in the lower Goodfellow third of the peroneal front of the dorsum of the foot (Fig. 2). Entrapment exit through the deep fascia causes loss. Retrograde Thompson cause pain 1963). may Pressure an increase in the the A not uncommon ankle. Occasionally due to a root be at at the level of the lower leg can should incident is a twist of are thought to be of the lumbar which a laminectomy may, mistakenly, (Banerjee and Koons 1981). A reliable diagnostic test is temporary the pain after injecting nerve leaves the deep and exit pain. precipitating the symptoms lesion the point of sensory (Kopell point radiating nerve leg and at the pain and a feature the also 1984). by the superficial distal leg has spine be for performed alleviation of lignocaine at the point where fascia. Operative decompression be expected to alleviate the the in pain permanently. We wish to thank the Department Surgeons of England, for allowing would also like to thank Mr Derek of Anatomy, Royal College the use of anatomical material. Sayers for the photographs. of We REFERENCES The superficial peroneal the skin of the great toe, toes, and the dorsum Kaushal et al. (1976) and reported peroneal nerve palsy direct Bianco injury and neuropathy fibular The distally, during MacCarty of total neck. peroneal nerve so forced inversion is and its fascial opening and Thompson VOL. I. JANUARY No. 1985 Rose et al. (1982) have at the knee caused by nerve taut against 1945; Kopell 67-B. Henry tethered at the proximally plantarfiexion and 1963; level can cause injury Banerjee and of and (Henry Koons Kaushal SP, following Kopell HP, Baltimore: Extensile 1945:296. Superficial exposure. peroneal 1981 ;55:991-2. Edinburgh Galante JO, McKenna total knee replacement. Thompson Williams WAL. and entrapment: London: R, Bachmann Clin Orthop Peripheral & Wilkins, 1963. textbook 1972. nerve E & S LivingF. Complications 1976; 121 : 18 1-7. entrapment ofanatomy. report neuropathies. 1 1 th ed. London: HA, Hood RW, Otis JC, Ranawat CS, Insall JN. Peroneal-nerve palsy following total knee arthroplasty: a review of the Hospital for Special Surgery experience. J Bone Joint Surg [Am] 1982; 64-A: 347-51. Stack RE, Bianco AJ Jr, MacCarty CS. Compression of the common peroneal nerve by ganglion cysts: report of nine cases. J Bone Joint Surg [Am] 1965;47-A:773-8. Rose the pull AK. stone, DD. J Neurosurg Romanes GJ, ed. Cunningham’s Oxford University Press, knee replacement. Stack, (I 965) reported compression peroneal the Banerjee T, Koons of two cases. nerve supplies the middle three of the foot. it Tibrewal SB, Goodfellow lower third of the leg. JW. Peroneal nerve palsy J R Soc Med 1984:77:72-3. at the level of the














![20 SCIATIC NERVE.IIppt[1].](http://s1.studyres.com/store/data/000476916_1-da0a7875960c02fecd474919cb5375ce-150x150.png)

