Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
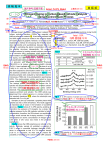
New Technologies and Challenges Targeted Therapies in Cancer Ian Olver MD PhD CEO The Cancer Council Australia Changing of the Guard There is a paradigm shift in the treatment of cancer Conventional cytotoxic drugs interact with DNA to prevent cell replication but are not specific to cancer cells We are moving to targeted therapies which specifically target cancer cells as evidenced by the many presentations at this meeting Side Effects of Chemotherapy Immediate Early Delayed Late Cardiotoxicity Lung fibrosis P. Neuropathy Hepatotoxicity Nephrotoxicity Second Cancer Encephalopathy Sterility Teratogenicity (hours - days) (days - weeks) (weeks- months) (months - yrs) Extravasation Emesis Hypersensitivity Tumour lysis Myelosuppression Mucositis Alopecia Cystitis Targeted therapies With targeted therapy the specific mechanism of action of the drug results in an increase in its therapeutic index However, the advantages of the specificity and safety of the are offset by the smaller number of susceptible tumour types Increasing numbers of these innovative and expensive anti-cancer drugs may exceed the capacity of the public purse to pay for them The Need to Identify the Target Appropriate use of newly approved and expensive targeted therapies for cancer first depends on the pathologist identifying the target for treatment in the tumour sample Currently the two major classes of targeted therapy are the small molecule tyrosine kinase inhibitors (TKIs) and monoclonal antibodies (mAbs) Potential mechanisms of Glivec Glivec may inhibit tyrosine kinases in many tumours, but this will be effective therapy only where tumour stem cells depend on these enzymes for survival, growth or metastasis Tyrosine kinases are part of the signalling pathways of cells which tell them to grow PET Before and after Glivec for GIST 7/12/00 9/1/01 STI 571 (Glivec) Specific inhibitor for BCR-ABL, PDGF receptor and c-kit tyrosine kinases produced by these genes which are responsible for growth in CML and GIST Effective in chronic myeloid leukaemia Effective in GIST Gastrointestinal stroma tumours which over express c-kit Side effects – Nausea, myalgia oedema, diarrhoea, myelosuppression, LFT’s early “storm” Monoclonal Antibodies Action of the mAbs, rituximab (Mabthera®) for NHL and trastuzumab (Herceptin®) for breast cancer depend on the targets CD20 expression and erbB2 gene being amplified and responsible for growth Rituximab Mabthera Mabthera is an Anti-CD20 monoclonal antibody for lymphoma CD20 is a protein on the surface of malignant lymphoma cells CD20 expressed on 90% of B-cells in lymphoma Mabthera Side effects include: – Infusion related fever, chills rigors – N + V, urticaria, pruritis, headache, fatigue, bronchospasm, hypersensitivity – Rare heart rhythm disturbance – Low blood counts for up to 30 days HER2 HER2 gene (neu, c-erb-2) ecodes a transmembrane gycoprotein receptor HER 2 is over expressed by 1/4 human breast cancer and correlates with poorer outcome MoAb against the receptor inhibits the growth of overexpressing cells HER 2 As a single agent 15% chance of shrinking metastatic breast cancer, 4% chance of a complete shrinkage in heavily pretreated patients Duration of response can be 9 months which is at least as good as single chemotherapy agents Can combine with chemotherapy Disease-Free Survival Romond H et al. Trastuzumab plus Adjuvant Chemotherapy for Operable HER2-Positive Breast Cancer NEJM 2005; 353:1673-1684 ACTH 87 ACT % % 85% 75% 67% N Events ACT 1679 261 ACTH 1672 134 HR=0.48, 2P=3x10-12 Years From Randomization B31/N9831 The Paradigm Shift The use of these drugs is giving clinicians a glimmer of the paradigm shift that will occur in the treatment of cancer One or several new targeted therapies offer the prospect of cancer being treated as a chronic disease. Brain Tumours The optimal use of temozolomide chemotherapy for the treatment of primary brain tumours may depend on knowing the DNA repair enzyme status of the tumour Hegi ME et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. New Engl J Med 2005; 352:997-1003 Dramatic response in female, non-smoking patient with Broncho-Alveolar Carcinoma Courtesy Dr T. Lynch, MGH Patient demographic factors associated with outcome in Gefitinib Phase II studies Gender – Females ORR 25% (CI 19-33%) – Males ORR 8% (CI 5-12%) Ethnicity – Japanese ORR 27% (CI 19-37%) – Caucasian ORR 11% (CI 6-19%) Smoking history – Non-smokers ORR 31% (CI 23-40%) – Smokers ORR 8% (CI 5-12%) Patient demographic factors associated with outcome in Gefitinib Phase II studies Histology – – – – – – Adenocarcinoma Squamous Undifferentiated Mixed Large cell Unrecorded n=275 n=75 n=35 n=26 n=11 n=3 ORR 19% ORR 7% ORR 3% ORR 4% ORR 9% ORR 0% EGFR Mutations and Response Lynch TJ et al New Engl J Med 350, May 20 2004 Hypothesis was that a mutation of EGFR accounts for the response of some patients with NSCLC to gefitinib They sequenced the entire coding region of EGFR in tumors from patients with a response to gefitinib and in tumors from those without a response Use of Molecular Methods Increase diagnostic accuracy and thereby improve prognostication Identify clinically distinct patient subsets to facilitate rational clinical trial design Help to optimize current treatments by increasing their specificity and improving their safety Identify signaling pathways that define cancer vulnerabilities and thus create drug targets Brown M, Buckley M, Rudzki B, Olver I. How can we turn cancer into a chronic disease that we can afford to treat? J Intern Med 2006 in press Practical Uses of Molecular Pathology and Targeting The decision to treat metastatic breast cancer depends on the state of the disease The need for additional treatment after surgery relies on predicting its behavior, which still relies on anatomic staging – Tumor size – Nodal status These are prognostic but not predictive of treatment outcome However hormone status and HER2 status have been shown to be both prognostic and predictive and we have had targeted hormonal therapy for decades Molecular Classification With technology that can rapidly measure multiple gene expression profiles it has been found that: – They correlate with microscopic observed difference e.g. one pattern of genes correlates with grade (Perou CM et al Nature, 2000, 406: letter 749-52, 2000) – They differ across tumors defined by hormone and HER2 status – Breast Cancer can be subtyped Sorlie T et al Proc Natl Acad Sci U S A. 2001, 98:10869–10874. 85 samples gene expression patterns analyzed by hierarchical clustering. Green is normal breast, red is the basal poor prognosis group Can use to predict prognosis and outcome of therapy and can target the therapy Conclusions Targeted therapies which improve the therapeutic index are the future of anti-cancer therapy Advances in molecular pathology will provide the means to identify the targets and will be used to subtype tumours and will provide predict response to therapy and provide prognostic information